
Abstract
Human immunodeficiency virus (HIV) infection prevalence in Pakistan has been increasing in high-risk groups, including people who inject drugs (PWID) and transgender hijra sex workers (TG-HSWs) nationwide. Effective control of HIV requires early diagnosis of the infection. We investigated recency of HIV infections in newly-diagnosed cases in PWID and TG-HSWs. This was an observational study with convenience sampling. Overall, 210 HIV-positive subjects comprising an equal number of PWID and TG-HSWs were included. Antibody avidity was tested using the Maxim HIV-1 Limiting Antigen Avidity (LAg) EIA (Maxim Biomedical, Inc. Rockville, Maryland, USA). The mean age of study subjects was 29.5 years: PWID, 28.5 years and TG-HSWs, 30.4 years. Study subjects were married, 27%, or unmarried. Eighteen percent of individuals had recently-acquired HIV infections: 19% of PWID and 17% of TG-HSWs. Eighty-two percent of individuals had long-term HIV infections: 81% of PWID and 83% of TG-HSWs. This is the first study identification of recent HIV-1 infections in Pakistan. We show that most newly-diagnosed HIV patients in the high-risk groups studied had long-term infections. There is an urgent need for intervention in these groups to facilitate early diagnosis and treatment of HIV infection to reduce transmission in Pakistan.
Introduction
The human immunodeficiency virus (HIV) affects 36.7 million individuals worldwide and led to mortality of 1.1 million individuals in 2016.1,2 An estimated 25.6 million affected people live in sub-Saharan Africa making it the region with highest number of people living with HIV (PLHIV). 1 The Eastern Mediterranean region is reported to have 360,000 PLHIV, 2 and within this, Pakistan is estimated to have 130,000 PLHIV. 3 Although the HIV prevalence in the general population in Pakistan remains low, with an estimated rate of <0.1% among adults aged 15 to 49 years, the number and rate of infections have shown a significant increase among high-risk populations. 1
The first case of indigenous HIV transmission in Pakistan was reported in 1988. 4 In the 1990s, most HIV-positive cases were reported among Pakistani workers deported from the Gulf States and among foreigners living in Pakistan. 5 Subsequently, a shift in the HIV epidemic in Pakistan started with an outbreak observed amongst people who inject drugs (PWID) in the small town of Larkana in 2004 6 and the larger cities of Karachi and Lahore. 7 HIV seroprevalence in PWID increased from 9.3% in 2004 6 ; 20% in 2009, 8 and currently at 38.4%. 9 Additionally, HIV infection rates in other high-risk groups were estimated at 11% in men who have sex with men (MSM) and 6% in Afghan refugees in 2010.10,11
The estimated number of PWID in Pakistan has been reported as 80,000–145,000. 12 It is thought that two-thirds of PWID are in the metropolitan city of Karachi. 9 In Karachi, the HIV prevalence among PWID has increased from 0.3% in 2003 to 23% in 2007, with 42% prevalence reported in 2011.7,13 Recent reports indicate the prevalence of HIV in PWID to be 38.4%. 9 A study on HIV seropositivity in PWID in Pakistan suggested an increasing rate of 12.4% per 100 person-years. 8 This indicates HIV incidence to be on the rise, regardless of risk reduction programs, with PWID as a driver of transmission in the country.
Factors associated with increasing HIV rates in high-risk populations, such as prisoners and PWID, include low condom usage by commercial sex workers and their clients,14,15 and incomplete needle/syringe exchange programs for PWID. 8 Current trends indicate that HIV infection rates may also be increasing in the so-called low-risk groups: HIV transmission by MSM and PWID to female spouses and children (through sexual and vertical transmission, respectively). 16 Another concern is antiretroviral (ARV) resistance reported at 14.2% in the province of Sindh, with 6.5% among treatment-naïve patients and 36.4% among ARV-experienced patients. 17
Another high-risk group for HIV is transgenders also known as hijra sex workers (TG-HSWs), who are biological males who identify themselves as females. Hijras have been a prominent part of South-Asian culture typically involved in the profession of singing and dancing at weddings and other ceremonies. These individuals maintain a lower social status and are marginalized for their gender identity and are frequently involved in sex trade. According to the national HIV surveillance program, there are approximately 36,000 TGs in cities and 200,000 nationwide and one-quarter of this population are involved in the HSW trade. 15 Karachi is estimated to have the largest (60%) proportion of this group with about 9000 TG-HSWs. 9 Recent surveillance reports cite prevalence of HIV in TG-HSWs to be 7.5% and the same in Karachi to be 12.9%. 9
Currently, the available HIV data for Pakistan have been based on targeted prevalence serosurveys, and incidence data are lacking. To determine the HIV incidence in a population, it is important to identify new or recent infections. A number of assays based on the identification of IgG antibodies to HIV-specific antigens have been developed.18,19 These are suggested for use in determining incidence in surveillance studies. 20 Incidence data are important in public health decision making and planning and for monitoring trends in the epidemic in particular populations. Here we investigated the frequency of recent HIV infections in two HIV antibody-positive high-risk populations, PWID and TG-HSWs. We used the HIV-1 LAg assay, 21 an in-vitro quantitative limiting antigen avidity enzyme immunoassay, to distinguish between recent and chronic or long-term HIV-1 infections. The assay involves the use of a recombinant rIDR-M protein which covers the immunodominant gp41 region (IDR) of all major subgroups and subtypes as well as major recombinants of HIV-1 group M. 22 Studies have identified that a six-month recency period or mean duration recent infection is what can be identified by low avidity-index testing based on the recommended cut-off of ODn 1.5.18,19 In contrast, a higher value suggests a long-term or chronic infection. Our data highlight that most HIV cases were diagnosed as long-term infections, indicating that there is delayed treatment and an increased risk of transmission from these patients prior to the awareness of their HIV status.
Materials and methods
Study design and population
This was a cross-sectional study conducted in Karachi which is the most populated metropolitan city in Pakistan, with an estimated 14.9 million individuals. 23 The study populations were PWID and TG-HSWs. The case definition for PWID was any person above 18 years old who injected drugs regularly for other than therapeutic reasons for at least six months; TG-HSWs were transvestites or transsexuals above 18 years who engaged in sexual activity with men in return for money or other benefits. A convenience sampling technique was employed with all newly-diagnosed HIV-positive PWID or TG-HSWs eligible to participate. This study received approval from the Ethical Review Committee of The Aga Khan University, Karachi, Pakistan, and the Institutional Review Board, Bridge Consultants Foundation (BCF), Pakistan.
Data collection
For incidence assay testing, a pre-determined sample size of 212 was taken to equally represent both target populations. One hundred and six PWID and 106 TG-HSWs were recruited with informed consent. Two samples from the PWID group could not be tested due to a technical issue. Therefore, the remaining 210 specimens from 104 PWID and 106 TG-HSWs were tested. All enrolled participants were already registered with community home-based care sites of BCF in Karachi, Pakistan, and were receiving HIV treatment and health-care services from them. Individuals were eligible for enrolment into the study for LAg testing and completion of the questionnaire only if they were tested and determined to be HIV antibody-positive within the previous 24 weeks. Subjects who had been diagnosed with HIV for >24 weeks at the time of recruitment were excluded from the study.
The data collection questionnaire used had been previously developed, field tested, and used in different rounds of Integrated Behavior and Biological Surveillance by the HIV/AIDS surveillance project supported by National AIDS Control Program Pakistan. 3 The form included questions regarding gender, ethnicity, marital status, education, occupation, date of HIV diagnosis, monthly income, partner’s HIV status if known, and probable mode of HIV transmission. Years of formal education, defined as teaching in an organized school setting, was documented. HIV diagnostic testing was performed as was HIV viral load and CD4 cell counts.
The field research team was comprised of a team leader, two social mobilizers, three supervisors, nine interviewers, one phlebotomist, and two messengers. Social mobilizers helped in community mobilization for data collection, providing services to PWID and TG-HSWs and assisted the research team in data collection.
HIV testing
Initially, finger prick blood samples were tested using the Alere Determine Combo (HIV Ag/Ab) rapid test. Study participants were provided results of the HIV test with post-test counseling. Those with a reactive rapid HIV antibody test had a further blood draw and were subsequently tested by two enzyme-linked immunosorbent assay (ELISA) tests based on different antigens such as HIV-1/2 ELISA 4.0 (MP Biomedicals, Sana Ana, California, USA) and HIV Ag-Ab Combo Assay (Bio-Rad, Hercules, California, USA). Individuals confirmed to be HIV-positive were then recruited for the incidence assay after obtaining informed consent. Whole blood samples were taken and the serum separated was stored at −80°C until tested.
Incidence assay
Serum samples were tested for the presence of HIV-1 antibodies using the Maxim HIV-1 Limiting Antigen Avidity (LAg) EIA test (Maxim Biomedical, Inc., Rockville, Maryland, USA) as per the manufacturer’s instructions. The test determines the presence of high-avidity antibodies using a quantitative assay. Briefly, test samples are incubated in plates coated with recombinant gp41 antigen (rIRD-IM); including a negative control, a calibrator, and low-positive and high-positive controls. The binding reaction between test sera and rIRD-IM was determined after the development of ELISA with a horse radish peroxidase-bound conjugate. Spectrophotometric reading at 450 nm/655 nm was used to obtain normalized OD results (ODn). Samples with ODn 2.0 were considered chronic or long-term anti-HIV antibodies. Samples with ODn ≤ 2.0 were re-confirmed by re-testing in triplicate, and subsequently, samples with a mean ODn > 1.5 was used as a cut-off to distinguish long-term infection from recent infection.
Results
Description of the study subjects
We analyzed data for 210 HIV-positive study subjects tested using the LAg avidity assay. There were 104 PWID and 106 TG-HSWs. The overall mean age of the group was 29.5 years: PWID, 28.5 years and TGs, 30.4 years. Overall, 56 (26.7%) of the study subjects were married while the remaining 154 (73%) were single (unmarried, divorced, separated, or widowed), as summarized in Table 1. Marriage between TGs, hijras, is not legal in Pakistan; therefore, marriages identified are those of biological males married to females. Within the sub-groups, 33 (31.7%) of PWID and 23 (21.7%) of TG-HSWs were married. Seventy-one PWID and 83 TG-HSWs were single. Regarding formal education, 96 (45.7%) of the study subjects had not received any schooling: 49 (47.1%) PWID and 47 (44.3%) TG-HSWs. Fifty-eight (27.6%) of the overall group had received less than five years of education, varying between 20.2% in PWID and 34.9% in TG-HSWs. Fifty individuals (23.8%; 30.8% of PWID and 17% of TG-HSWs) had received 5–10 years of education. Six study subjects (2.9%; 1.9% of PWID and 3.7% of TG-HSWs) had received greater than 10 years of education.
Demographic characteristics of study subjects.
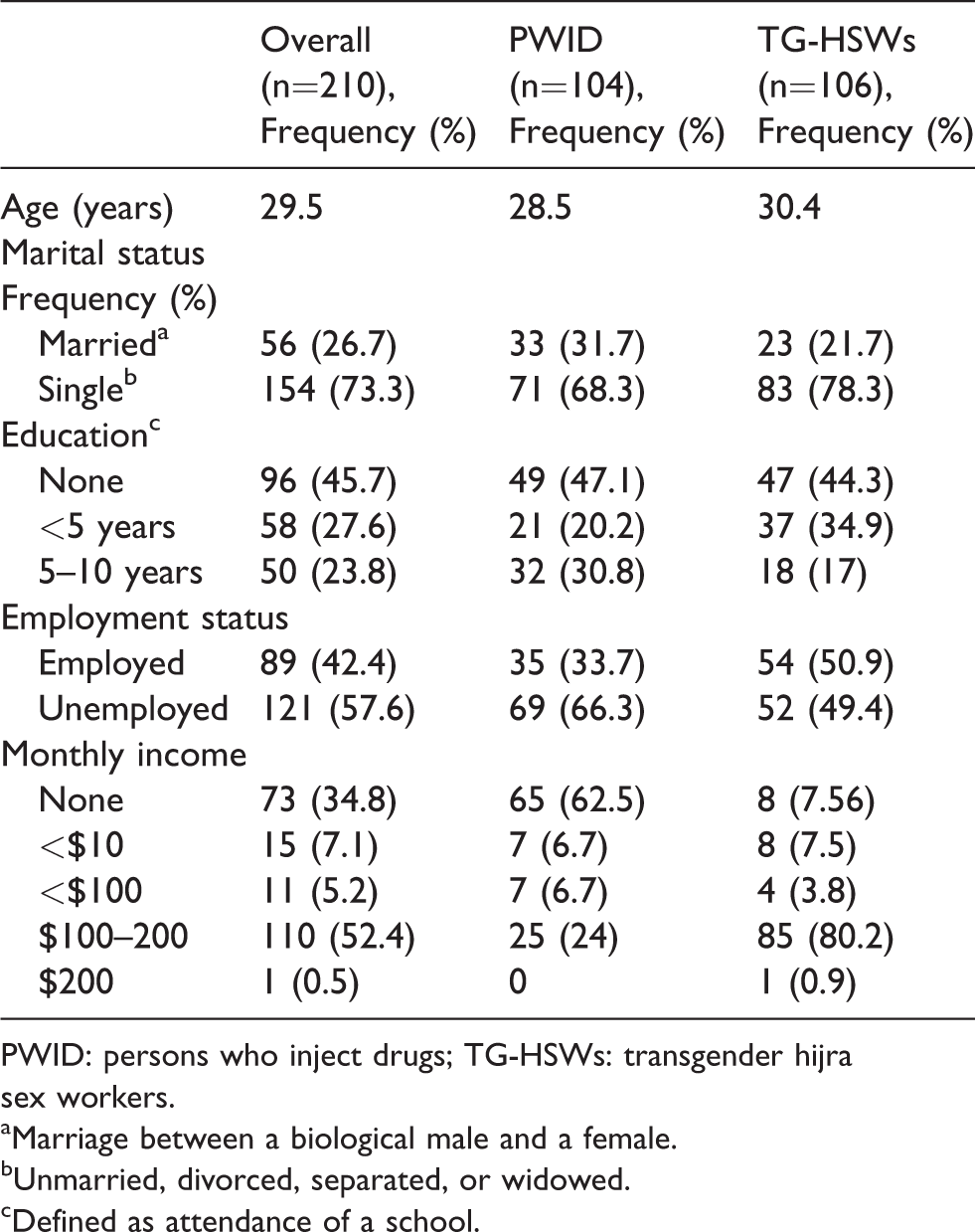
PWID: persons who inject drugs; TG-HSWs: transgender hijra sex workers.
aMarriage between a biological male and a female.
bUnmarried, divorced, separated, or widowed.
cDefined as attendance of a school.
Eighty-nine (42.4%) of the overall group were in formal employment: 34% of PWID and 51% of TG-HSWs. Amongst the employed PWID (n = 35), 15 were unskilled and 18 were skilled workers but two did not reveal their profession. Amongst the employed TG-HSWs (n = 53), 4 were unskilled, 3 were skilled workers, and 45 individuals did not reveal their profession although they were known to be in sex-work jobs. One hundred and twenty-one (57.6%) study subjects were unemployed. Sixty-nine (66%) PWID were unemployed. Fifty-four (50.9%) TG-HSWs who were unemployed (not in formal employment) identified themselves as beggars or dancers. Overall, 73 (34.8%) of study subjects did not have any monthly income (62.5% of PWID and 7.6% of TG-HSWs). Conversely, 137 (65.3%) of study subjects had a monthly income (37.5% of PWID and 92.5% of TG-HSWs). Income level assessment in PWID revealed 25 (24%) earning $100–200/month and 7 (6.7%) earning < $100/month and < $10/month each, respectively. Amongst TG-HSWs, 89 individuals (81.1%) earned > $100–200/month, 4 (3.8%) earned < $100/month, and 8 (7.5%) earned <$10/month.
Proportion of HIV infections classified as recent or long-standing
We determined the recency of HIV infection in the newly-diagnosed study cohort using LAg avidity assay testing. Based on the final result, individuals were divided into those with recent or newly-acquired HIV infections or chronic, long-term infections. Further, to avoid any confounding effect related to the time of recruitment of the subject into the study (which was up to 24 weeks after initial diagnosis), data for recent and long-term infection were stratified according to the time between the date of initial HIV diagnosis for each individual and recruitment in the study. Sixty-nine percent of all participants were tested within 4 weeks of their HIV diagnosis and 82% within 8 weeks of diagnosis (Table 2).
Time between HIV diagnosis and LAg testing.

aTime between initial diagnosis of HIV and sampling for the study.
bNumber of HIV-positive study subject recruited in the period.
LAg avidity assay testing revealed that 72 (82%) of study subjects had long-standing infections and 18% had recently-acquired HIV infections (Table 3). Eighty-one percent of PWID and 83% of TG-HSWs had long-standing HIV infections. Nineteen percent of PWID and 17% of TG-HSWs had evidence of recent HIV infections. To see if there was any association between identification of long-standing infection and the time from initial diagnosis to recruitment, we analyzed the LAg results as per the time of sampling in this study. Of those with long-standing infections, 65% had LAg testing within 4 weeks and 77% within 8 weeks of HIV diagnosis (Figure 1(a)). Of those with recently-acquired infections, 82% had LAg testing within 4 weeks and 85% within 8 weeks of HIV diagnosis (Figure 1(b)).
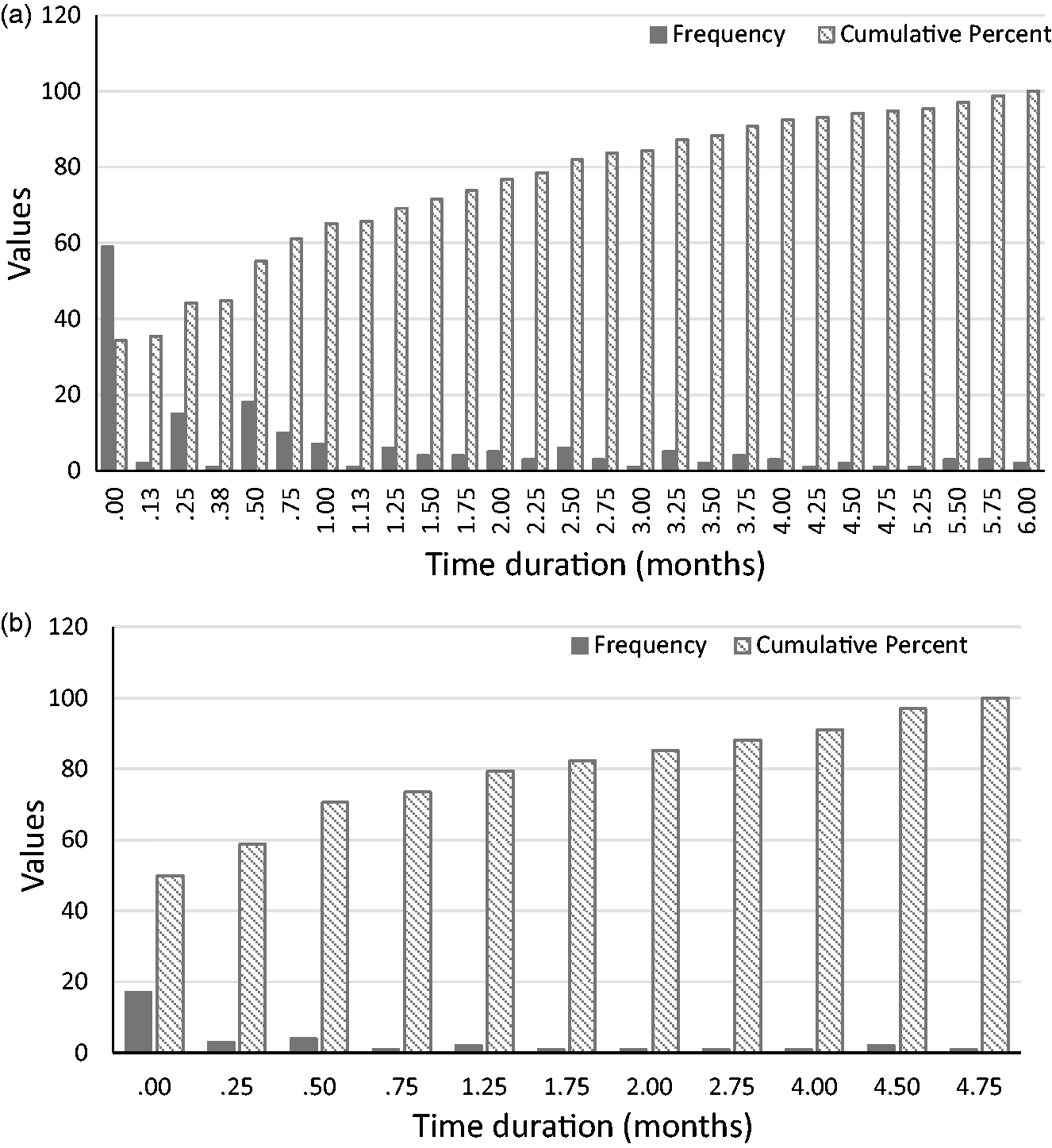
Frequency of positive LAg tests in relation to time of HIV diagnosis in study subjects. The graphs depict month-wise identification of (a) long-standing HIV infections and (b) recently-acquired HIV infections amongst the high-risk groups tested. People who inject drugs (PWID, n = 104) and transgender hijra sex workers (TG-HSWs, n = 106) populations.
Incidence of HIV infection.
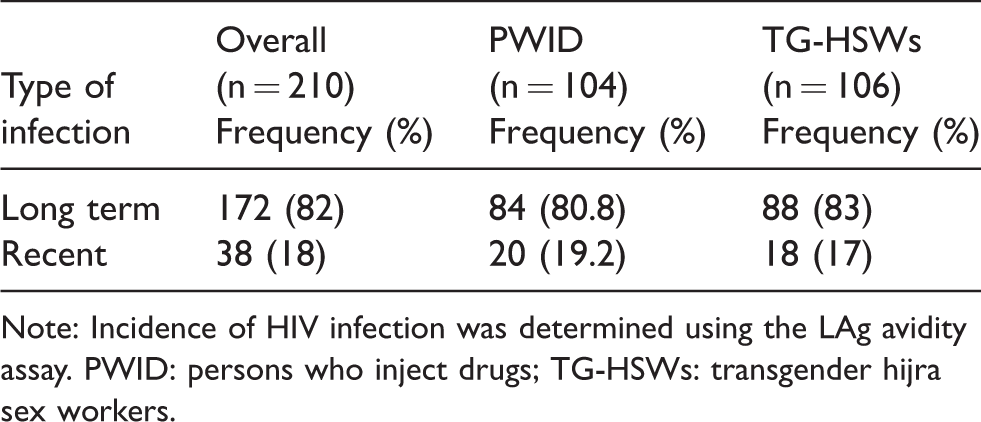
Note: Incidence of HIV infection was determined using the LAg avidity assay. PWID: persons who inject drugs; TG-HSWs: transgender hijra sex workers.
Discussion
This is the first study to investigate recency of HIV infections in newly-diagnosed patients in Pakistan. It focused on two high-risk populations in Pakistan, PWID and TG-HSWs. Overall, 18% of individuals had recently-acquired HIV infections and 82% had late HIV infections. Nineteen percent of PWID had recent and 81% had late infections, and 17% of TG-HSWs had recent while 83% had late, chronic HIV infections. The demographics of the high-risk groups showed a mean age of 29 years including both married and unmarried individuals in the cohorts studied. The majority of individuals had not received any formal schooling. Unemployment was high in both groups. Income generation was low, particularly in the PWID groups.
Recent analysis on HIV prevalence in Pakistan and epidemic modeling of the disease have already identified these groups as key high-risk groups and drivers of the HIV epidemic in the country. It has been reported that needle exchange programs are not working sufficiently, further increasing risk in the PWID. Our data indicate that within the high-risk groups, there is an additional burden due to late diagnosis which is in turn linked to continual transmission of HIV infections. The spread of HIV through both male and female partners was evident in that both PWID and TG-HSWs included individuals who were married to women, further driving horizontal and vertical transmission in the population through sex with female partners. The young age we observed is in concordance with national survey results that show the age of high-risk groups to be 16–49 years. 3 The lack of education revealed low literacy levels in the country and particularly in these high-risk cohorts. 3 We observed that the average income of PWID was lower (< $100/month) as compared with TG-HSWs ($100–200/month) which is also concordant with national data. 3 The higher income of the TG-HSWs despite formal employment is reflective of their lifestyle and sexual behavior.
A recent survey from Pakistan in 2016 indicated HIV seroprevalence to be 38.4% among PWID and 7.1% among TG-HSWs. 9
The identification of mostly long-term HIV infections in the PWID and TG-HSWs is also possibly reflective of their lack of awareness related to health care and/or limited access to health-care facilities. The high-risk behavior and practices of the PWID and TG-HSW groups put them at risk of additional infections and of spreading HIV. It has been reported that 58% of TG-HSWs and 38% of PWID in Pakistan had multiple sexually transmitted infections. 11 Recently, it has been shown that the HIV epidemic in Pakistan is heterogeneous and there is intermixing between populations of PWID and TG-HSWs, further driving transmission. 24 There is a growing awareness of increasing rates of HIV transmission in Pakistan and the epidemic which was previously termed “low prevalence, high risk” is now a “concentrated” epidemic.
The definition of recency of HIV-1 infection is the period between seroconversion and the establishment of viral load in the infected individuals. Recent infections are difficult to diagnose and different assays have varying sensitivities for Mean Duration of Recent Infection (MRDI). 18 As we used the low avidity LAg assay which has an MRDI of six months, 19 we included patients who had been diagnosed with HIV in the 24 weeks prior to inclusion in the study. To see if there could be any bias in the assessment of “late” infections due to the sampling period, we also divided this into four-week intervals. Sixty-five percent of participants had LAg testing within four weeks of HIV diagnosis.
The marital status of study subjects from high HIV-risk groups studied indicated that about one-third were in heterosexual marriages. As such, they are at risk of transmitting the infection to their partner/s. Since incidence testing revealed that 80% of individuals were diagnosed with long-term HIV infections, there is risk that they may have already transmitted HIV to their spouses or to others prior to the diagnosis of their HIV infections.
An analysis of the education and economic conditions of the HIV-positive study population identified that most study subjects had received limited or no education. In addition, a large majority of them had a very low income level, earning <$100 a month in the case of PWID. The HSWs had higher incomes of $100–200/month, but as this was probably a consequence of their sexual behavior, it only increased their own risk.
Poor access to health care, economic distress, and marginalized populations are all conditions that have been related to poor health-seeking behaviors. In HIV-infected populations, access to health care, stigma against HIV, and financial concerns have been identified as pre-disposing conditions to HIV worldwide.25,26 There are additional concerns due to the emergence of ARV resistance mutations among various HIV strain types which are driving the HIV epidemic in Pakistan. 27
The study had some limitations related to the relative sample size and restricted sampling strategy due to financial constraints. Therefore, the actual sample size was not calculated. Also, we could only target two high HIV-risk populations from a selected population in Karachi. Therefore, we can infer that the trends observed regarding diagnosis are consistent with those observed nationwide. One inherent limitation is of the Avidity EIA itself which may give a false result of recent infection if there are low antibody concentration present in the specimen. 28
We highlight the high rates of long-term HIV infection in newly-diagnosed cases from high-risk groups: PWID and TG-HSWs. Late diagnosis of HIV infection results in an increased period of transmission and spread through patients and their contacts. Although action is being taken on the part of government and at non-governmental levels to diagnose and treat HIV, there remains a gap in what is required. At a policy level, it is imperative to have improved interventions to increase health access to these groups which have a low-level of health-seeking behavior as a consequence of their social and economic factors. There should be easy-to-access care for these marginalized populations that provide counselling, diagnosis, and treatment for HIV. Without an improvement in the HIV treatment and monitoring system, we will continue to see increasing infections in high-risk populations and with progressive infection rates in the low-risk groups as well.
Footnotes
Acknowledgements
Study subjects were recruited through the Bridge Consultants Foundation, Pakistan network. We thank Rubab for her field work and recruitment of study subjects.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through funds from Blood Systems Research Institute from EQAPOL “NIAID DAIDS External Quality Assurance Program (EQAPOL, HHSN272201700061C).”