
Abstract
Data on the association between syphilis reactivity and dementia in memory clinic patients are scarce. We studied the prevalence of syphilis reactivity and investigated its association with dementia and markers of cerebrovascular disease (CeVD) and neurodegeneration. Data on age, gender, education, brain computed tomography scan findings and syphilis reactivity were obtained from patients who attended the National University Hospital memory clinics (February 2006–February 2016) and subjects from the community. Binary logistic regression models were used to investigate associations between syphilis reactivity and dementia, CeVD and neurodegeneration, and odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Of 1271 memory clinic patients eligible for the study, 57 (4.5%) were syphilis reactive, with the rate of syphilis reactivity higher in demented (44/745; 5.9%) compared to non-demented (13/526; 2.5%) patients (p = 0.004) and non-demented community-based (21/872; 2.4%) subjects (p < 0.001). Binary logistic regression showed a significant association between syphilis reactivity and dementia in memory clinic patients independent of demographic factors (odds ratio: 2.06; 95% CI: 1.02–4.17, p = 0.044). A significant association between syphilis reactivity and dementia was found in memory clinic patients. The mechanism of this association requires further research and may involve neuroinflammation.
Introduction
Syphilis is a sexually transmitted multisystem disease that can affect the central nervous system, causing neurologic and psychiatric manifestations in distinct stages, 1 as the causative spirochete bacterium (Treponema pallidum) remains in the central nervous system after the primary infection. 2 Although neurological problems are usually present in the late stage of syphilis infection, T. pallidum can also invade the nervous system in the early stages of the disease, 3 giving rise to a wide range of symptoms ranging from headache, to altered behaviours, and cognitive impairment and dementia. 4
It has been reported that 36.4 million people were infected with syphilis worldwide in 2008 and approximately 12 million new cases are reported every year worldwide. 5 A study conducted in a demented Caucasian population reported a 10.9% prevalence of syphilis reactivity. 6 However, this study was published over two decades ago in 1993 and did not have a control group. There are no recent studies on syphilis reactivity in dementia populations. Prevalence estimates of syphilis infection in older Asian populations range between 0.22 and 12.7%,7,8 whereas in Singapore it is reported to be 0.026%. 9 This wide range may be due to differences in socio-economic status, unsafe sexual practices, change in sexual preferences, incidence of immunocompromised diseases such as HIV, migration and travel. 10 The prevalence of syphilis reactivity in Asian dementia populations is yet to be reported.
A previous study on assessing syphilis reactivity using blood tests has reported its association with impaired cognition in immunocompromised patients. 11 Whilst vascular dementia has been described in the tertiary stage of syphilis, due to numerous cerebral infarcts, 12 only a few case studies have reported the presence of white matter hyperintensities (WMHs), cerebral infarction and cerebral atrophy in cognitively-impaired syphilis-reactive subjects.13–16
Therefore, the present study had two aims. The first was to investigate the prevalence of syphilis reactivity in elderly patients with dementia in an Asian memory clinic population in comparison to non-demented patients of the same memory clinic population as well as non-demented community-based subjects from the Epidemiology of Dementia in Singapore (EDIS) study. Second, was to examine the association between syphilis reactivity with dementia, cerebrovascular disease (CeVD) and neurodegeneration in memory clinic patients. Specific hypotheses were as follows: (a) there is higher prevalence of syphilis reactivity in demented patients compared to non-demented patients in memory clinic, as well as to community-based non-demented subjects; (b) there is no difference in prevalence of syphilis reactivity between non-demented memory clinic patients and non-demented community-based subjects and (c) syphilis reactivity is associated with markers of CeVD and neurodegeneration as assessed by computed tomography (CT).
Methods
Study design
We retrospectively analysed patients attending memory clinics at the National University Hospital (NUH), Singapore from February 2006 to February 2016 and community-based subjects from the EDIS study. The EDIS study recruited multi-ethnic (Chinese, Indian and Malay) subjects from the Singapore Epidemiology of Eye Disease (SEED) study. 17 Participants from the SEED study who were ≥60 years old and were screened positive on the Abbreviated Mental Test or self-reported progressive forgetfulness, and were invited to participate in the EDIS study and underwent clinical and neuropsychological assessment from August 2010 to July 2015.
Data were obtained from review of medical records including, age, gender, education (≥6 years and <6 years of formal education), syphilis reactivity and Mini-Mental State Examination (MMSE). However, only CT scans performed after July 2011 were analysed as they had coronal sequences required for assessment of atrophy.
This study was approved by the National Healthcare Group Domain-Specific Review Board (DSRB) of Singapore (DSRB Reference: 2017/00745) for the use of previously collected data from the NUH dementia registry (NUH/2014-00039). For the EDIS study ethics approval was obtained from both the Singapore Eye Research Institute and National Healthcare Group DSRB.
Syphilis reactivity
We used the enzyme immunoassay (EIA) test to detect syphilis reactivity. The test was performed in the diagnostic laboratory of NUH, using an automated chemiluminescence immunoassay. In this study, subjects reactive on EIA were considered as subjects with syphilis reactivity. All subjects with syphilis reactivity were referred for lumbar puncture for cerebrospinal fluid-venereal disease research laboratory (CSF-VDRL) test.
Neuroimaging
Non-contrast CT scans were performed using a 256-multislice CT from Philips (slice collimation: 30 by 0.625 mm2 for CT brain, kVp: 120, mAs: mA modulation with reference mAs of 300).
Markers of CeVD on CT scan were graded using the following criteria:
Lacunae were defined by the presence of hypodense focal lesions measuring ≥3 mm and <15 mm. Cortical infarcts were defined as hypodense lesions interrupting the cortex grey/white junction. WMHs were graded using the age-related white matter changes (ARWMC) scale.
18
Markers of neurodegeneration on CT scan were graded using the following criteria:
The degree of central and cortical atrophy was graded by ventricular or subarachnoid space and sulcal dilation, on axial sections. The degree of cortical and central atrophy was rated and categorized using a 4-point scale (0 – normal, 1 – mild, 2 – moderate or 3 – severe).
19
Medial temporal lobe atrophy (MTA) was graded on coronal sections and was defined using the 5-point Scheltens’ scale (0 – normal, 1 – mild, 2 – mild–moderate, 3 – moderate, 4 – severe) which takes into account the widening of the choroid fissure, widening of temporal horn and loss of hippocampal height.
20
The degree of central and cortical atrophy was further divided into two groups: no significant atrophy (0–1) and significant atrophy (2–3). Similarly, MTA was also categorized into two groups: no significant MTA (0–1) and significant MTA (2–4). WMHs were also categorized into two groups: no significant WMHs (ARWMC< 8) and significant WMHs (ARWMC ≥8).
Cognitive assessment
Diagnoses were made in weekly consensus meetings attended by neurologists, psychologists and research staff. Diagnostic evaluations involved past and present medical history, physical examination, blood test, CT scan findings and neuropsychological assessment. Other possible causes of cognitive impairment and dementia such as HIV infection, subdural haemorrhage, obstructive hydrocephalus, infection, intoxication, medication, electrolyte disorders, hypothyroid and nutritional deficiency states like low vitamin B12 were excluded.
Those who were not impaired in any of the domains of the neuropsychological test battery were diagnosed as no cognitive impairment (NCI). Diagnosis of cognitive impairment no dementia (CIND) was made if there was impairment in at least one domain of a neuropsychological test battery without any significant loss of independence in daily activities. Diagnosis of dementia fulfilled the criteria of Diagnostic and Statistical Manual of Mental Disorders-IV. For the purpose of this study, patients were broadly classified into two groups: patients with diagnosis of NCI or CIND were classified into the ‘non-demented’ group, and patients with a diagnosis of dementia were classified into the ‘demented’ group.
Statistical analysis
In order to examine differences between memory clinic patients and non-demented EDIS subjects and non-demented memory clinic patients, Mann–Whitney U test was performed for continuous variable and Chi square test for dichotomous variables. A binary logistic regression model was constructed to compute odds ratios (ORs) and 95% confidence intervals (CIs) for the association between syphilis reactivity with dementia, neurodegeneration and CeVD. The regression model was adjusted for age, gender and education. The tests were considered significant at p < 0.05. All the data were analysed using SPSS software package (version 24).
Results
Among 1682 patients from the memory clinic, only 1271 (526 non-demented and 745 demented) patients with complete investigations and consensus diagnosis were available for the analyses (Figure 1). Excluded patients were significantly younger, had a higher level of education and had a higher MMSE score (p < 0.05) (Supplementary table 1). Of 1271 subjects with a syphilis reactivity performed and with consensus diagnosis only a subgroup of 580 patients with CT scans in standard digital format with coronal sequences were analysed to test the association between CeVD and neurodegeneration (Figure 1). Patients without CT scan were significantly younger and had higher levels of education (p < 0.05) compared to patients with CT scan (Supplementary table 2).
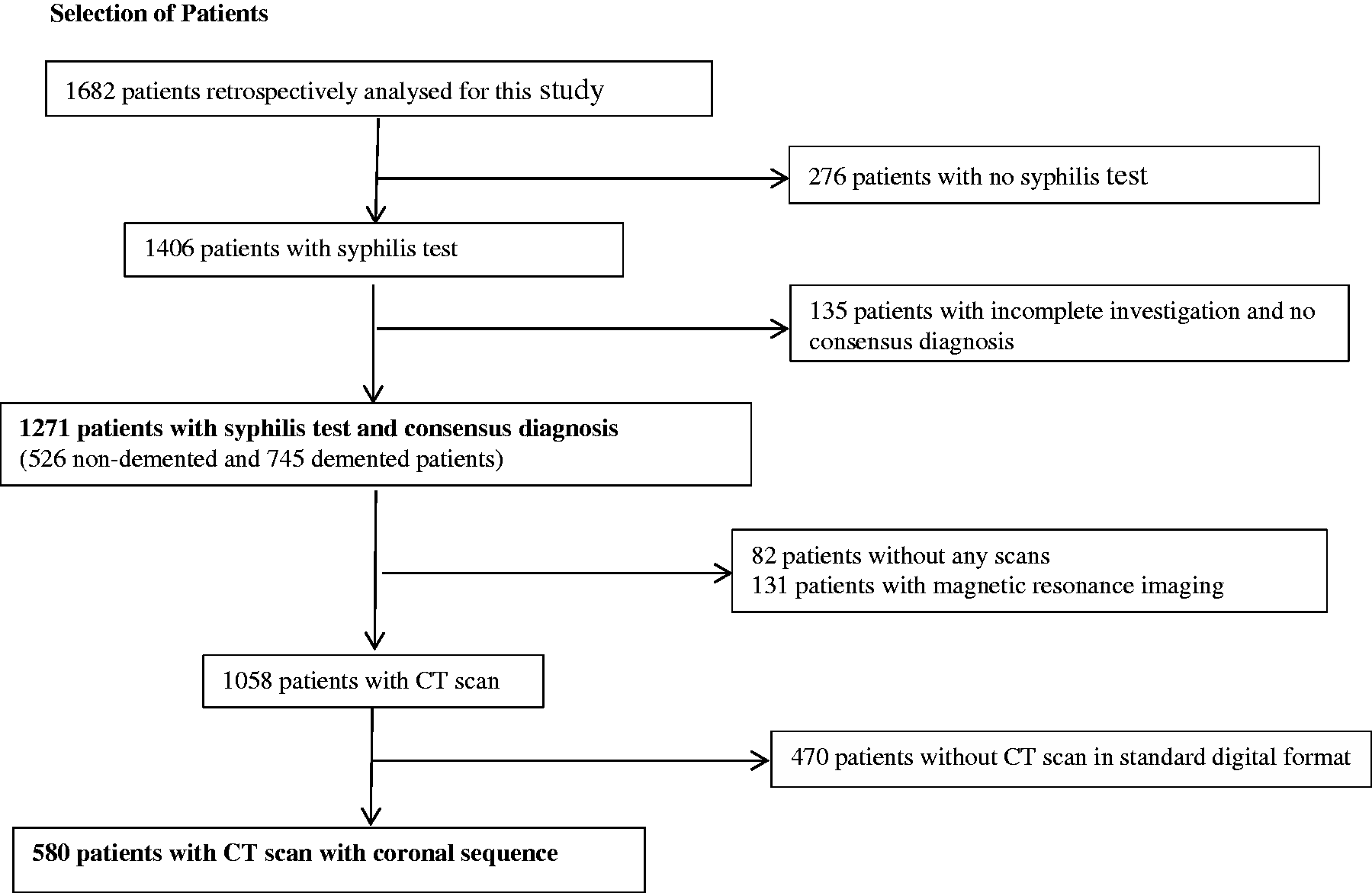
Selection of patients. CT: computed tomography.
Of the 1598 screened-positive participants from the SEED study who were invited to participate in the EDIS study, 957 agreed. Of 912 non-demented subjects eligible for this study, 40 did not have a syphilis reactivity test performed, leaving 872 non-demented community-dwelling subjects for the analysis.
The characteristics of the study population from memory clinic patients and non-demented subjects from the EDIS study are shown in Table 1. In the memory clinic sample, demented patients were significantly older and had a lower level of formal education compared to non-demented patients (p < 0.05). Non-demented subjects from the EDIS study were younger, had higher level of education and had higher MMSE score compared to demented subjects from the memory clinic (p < 0.05). The overall prevalence of syphilis reactivity in the memory clinic was 4.5%. Significantly more (44; 5.9%) of the dementia patients were syphilis reactive compared to non-dementia patients (13; 2.5%; p = 0.004) from the memory clinic and non-demented subjects from the community (21; 2.4%; p < 0.001). There was no significant difference in the prevalence of syphilis reactivity between non-demented memory clinic and non-demented community-dwelling subjects (p > 0.05).
Characteristics of patients from the memory clinic (n = 1271) and non-demented participants from the EDIS study (n = 872).
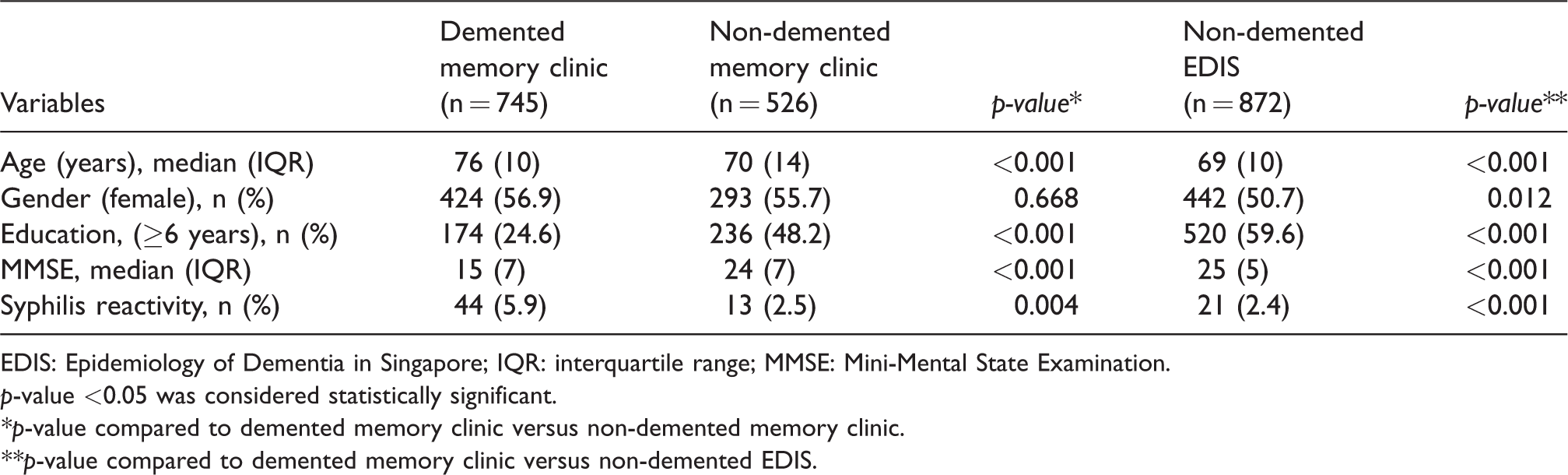
EDIS: Epidemiology of Dementia in Singapore; IQR: interquartile range; MMSE: Mini-Mental State Examination.
p-value <0.05 was considered statistically significant.
*p-value compared to demented memory clinic versus non-demented memory clinic.
**p-value compared to demented memory clinic versus non-demented EDIS.
Table 2 shows the subgroup analysis of memory clinic patients with CT scan findings. There were no differences between the two groups with respect to markers of CeVD and neurodegeneration (p > 0.05).
Characteristics of subgroup memory clinic patients with CT scan findings (n = 580).
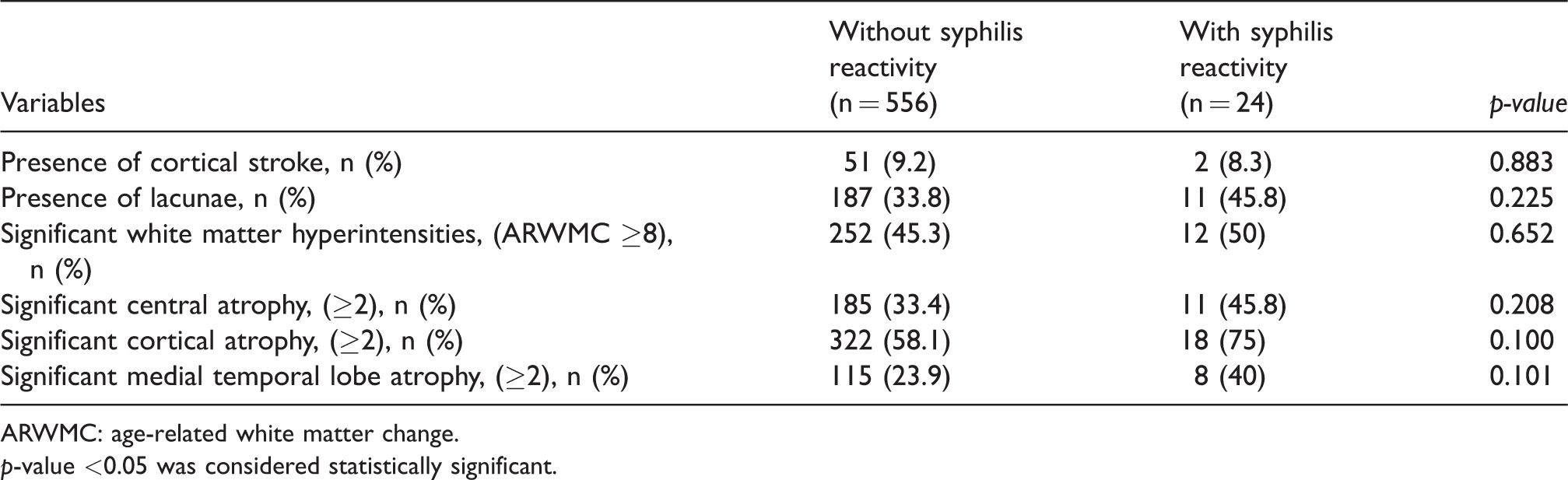
ARWMC: age-related white matter change.
p-value <0.05 was considered statistically significant.
Table 3 summarizes adjusted models using binary logistic regression for the association between syphilis reactivity with dementia, markers of CeVD and neurodegeneration in memory clinic patients. After adjusting for age, gender and education, syphilis reactivity was significantly associated with dementia (OR: 2.06; 95% CI: 1.02–4.17; p = 0.044). There was no significant association between syphilis reactivity and any markers of CeVD and neurodegeneration.
Association between syphilis reactivity with dementia, markers of cerebrovascular disease and neurodegeneration in the memory clinic.
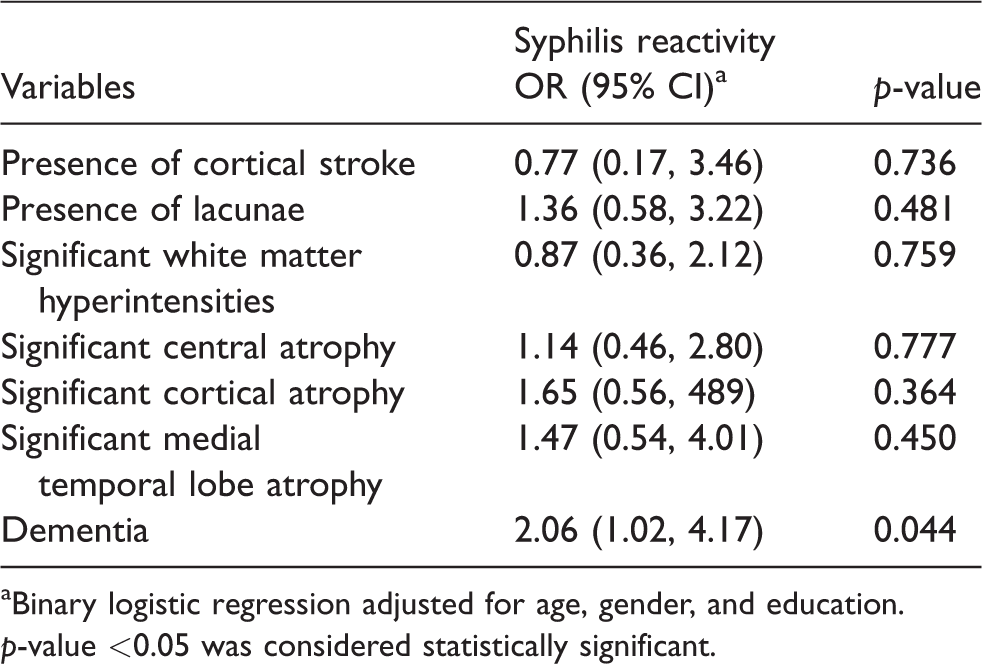
aBinary logistic regression adjusted for age, gender, and education.
p-value <0.05 was considered statistically significant.
Discussion
Our study demonstrates that in an Asian memory clinic population, the overall prevalence of syphilis reactivity was 4.5%. There was significantly higher prevalence of syphilis reactivity in demented compared to non-demented patients from both the memory clinic and community, and there was similar prevalence rate of syphilis reactivity between non-demented memory clinic and non-demented community subjects. There were no significant associations between the presence of CeVD and neurodegeneration with syphilis reactivity.
We found a 5.9% prevalence of syphilis reactivity in memory clinic patients with dementia. Although several reports have stated an increased rate of syphilis reactivity among hospitalized elderly Asian patients,21,22 there are limited reports exploring the prevalence of syphilis reactivity in dementia populations from Asian memory clinics. According to the data from the Ministry of Health, Singapore, the incidence rates of syphilis in the general population have shown a dramatic increase from 1.7 per 100,000 populations in 1999 to 6.9 per 100,000 populations in 2005. 23 In 2016, the Department of Sexually Transmitted Infections Control, Singapore reported 1481 cases affected by syphilis infection in Singapore, which is approximately 0.026% of the Singapore population. 9 Although there has been a significant drop in infection rate after 2005, syphilis infection is still one of the most common sexually transmitted infections in Singapore.9,23 Syphilis is one of the treatable causes of cognitive impairment and dementia. 24 Syphilis can be easily treated with antibiotics but the under-detection and treatment failure of syphilis may lead to multi-system damage and possibly increase the risk of concomitant neurological impairments. 25 Therefore, the presence of syphilis reactivity in patients with dementia may suggest a need for earlier detection and treatment.
Our study demonstrates syphilis reactivity to be independently associated with dementia but not associated with CeVD or neurodegeneration. The association with dementia may be instead due to spirochete-induced chronic neuroinflammation. Several bacterial infections, including spirochetes containing amyloidogenic proteins, can induce deposition of amyloid beta and tau phosphorylation.26,27 Moreover, spirochetes have the ability to evade host defence mechanism and activate inflammatory processes and host immune responses, which cause damage to infected and neighbouring neuronal cells. 28 The effect of Treponema and other microorganisms in dementia has been mostly focused on Alzheimer’s disease (AD).26,29,30 Previous studies in AD patients have shown the role of systemic inflammation in the disease process. Infection from various organisms such as syphilis can accelerate neurodegeneration through various neuropathological processes such as increased oxidative stress, formation of inflammatory mediators and increased production of beta-amyloid proteins.27,28 Neuropathological studies have shown infiltration of spirochetes into brain tissue may cause degeneration, fibrosis and gradual narrowing of cerebral blood vessels. 12 Such degeneration may increase permeability of the blood–brain barrier leading to vasogenic and cytotoxic oedema, which, if not treated may at a later stage undergo irreversible atrophy. Similarly, fibrosis and gradual narrowing of blood vessels cause hypoperfusion in brain tissue; such chronic hypoperfusion leads to cerebral atrophy, lacunae, infarcts and WMHs.14,15,31,32 Although prior studies reported that syphilis infections may contribute to vascular dementia through several pathological changes to blood vessels affecting cerebral blood flow that lead to multiple cerebral infarcts and cerebral atrophy12,31,32 we could not observe any association between syphilis reactivity with CeVD or neurodegeneration. Further studies are required to examine the mechanistic link between syphilis infection and vascular cognitive impairment, neurodegeneration and dementia.
Our study has some limitations. First, we used a memory clinic population, where there is a limited availability of cognitively-normal subjects. This may limit the generalizability of the study to the community. However, our comparison with community-dwelling non-demented subjects showed that the prevalence of syphilis reactivity was similar between non-demented memory clinic patients and EDIS subjects. Second, we did not perform CSF analysis to confirm the presence of central nervous system infection in all patients. Of those patients with syphilis reactivity referred for CSF analysis, only 21 patients underwent CSF testing and one patient had a positive CSF-VDRL examination. However, CSF testing is not invariably positive (5) and has been found to be negative in 28–78% of cases of neurosyphilis. 33 Third, we were unable to perform CSF analysis, brain autopsy, positron emission tomography scans and assess other brain inflammatory biomarkers to show biological evidence of neuroinflammation in our subjects. However in this study both CeVD and neurodegeneration were not associated with syphilis reactivity; thus, we propose a hypothesis for further study that neuroinflammation may be the cause of cognitive impairment and dementia in syphilis-reactive patients. Fourth, only a subsample of 580 cases had CT scans in standard digital format with coronal sequences which could be analysed for the association between syphilis reactivity markers of CeVD and neurodegeneration. Strengths of the study include our large memory clinic and community-based populations, and as such this is one of the few studies conducted in a memory clinic population. Second, all the patients underwent comprehensive physical, medical and neuropsychological assessment to rule out other causes of dementia; thus the chance of overdiagnosis of dementia was minimized.
Conclusion
The present study demonstrates an overall prevalence of 4.5% for syphilis reactivity in a memory clinic population and syphilis reactivity was significantly associated with dementia. Since CeVD or neurodegeneration did not appear to be associated with syphilis reactivity, neuroinflammation may be the cause of cognitive impairment and dementia in patients who are syphilis reactive, which requires further study. In addition to CSF analysis, brain biopsy and assessment of other brain inflammatory biomarkers research can be done to study the association between syphilis reactivity and neuroinflammation and dementia.
Supplemental Material
Supplemental material for Prevalence and association of syphilis reactivity in an Asian memory clinic population
Supplemental material for Prevalence and association of syphilis reactivity in an Asian memory clinic population by Bibek Gyanwali, Muhammad A Shaik, Saima Hilal, Jemellee Cano, Christopher Chen and Narayanaswamy Venketasubramanian in International Journal of STD & AIDS
Footnotes
Authors’ contributions
BG and MAS participated in data acquisition, performed analysis, drafted and revised manuscript. SH contributed in data analysis and revising manuscript. JC contributed in data collection. CC was responsible for study design and concept, overall supervision and revised the manuscript. NV was responsible for obtaining funding, provided intellectual advice, overall supervision and revised manuscript.
Acknowledgement
We acknowledge all the NUH memory clinic and Memory Aging & Cognition Centre co-ordinators for their contributions to subject recruitment and data acquisition.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: EDIS study was supported by the National Medical Research Council grants (grant numbers NMRC/CG/NUHS/2010, NMRC/CSA/038/2013 and NMRC/CG/013/2013).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.