
Abstract
The extent to which healthcare professionals (HCPs) and young people (YP) are aware of, and adhere to, National Chlamydia Screening Programme (NCSP) recommendations on testing frequency is unclear. To address this two cross-sectional surveys in 2015–2016: one among genitourinary medicine (GUM) and non-GUM HCPs (n = 109) and the other among YP attending a GUM clinic in England (n = 195). For both, questions were designed to measure awareness of NCSP guidance and whether respondents acted on that knowledge. This included questions about YP’s most recent test(s) (if ever) and the time since first and last sex with their most recent partners. Knowledge of NCSP testing guidelines varied among both GUM and non-GUM HCP respondents. However, lack of knowledge of the guidelines did not preclude HCPs from recommending testing in line with NCSP recommendations in practice. While most YP were not aware of NCSP recommendations, around two-thirds had tested for Chlamydia at least once in the last year. However, testing seldom appeared to coincide with partnership change. There is a knowledge gap and a discord between testing recommendations and practice. Interventions are needed to encourage appropriate testing patterns to maximise the individual and public health benefits of testing.
Keywords
Introduction
Chlamydia trachomatis is the most commonly diagnosed bacterial sexually transmitted infection (STI) in the UK with over 200,000 people diagnosed in 2016. 1 The greatest prevalence of infection is found among sexually-experienced 16–24 year olds (3.1% in women; 2.3% in men) 2 with the majority of those infected experiencing no symptoms. 3 Left untreated, Chlamydia can cause significant and costly adverse reproductive health problems including ectopic pregnancy and infertility. 3 Transmission may also occur to sexual partners and to the neonate. 3
In England, the National Chlamydia Screening Programme (NCSP) was introduced in 2003 with the aims of preventing and controlling Chlamydia through the detection and prompt treatment of infection in people aged 15–24 years. Reinfection among young people (YP) who have been treated for Chlamydia is estimated to be 10–30%. 4 As a result, the NCSP advises that all sexually-active men and women under the age of 25 are tested annually, on change of sexual partner and three months following treatment. 5 Adherence to NCSP guidelines is monitored through local, regional and national audit and surveillance systems.
NCSP aims to deliver high volume, high-quality screening to YP by embedding Chlamydia screening within primary care and sexual health services. The NCSP encourages commissioners and providers to use core services including: sexual and reproductive health services; internet testing; general practice; abortion services and community pharmacies.
Appropriate testing in accordance with the NCSP recommendations may require knowledge of these recommendations among healthcare professionals (HCPs) and YP as well as the feeling that a test is needed in relation to sexual activity. There is little understanding of the testing patterns of YP in relation to the timing of sex with partners. For example, during a sexual health consultation, sexually-active YP will be asked when they last had sex, and the number of partners in the last three months will be documented. However, the timing of sexual health screens in relation to changes in partners is often undocumented. Individuals may have two or more sexual partnerships at a time (concurrency) which further adds to the challenges of understanding patterns of testing in relation to sexual partner change. 2 Timing of testing is crucial for the prevention of transmission and prevention of sequelae, as treatment after transmission events, or after upper reproductive tract damage has occurred, will have much less benefit for the same cost. In this study, we aimed to establish (1) HCPs’ and YP’s knowledge of NCSP testing recommendations; (2) testing practices among HCPs in relation to knowledge of guidance and (3) testing practices among YP in relation to timing since first sex with most recent sexual partner.
Methods
We conducted two cross-sectional surveys in 2015–2016: one among HCPs and the other among YP attending a genitourinary medicine (GUM) clinic. In both surveys, questions were designed to measure awareness of the NCSP testing guidance and whether respondents acted on that knowledge. Both questionnaires were piloted with a small group of HCPs and YP in order to optimise question wording and improve survey validity.
HCP survey
This was an online survey of HCPs working in GUM and Sexual and Reproductive Health across England (see online Appendix 1). HCPs were invited between December 2015 and April 2016 through the British Association of Sexual Health and HIV (BASHH) and Faculty of Sexual and Reproductive Health (FSRH) newsletters and snowball sampling. We asked respondents whether they could correctly identify age limits for Chlamydia screening (15–24 years) and used hypothetical scenarios to determine HCPs’ awareness of and adherence to NCSP recommendations for testing annually, on change of partner and re-testing following treatment for an infection. Respondents were categorised as being aware of each recommendation if they responded correctly to each scenario. Respondents were then informed of the NCSP recommendation and asked whether, in practice, they always/sometimes/rarely/never recommended testing in the specified way (e.g. on change of sexual partner) to their patients, regardless of whether they were aware of NCSP guidance.
YP survey
This was a clinic-based convenience survey of young adults attending a GUM clinic in Bolton, a large town in Greater Manchester, UK, with areas of high-level deprivation. We used a self-completion pen-and-paper questionnaire (online Appendix 2), which the reception staff distributed to all those aged 15–24 years who attended the clinic between 26 May and 8 July 2016. We anticipated this would result in a sample of ∼200 patients, which we believed would provide a sufficient level of precision for the purposes of this exploratory study. A sample size of 200 patients would be sufficient to estimate a 20% proportion who report having/expecting to have a Chlamydia test upon change of sexual partner to within 6 percentage points; a 50% proportion can be estimated within 7 percentage points. The survey included questions about YP’s awareness of NCSP recommendations, and their history of Chlamydia testing and diagnosis. The time between commencing a new sexual partnership and having a Chlamydia test represents a period when a young person is at risk of any newly-acquired infection going untreated. We therefore explored the timing of testing in relation to sexual partnership formation by asking respondents to report the time (days/weeks/months) since the first and last sex with their most recent sexual partner(s) (at most three) and most recent Chlamydia test(s) (again, at most three). These data were then used to estimate the time between the most recent test and first sex with their most recent partner. Given the approximate nature of these data, and because they are potentially subject to recall bias, the following broad categories were used: the test occurred (1) ‘well over a year after first sex’; (2) ‘around one year after first sex’; (3) ‘around six months after first sex’; (4) ‘a couple of months after first sex’; (5) ‘at the time of first sex’; (6) ‘a couple of months before first sex’; (7) ‘around six months before first sex’; (8) ‘around one year before first sex’; (9) ‘well over a year before first sex’.
Ethics approval was not required for the HCP survey as this was conducted as a service evaluation of NCSP delivery. Ethics approval for the YP survey was obtained from North West – Greater Manchester Central NHS Research Ethics Committee, reference number 16/NW/0217.
Descriptive analyses were performed using Excel and Stata, specifically, percentages were calculated and where applicable compared using the chi-square test. Statistical significance was considered as p < 0.05. The average age at first sex was calculated as the median with the inter-quartile range used as a measure of spread, among participating YP who reported that they had had sex as this was all but two of the sample.
Results
HCP survey
One hundred and nine HCPs completed the online questionnaire. Of these, 69 were GUM HCPs (64 doctors; 4 nurses; 1 health advisor) and 40 were non-GUM HCPs (26 doctors, including 7 GPs; 14 nurses).
Awareness of the key NCSP recommendation that 15–24 year olds should be tested annually was low among HCPs: only 19% of respondents accurately identified the recommended age group for the NCSP and only 26% reported being aware of the recommendation to test annually (Table 1). A higher proportion of HCPs were aware of the need to test on change of partner (70%) and three months after a diagnosis (58%). There was no statistically significant difference in awareness of guidance for age limit, annual testing or re-test between specialties (GUM vs. non-GUM). However, there was a statistically significant difference (p = 0.007) between specialties with regard to awareness of re-test requirements.
Awareness of NCSP guidance and reported frequency of recommending testing to patients in practice (healthcare professionals survey).

GUM: genitourinary medicine; NCSP: National Chlamydia Screening Programme.
aTotals do not necessarily sum to total respondents in each group due to item non-response.
bIncludes two who reported that they assumed another HCP would arrange this. For example, 14–25 years, 15–26 years.
Despite relatively low awareness of some of the specific recommendations, the proportion of respondents who reported that they sometimes or always recommended testing annually, on change of sexual partner and three months after a positive test was relatively high in both those who were aware of recommendations and those who were not (Table 1).
YP survey
Six hundred and eighty patients aged 15 to 24 years attended the clinic during the study period; 195 (29%) completed the paper questionnaire. As shown in Table 2, YP had relatively low levels of awareness of the NCSP recommendations to test annually (12%) and on change of partner (37%). However, annual testing was still reported by 66% of respondents in the YP’s survey and 56% reported having been tested for Chlamydia in the last year. Three-quarters of respondents indicated they would be happy to be offered a Chlamydia test each time they saw a doctor or nurse.
Respondent characteristics, awareness of NCSP recommendations, reported testing and diagnosis histories (YP survey).
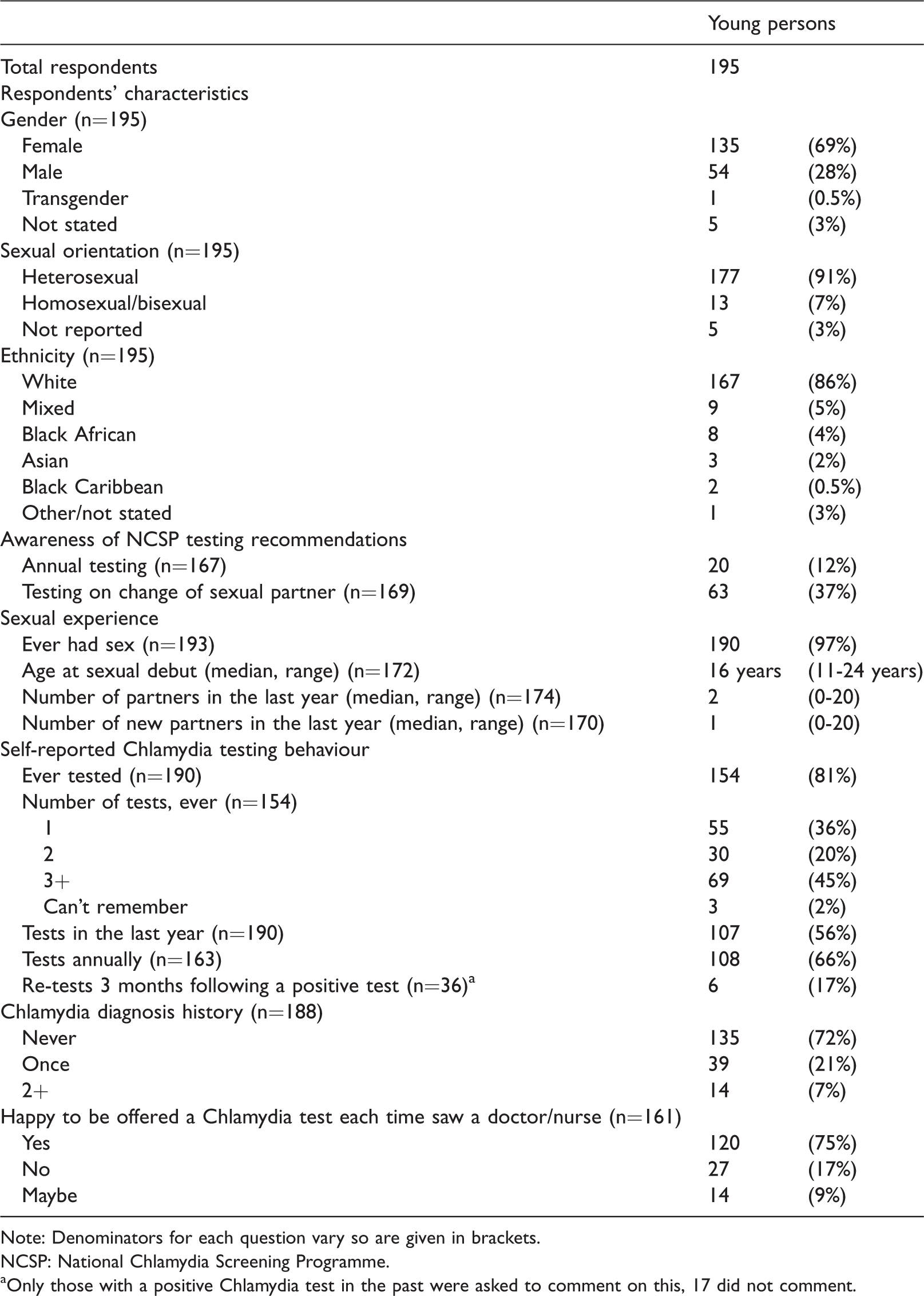
Note: Denominators for each question vary so are given in brackets.
NCSP: National Chlamydia Screening Programme.
aOnly those with a positive Chlamydia test in the past were asked to comment on this, 17 did not comment.
In total, 117 respondents had valid responses on both the timing of their most recent Chlamydia test as well and the timing of first sex with their most recent partner enabling the relative timing of Chlamydia test to be established for these YP. On average (median), respondents’ most recent test was around six weeks after first sex with their partner; however, there was substantial variation. As shown in Figure 1, while 24% reported having had a Chlamydia test within a few months of first sex occurring with the partner, 31% had not been tested since having sex with the partner and 45% had been most recently tested around six months to well over a year after first sex with the recent partner.

Timing of Chlamydia test (most recent if more than one) relative to first sex with most recent partner.
Discussion
Knowledge of NCSP testing guidelines varied among both GUM and non-GUM HCP respondents in our cross-sectional survey. However, in practice, lack of knowledge of the guidelines did not preclude HCPs from recommending testing in line with NCSP recommendations. The majority of respondents to the YP survey were not aware of NCSP recommendations. However, around two-thirds had been tested for Chlamydia at least once in the last year, suggesting that knowledge of the NCSP guidance is not a pre-requisite for health-seeking behaviour in this clinic-attending population. Our comparison of reported testing history in relation to sexual partnership formation suggested that Chlamydia testing seldom coincided with partnership formation.
These surveys collected information from two populations that are key to the success of the NCSP. The YP survey was the first study that we are aware of that has attempted to look in detail at the timing of Chlamydia testing in relation to sexual partnerships in the context of the NCSP.
There were, however, some limitations. With regard to the HCP survey, we are unable to quantify the response rate, since we do not know how many emails were sent out via the BASHH and FSRH newsletters. We do know that no reminder emails were sent in this time. The resources available for our exploratory study meant that we were limited to using a convenience sample and so knew that we would not achieve views that were representative of HCPs across England. The relatively small sample size limited our ability to explore differences between professional groups. However, incomplete awareness of, and adherence to, recommendations were seen among both GUM and non-GUM professionals, suggesting there is room for the NCSP to improve awareness among HCP from both groups. Our findings may also be biased towards an overestimate of awareness and adherence to recommendations; we aimed to reach a sample that was representative of HCPs working in sexual health by accessing them through professional bodies but response bias may have occurred as people who are aware of the guidance may have been more inclined to complete the survey. Additionally, we used scenarios to test respondent awareness, which did not leave room for nuanced views. Although we piloted the questionnaire to try to optimise question validity, it is possible that respondents have some awareness of the recommendations but that they responded in a way we would not have expected. For example, we provided a graph for HCPs to mark on where they felt the age range for testing within the NCSP fell. It may well have been more appropriate to ask for a written response for the lower age limit and for the higher age limit. We have recognised in our data when a respondent identified the age limits within a year of each end of the actual age range.
The YP’s survey has limited generalizability, because the sampling frame was clinic attendees who attended one particular clinic in England and the number of YP who filled in the survey was relatively small. Our analyses are based on a convenience sample of YP attending a GUM clinic and so are also at greater risk of having chlamydia than the general population or than those attending other services for testing. 6 As with the survey of HCP, the YP’s survey is subject to response bias as young persons more aware of the NCSP may have been more inclined to participate in a survey about Chlamydia testing. We do not know the number of patients offered the survey in the study period due to variations in reception staff and their awareness of the study, despite regular reminders.
Capturing information on the timing of events is particularly challenging, especially those not regarded as particularly salient or all that recent, for example, sexual debut. Thus, while we would have ideally had precise dates of testing and when people first and last had sex with their recent sexual partner(s), we instead asked respondents to estimate the time since testing and first sex with their partners such that we were only able to approximate the relative timing of testing. To minimise recall bias further and to reduce the proportion of the sample with missing data, we limited our analyses to the most recent of these events, but even then, data were only available for 60% of our total sample. By only taking account of the most recent Chlamydia test, we may have overlooked earlier tests that occurred just before or soon after first sex with the most recent partner. Additionally, we could not fully capture an individual’s risk as we did not collect data on reasons for not yet having tested, which might include knowledge that their partner had been tested recently or continuous use of condoms. Despite these limitations, we identified some interesting features of the relative timing of Chlamydia testing, chiefly that there is substantial variation, suggesting that neither anticipating nor having sex with a new partner trigger testing for Chlamydia. These data therefore imply that the recommendation of ‘testing on change of sexual partner’ may rarely occur in practice. This represents potentially missed opportunities to interrupt transmission and the potential for infections to go untreated for several months, with the associated risks of developing complications such as pelvic inflammatory disease in women or epididymitis in men.
Our findings suggest there is room for improvement in relation to awareness of NCSP recommendations among both HCPs and sexually-active YP. Given this knowledge gap and a discord between testing recommendations and testing practice, further work is needed to develop targeted interventions with both HCPs and YP to support appropriate testing patterns in clinical practice. However, the relatively high proportions of respondents who were recommending/accessing testing also highlight that the relationship between knowledge and behaviour is not straightforward. The ‘COM-B’ model proposes that behaviour (B) is the result of an interaction between three components: capability (C), opportunity (O) and motivation (M). 7 HCPs and YPs must have adequate knowledge (capability) the physical and social opportunity and the appropriate want or need (motivation) in order for Chlamydia testing to occur. Because low levels of knowledge among HCPs did not necessarily inhibit testing it may be that interventions to try and increase knowledge do not help to significantly improve testing rates. Interventions which address the motivation to test by increasing the perceived need or want to test following or before sex with a new partner may be useful for YP. In addition, targeting underlying beliefs (motivation) and peer norms (opportunities) around sex and relationships may also be helpful. Qualitative work with both HCPs and YP would be useful to develop a better understanding of how both groups interact with NCSP recommendations and how best to implement guidelines in a way that results in testing in line with recommendations.
Further work to capture the complexity of testing in relation to sexual partnerships would be fruitful to better understand transmission risk and the potential duration of untreated infections. Better ways of capturing data on timing of testing in relation to partnership formation are needed, along with sufficient numbers of people who have been diagnosed, which would allow better understanding of how long people have untreated infections for. This would likely require some more in-depth qualitative work to develop the conceptual frameworks around testing practices, including focus group-based discussions. This would in turn be useful to improve recommendations to YP and HCPs regarding when Chlamydia testing should be recommended.
Key messages
This is the first piece of research evaluating HCPs and young persons’ awareness of the NCSP. HCPs have variable awareness of the NCSP guidance. GUM clinic-attending young adults were found to report testing relatively frequently. Chlamydia testing among these young persons rarely coincided with partner change.
Supplemental Material
Supplemental material for Do healthcare professionals and young adults know about the National Chlamydia Screening Programme? Findings from two cross-sectional surveys
Supplemental material for Do healthcare professionals and young adults know about the National Chlamydia Screening Programme? Findings from two cross-sectional surveys by Susanna Currie, Catherine H Mercer, Kevin J Dunbar, John Saunders and Sarah C Woodhall in International Journal of STD & AIDS
Footnotes
Acknowledgements
We thank all survey respondents as well as the Genitourinary Medicine Department at The Royal Bolton Hospital, the British Association of Sexual Health & HIV and the Faculty of Sexual & Reproductive Health for their assistance.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Greater Manchester Central NHS Research Ethics Committee, reference number 16/NW/0217.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.