
Abstract
Background
Tubal infertility and ectopic pregnancies are serious, but rare, complications of chlamydia infections. It is unclear whether chlamydia screening in women has an impact on these complications. Chlamydia incidence rates between European countries vary by orders of magnitude, which largely reflects different intensities of screening.
Methods
We used chlamydia diagnoses rates as a proxy for chlamydia screening rates to assess if differences in screening intensity were associated with differences in the frequency of ectopic pregnancy and the prevalence of infertility in women. We used mixed effects linear regression to assess for an association between chlamydia screening intensity in European countries and two outcomes: (1) the incidence of ectopic pregnancy and (2) the prevalence of infertility in women, while controlling for year, income and quality of health services.
Results
The number of countries with available data increased from 3 in 1990 to 23 in 2019, before slightly declining to 22 in 2020. CT incidence varied across countries, from a median of 207 cases per 100,000 in 1990 (IQR: 59–313) to 33 cases per 100,000 in 2021 (IQR: 3–179). There was less variation in ectopic pregnancy incidence (median: 208 and 33 per 100,000 in 1990 and 2021, respectively), and female infertility prevalence (median 1,224 and 1,587 per 100,000 in 1990 and 2021, respectively). No association was found between screening intensity and ectopic pregnancy incidence or infertility prevalence after adjusting for year, GDP per capita, and universal health coverage index.
Conclusions
Our results are compatible with other types of data that suggest that the intensity of screening for chlamydia is not associated with a large effect on the population-level frequency of all ectopic pregnancies and female infertility.
Introduction
It is increasingly questioned as to whether or not asymptomatic women should be screened for Chlamydia trachomatis (CT).1–3 International guidelines stipulate that screening programs should only be introduced once high-quality randomized controlled trials (RCT) have established that screening is effective in reducing mortality or morbidity. 4 The primary reason to screen for CT is to reduce ectopic pregnancies and tubal infertility. 1 No RCT has ever been conducted to evaluate the efficacy of screening CT in women to reduce the incidence of ectopic pregnancy and tubal infertility. 1 Four RCTs have been performed to evaluate if screening for CT reduces the incidence of pelvic inflammatory disease (PID). 5 A systematic review of these studies found that screening was associated with a reduced incidence of PID in two of the studies. 5 Both these studies were at moderate risk of bias, whereas in the two studies at low risk of bias, no effect was seen on PID. Another reason for screening is to reduce prevalence. Two large cluster RCTs have been conducted to evaluate the effect of screening for CT in general populations.6,7 Both found no significant impact of screening on the prevalence of CT. In one of these studies, 5,704 women were followed up for 14 years with regular assessment for CT infection and complications of CT. 8 This NECCST study found that a high proportion of the population (37%) had contracted CT infection, but the incidence of PID, ectopic pregnancy and infertility were all low. These adverse outcomes were associated with symptomatic CT infections but were not associated with only asymptomatic infections. Different study types have also provided evidence that screening may arrest the development of immunity to CT, which may paradoxically increase the risk of subsequent infection.9,10 On the basis of these and other results, the Netherlands has recently stopped screening asymptomatic men and women for CT. 11
England has also reevaluating its chlamydia screening programme. Since its inception in 2003, the National Chlamydia Screening Programme (NCSP) has significantly increased the rate of chlamydia testing among young individuals aged 15–24 years. 12 For some years during, more than one million tests have been conducted on young people, with estimated coverage reaching up to 30% among young women in peak activity years. 12 Previous mathematical modelling studies had suggested that this level of screening uptake would be sufficient to reduce the overall prevalence of chlamydia within the population. However, evidence reviewed in 2019 including findings from two population-based surveys conducted as part of the British National Surveys of Sexual Attitudes and Lifestyles found an absence of evidence indicating that chlamydia prevalence had not declined between 2000 and 2011. 13 In response to these findings, the NCSP is in the process of redefineding its strategic priorities. 1 This includes changing its primary aim to focus on reducing harms from untreated CT within young women. 14
The low incidence of ectopic pregnancy and infertility, and the low attributable fraction of these outcomes to chlamydia infection (around 5%), and the long time period till these outcomes are apparent, means that impossibly large sample sizes and data completeness and accuracy, and very long follow-up periods would be required for RCTs to have the power to assess the efficacy of screening CT on these outcomes. Such RCTs are, therefore, impractical. 1 The reported incidence of CT varies by orders in magnitude between European countries (between 0.02 and 627 cases/100 000 inhabitants in 2021). 15 This provides an interesting natural experiment to evaluate if the reported CT incidence (as a proxy for screening intensity) is associated with reduced rates of ectopic pregnancy and infertility. In this paper, we use multiple data sources to test this hypothesis.
Methods
We conducted a country-level ecological analysis of CT incidence (as a proxy for chlamydia screening rates) and two outcomes: (1) the incidence of ectopic pregnancies in women and (2) the prevalence of female infertility.
Our data came from 3 sources.
C. trachomatis incidence
The European Surveillance System (TESSy) of the European Centre for Disease Prevention and Control does not collect data on CT screening. 15 However, it collects data on the incidence of CT per 100,000 population for 24 countries using a comprehensive surveillance system and a standard case definition of CT infection. 15 Three countries (Belgium, France and the Netherlands) reported data derived from sentinel systems that only capture a proportion of all chlamydia diagnoses. In Italy no rate was calculated until the year 2023. National chlamydia incidence for these four countries is therefore not calculated.
A number of population-based surveys in European countries have found that the prevalence of CT in general populations is very similar.16–18 For example, a systematic review of studies based on nationally representative surveys in Europe found that the point prevalence of chlamydia in women aged 18–26 years ranged from 3.0 to 5.3% in different countries.17,19 A more extensive systematic review that has not been peer-reviewed was recently published by the European Center for Disease Prevention and Control. 20 This review found that the median prevalence of chlamydia in women was 2.81% (95% CI 1.71–3.91), and in men was 2.67% (95% CI 0.65–4.69).
This same review found that the prevalence of CT was similar between countries in key populations, such as MSM on HIV PrEP. 20 If this is the case, then the number of cases of CT diagnosed per country per year will be heavily influenced by how intensively the population is screened for CT. 15 TESSy does not provide the proportion of CT infections that are symptomatic. 15 TESSy has data on transmission category for only around a third of infections, and all these come from a limited number of countries. 15 It is unlikely that the proportion of infections that are symptomatic will differ between countries. We, therefore, made the assumption that the incidence of CT in the TESSy data can be used as a proxy for the intensity of CT screening. The indicator used was a crude number of cases of CT/100,000 per year for women of all ages. 15
Incidence of ectopic pregnancies and prevalence of female infertility
The incidence of ectopic pregnancies and prevalence of female infertility per country and year in 15–49 year old women were obtained from the Global Burden of Diseases (GBD) study. The GBD defines an ectopic pregnancy as a pregnancy occurring outside of the uterus. The indicators used were: cases of ectopic pregnancy/100,000 women per year, prevalence of female infertility per 100,000 women (https://www.healthdata.org/research-analysis/gbd-data).
Income and quality of health services
Differential quality of health care services and income may be associated with infertility and ectopic pregnancy. 21 We used the Universal Health Coverage (UHC) Service Coverage Index to control for quality of health care and GDP per capita (current US$) to control for income levels (https://data.worldbank.org/indicator).
The UHC is a composite indicator developed by the World Health Organization (WHO) to measure how well a country’s population has access to essential health services. The index is measured on a scale from 0 to 100, where 100 represents full coverage of essential health services. When data was missing for this indicator, the value for the first following year with data available was used.
Data analysis
In two separate analyses, mixed-effects linear regression was used to assess the correlation between ectopic pregnancy incidence/ female infertility prevalence and CT screening intensity controlling for year, UHC and GDP per capita. The CT screening intensity data from 3 years prior to the outcome data was used for all analyses to account for the delay between CT infection and complications. 1
The following mixed-effects linear regression model was used:
(ectopic pregnancy incidence/ female infertility prevalence in year Y and country C)˜
(CT screening intensity in year Y − 3 and country C) (residuals (ar 1, t (year)) + (random intercept for country C) + intercept + error.
The same model was used to assess the correlations of national CT screening intensity, with year, UHC and GDP per capita as predictors.
The data for the incidence of ectopic pregnancies were cube transformed, and the data for CT screening were square root transformed to create more normal distributions for these regression analyses.
We assumed that all missing data were missing at random; therefore, all missing data points were dropped from the analyses. All statistical analyses were performed in StataMP, version 16.0.
Results
Mean (Interquartile ranges) of key variables by country for the years 1990–2021.
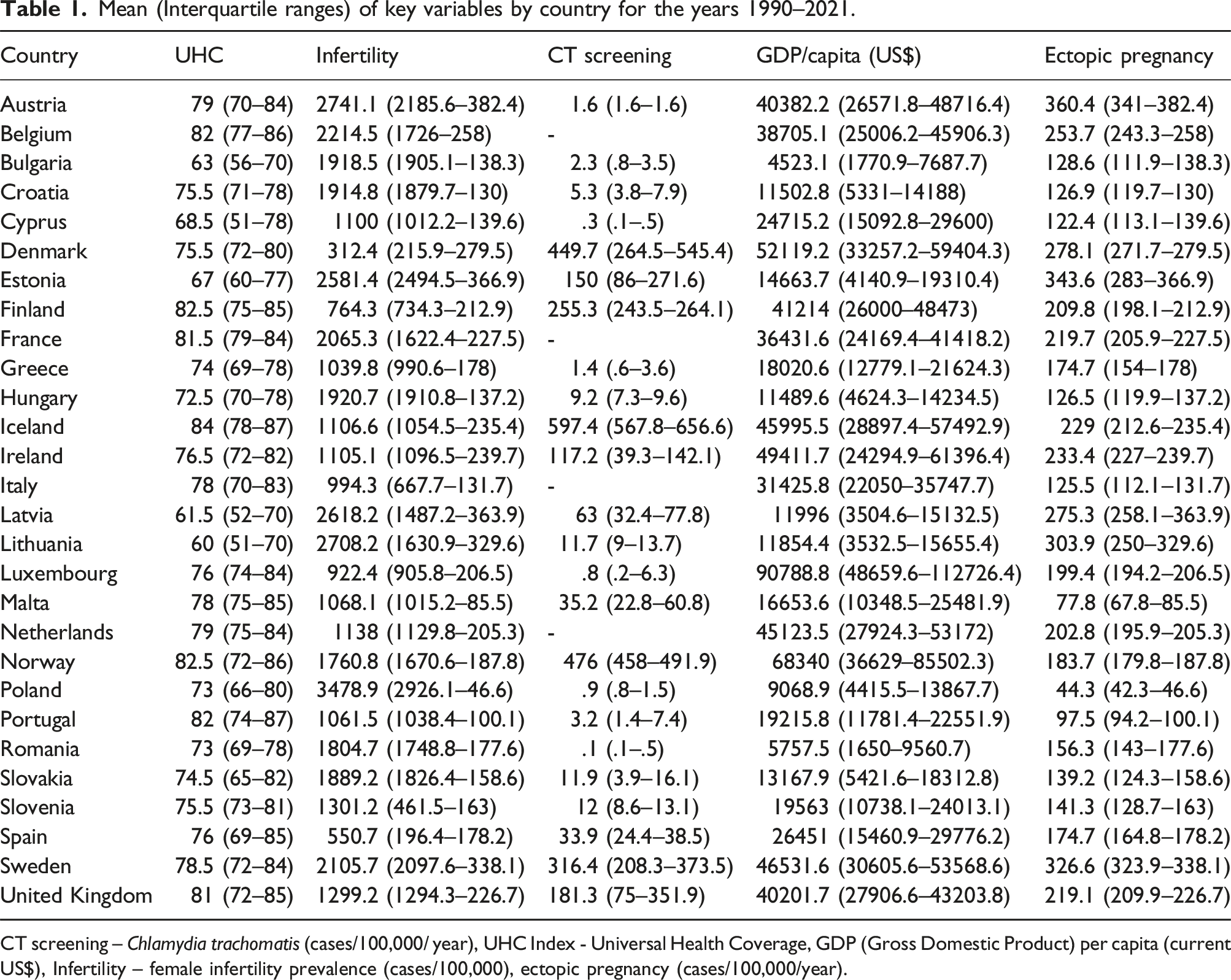
CT screening – Chlamydia trachomatis (cases/100,000/ year), UHC Index - Universal Health Coverage, GDP (Gross Domestic Product) per capita (current US$), Infertility – female infertility prevalence (cases/100,000), ectopic pregnancy (cases/100,000/year).

Longitudinal changes in C. trachomatis (CT) incidence (cases/ 100,000/ peryear) and the incidence of ectopic pregnancies (cases/ 100,000 women per year) (a) and the prevalence of female infertility (cases/ 100,000 women per year) (b) in countries in Europe.

Longitudinal changes in C. trachomatis (CT) incidence (cases/ 100,000 per year) (a) and the incidence of ectopic pregnancies (cases /100,000 women per year) (b) and the prevalence of female infertility (cases/ 100,000 women per year) (c) by European country.
There was less variation in the incidence of ectopic pregnancy (1990: median 208 cases/100,000 inhabitants, IQR 60–314 [n = 28]; 2021: median 33 cases/100,000 inhabitants, IQR 3–179 [n = 28]) and female infertility (1990: median 1224 cases/100,000 inhabitants, IQR 1142–1887 [n = 28]; 2021: median 1587 cases/100,000 inhabitants, IQR 1095–2114 [n = 28]; Table 1; Figure 1).
CT incidence increased in a number of countries, but there was little change in the incidence of ectopic pregnancies and the prevalence of female infertility over time (Figure 1).
Association between screening intensity and ectopic pregnancy/infertility
Mixed effects linear regression of factors associated with ectopic pregnancy, female infertility and chlamydia screening intensity in 24 European countries.
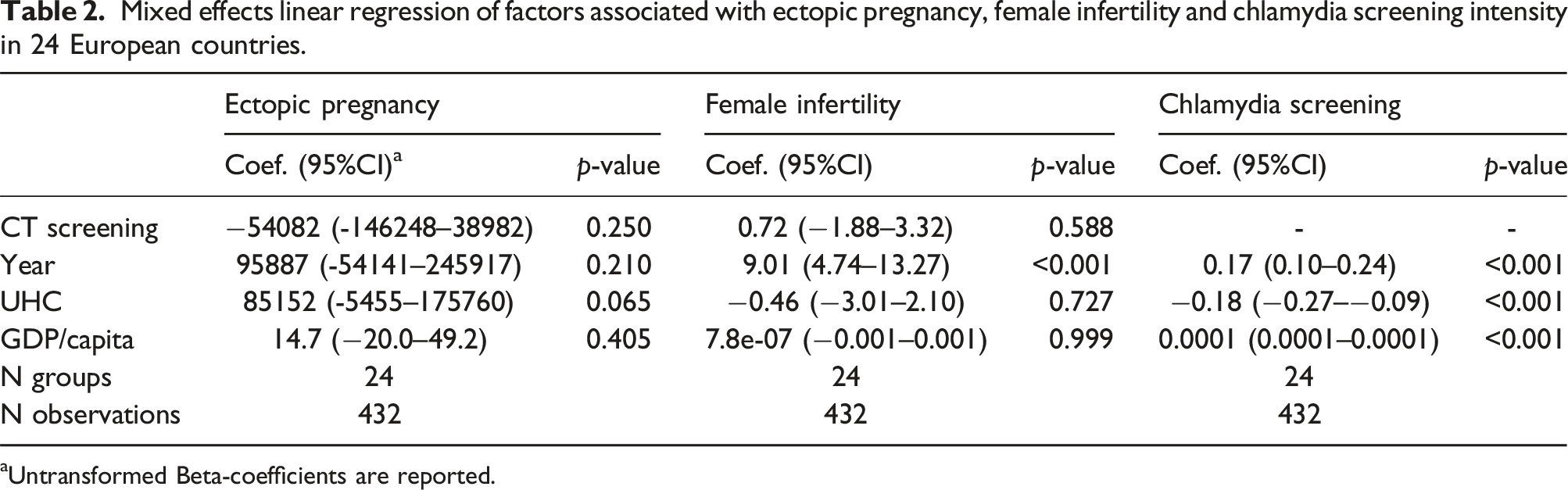
aUntransformed Beta-coefficients are reported.
The prevalence of female infertility was positively associated with year (p < .001) but not associated with CT incidence, GDP per capita, or UHD (Table 2).
Predictors of screening intensity
CT incidence was positively associated with GDP per capita and year and negatively associated with UHC (all p < .001; Table 2).
Sensitivity analyses using a lag of 8 and 12 years between CT incidence and the outcome variables produced similar results (data not shown).
Discussion
In this ecological analysis, we found that the intensity of CT screening varied by orders of magnitude between European countries, and this was associated with GDP per capita, UHC and year. We found that the intensity of CT screening was not associated with the incidence of ectopic pregnancies or female infertility. These findings add to other types of evidence that suggest that screening for CT does not have a large impact on the incidence of these outcomes.1,8
The largest caveat to this conclusion is that our variable for CT screening intensity is far from perfect. It is based on the assumption that the number of CT infections diagnosed is proportional to the number of CT tests performed. The authors of the ECDC surveillance reports conclude that the large differences (31,350-fold difference in 2021) in CT incidence between countries is likely due to differences in screening policy. 15 We cannot, however, exclude the possibility that the higher incidence of CT is indicative of a real higher incidence of CT in these countries. Other important limitations include the fact that we only controlled for a limited number of confounders and that the data for ectopic pregnancy and infertility are based on estimates obtained via complex algorithms used by the authors of the GBD. 22 These algorithms impute data for missing values. 22 As such, these estimates may be inaccurate. Whilst we had data for ectopic pregnancies and female infertility for all countries at all timepoints, this was only the case for CT incidence for 3 countries in 1990, increasing to 23 countries in 2020. CT is only responsible for a proportion of ectopic pregnancies and female infertility. As such our analysis would be less likely to detect a small effect of CT screening on these outcomes. There are a wide range of estimates as to the proportion of female infertility and ectopic pregnancies that are due to chlamydia. 23 One robust study from the United Kingdom that used CT serology in a case-control design, found that between 28% and 47% of excess cases of tubal infertility could be explained by CT infections. 23 The proportion of ectopic pregnancies attributable to CT is lower (5%–25%).24,25 The lower the proportion of cases due to CT, the more likely this will lead to a type II (false-negative) error. Our data for CT incidence was for women of all ages, whereas the infertility and ectopic pregnancy data was limited to 15–49 year old women. The key target population of CT screening is young sexually active women, typically under 25 years old. It would therefore have been more appropriate to have used data from this population age group for the CT testing/screening variable. A number of countries with relatively high numbers of tests were excluded from our analysis as their data is based on sentinel surveillance that has not been extrapolated to provide national testing estimates. The inclusion of these countries could have changed our results. Finally, being an ecological study, the study is susceptible to the ecological inference fallacy.
Despite these very significant limitations, our analysis did not find that the intensity of testing for CT was associated with a large effect on ectopic pregnancies and infertility. Studies have estimated that one thousand CT infections will be associated with two cases of ectopic pregnancy and five cases of tubal infertility. 5 It is unknown when tubal damage occurs in the natural course of CT infection. 1 Tubal tissue damage might already have occurred between the acquisition of the infection and CT detection. 1 This could explain the results of the NECCST study. As noted above, this study found that asymptomatic CT was not associated with an elevated risk of ectopic pregnancy or infertility. 8 In conclusion, this study does not add to evidence about the health benefit of chlamydia screening to the individuals who accept screening. Our results could, however, be tentatively interpreted as providing cautious reassurance that initiatives in the Netherlands and Belgium to reduce CT screening should not result in large increases in the frequency of ectopic pregnancies and all-cause infertility at the population-level.8,26
Footnotes
Acknowledgements
The authors thank the providers of the data for making this data accessible.
Authors contribution
CK, TV and SB contributed to the conceptualization and methodology. All authors contributed to the investigation. CK performed the formal analysis. All authors contributed to the writing of the manuscript, and all authors approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by routine funding
Data Availability Statement
All the data analyzed is available without restriction from the ECDC, WHO and GBD websites.