
Abstract
Syphilis rates have been increasing in men who have sex with men (MSM) in London. To describe risk behaviour and refine public health interventions, we conducted prospective enhanced surveillance of new syphilis cases in MSM attending selected London sexual health clinics (SHCs) between October 2016 and January 2017. Sexual health advisors (SHAs) completed 107 questionnaires. Eighteen per cent of respondents reported always using condoms, with lower use in HIV-positive (8%, 4/53) than HIV-negative men (33%, 14/52). Almost half of respondents reported condomless sero-discordant sex (46%, 33/72). The most frequent means of meeting new partners reported were venues (80%, 76/95), particularly bars or clubs (34%, 32/95), and apps or websites (79%, 75/95). Nearly a third of respondents reported engaging in group sex (32%, 30/95). Almost half reported drug use during sex (47%, 46/98), with HIV-positive men more likely to report use of the three main ‘chemsex’ drugs. The majority of respondents preferred health promotion information from SHAs (63%, 58/92) compared to other sources such as Google/Wikipedia and apps. Prevention activity should continue to focus on condomless sex, serosorting, multiple and overlapping partners, and chemsex. SHCs, particularly those serving HIV-positive men, are important sources for sexual health promotion advice.
Introduction
Syphilis rates have been increasing in England since the late 1990s, particularly in men who have sex with men (MSM), a rise which has accelerated over recent years, and concentrated in urban centres such as London. 1 From 2010 to 2015, syphilis rates in London increased by 163% (from 1067 to 2811 cases) and in 2015 London accounted for 56% of all syphilis cases in England. MSM are disproportionately affected by syphilis, accounting for 90% of cases diagnosed in London in 2015. 2
There have also been parallel increases in other sexually transmitted infections (STIs) in MSM in London in recent years, such as lymphogranuloma venereum (LGV) and gastrointestinal infections with Shigella, which can be sexually transmitted, and evidence that changes in risk behaviours have contributed to increased rates of transmission. 3 This suggests that risk behaviours may also be contributing to sustained high rates of syphilis in London. Syphilis infection is a marker of individual sexual risk behaviour and sex within sexual networks at risk and high rates underline the need for enhanced efforts across prevention, early testing, and treatment.
Historically, in response to rising rates of syphilis, two enhanced surveillance systems were put into place between 1999 and 2002 which provided additional information confirming that there was a high incidence of syphilis in MSM, high prevalence of HIV coinfection, and a high proportion of MSM using social/sexual networks to meet new partners.4,5
While demographics for syphilis infection in MSM in London are well described, 2 behavioural risk factors are insufficiently understood, and detailed information on risk behaviours of syphilis cases is not currently routinely collected. In the context of continued and increasing rates of syphilis infections in MSM, this lack of information is a barrier to ensuring that health promotion interventions are targeted appropriately. In 2016, the Public Health England-led syphilis control group agreed to establish enhanced surveillance for syphilis in London sexual health clinics (SHCs) to provide intelligence to refine prevention activity.
In 2016, HIV trends in MSM in London showed signs of change, which has potential to impact future prevention efforts. Several clinics in London reported decreasing HIV diagnoses in 2016, likely the result of combination prevention efforts, including: increased testing, earlier antiretroviral treatment initiation, high condom use with casual partners, access to HIV pre-exposure prophylaxis (PrEP) through the internet, and research trials providing access to PrEP. A similar trend has been seen in HIV rates in MSM nationally. 6 Syphilis diagnoses in MSM, however, have continued to rise.7–10
Methods
We undertook prospective sentinel enhanced surveillance of newly diagnosed infectious syphilis cases in MSM in London between October 2016 and January 2017. A case was defined as a new diagnosis of infectious syphilis in MSM at participating specialist SHCs. Infectious syphilis was defined as primary, secondary, and early latent stage syphilis. Sex was defined as oral, vaginal, or anal sex, although condom use questions focused on vaginal and anal sex. Group sex was defined as sex involving more than two people at one time.
An opportunistic sampling method was used to identify cases, targeting all clients newly diagnosed with syphilis at high volume specialist SHCs serving MSM, until at least 100 questionnaires had been completed. To establish the surveillance within clinic flow, a survey method of clinic staff integrating questioning into clinical practice was chosen. The sample size was chosen pragmatically to balance data requirements with feasibility of data collection within the allocated time period.
Staff at three central London specialist SHCs a diagnosing a high volume of MSM syphilis cases were contacted and invited to participate. Another clinic invited to participate, however, was unable to collect data due to staff time constraints.
A questionnaire was developed and piloted with input from all four specialist SHCs, recording sexual behaviour that previous reports suggested increase risk for transmission, 3 means of meeting new partners, and preferred means of accessing health information and messages. Paper or online questionnaires were completed at participating clinics by health advisors, dependent on staff time available to complete questionnaires and preference for online versus paper forms. Piloting was conducted in the same setting. Data collection started in October 2016 and continued for four months until the 100 questionnaire target had been met.
Information from paper questionnaires was entered into an online data entry questionnaire. Data were downloaded as a .csv file and analysed using STATA v13. Descriptive analysis of cases was undertaken.
Results
A total of 107 questionnaires were completed. Sixty per cent of questionnaires (64/107) were reported by Mortimer Market Centre clinic, 22% (24/107) from 56 Dean Street, and 18% (19/107) from Guy’s and St Thomas’ NHS Foundation Trust. While questionnaires from two of the clinics were largely complete, almost half (11/24) the forms from a third clinic did not report on group sex, sex work, venues, or apps to meet sexual contacts or substance use. Data gaps are likely to be due to the source of information being clinic notes supplemented by follow-up phone calls. Additional gaps in the data for all clinics included instances where a patient was not asked a question or declined to answer; the full reasons for gaps were not reported when questionnaires were submitted.
Current HIV status was recorded by clinic staff completing questionnaires for all but three respondents (n = 104). Of these 59 (57%) were HIV-positive. This varied considerably by clinic (26, 39, and 73%).
Overall 97% (97/100) of respondents reported sex with one or more people in the previous three months (Table 1). Of the three who reported no sexual contacts over this period, two reported sexual contacts in the previous 12 months. There was no difference in the number of sexual contacts comparing HIV-positive and HIV-negative respondents (p = 0.70, Mann–Whitney test).
Numbers of sexual contacts in the previous three months (n = 100).
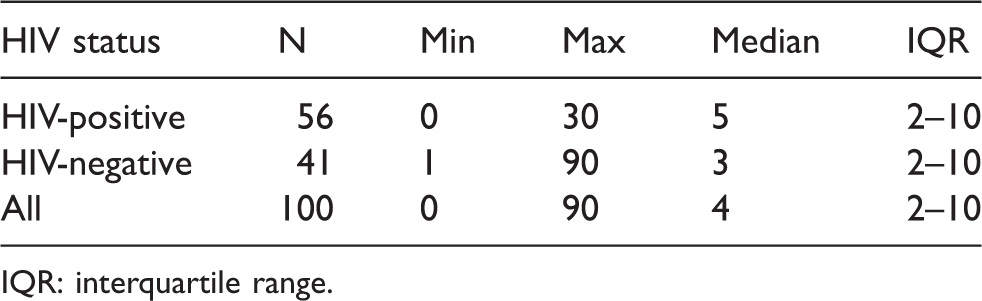
IQR: interquartile range.
Among those who reported sexual contacts in the previous three months, 81% (79/97) reported one or more traceable contacts, with a median of two contacts (IQR 1–5). There was no difference in the number of traceable contacts between HIV-positive and HIV-negative respondents (p = 0.75).
Eighteen per cent (18/98) of respondents reported always using condoms for anal or vaginal sex in the last three months. Eight per cent of HIV-positive men answering this question reported always using condoms, compared to a third of HIV-negative men (4/53 versus 14/42, p = 0.003) (Figure 1). Similarly, those respondents reporting anal or vaginal sex without condoms were 92% for HIV-positive and 67% for HIV-negative respondents. Never using condoms for anal or vaginal sex in the previous three months was reported by almost a third of HIV-positive men and 7% of HIV-negative men (16/53 versus 3/42, p = 0.009).
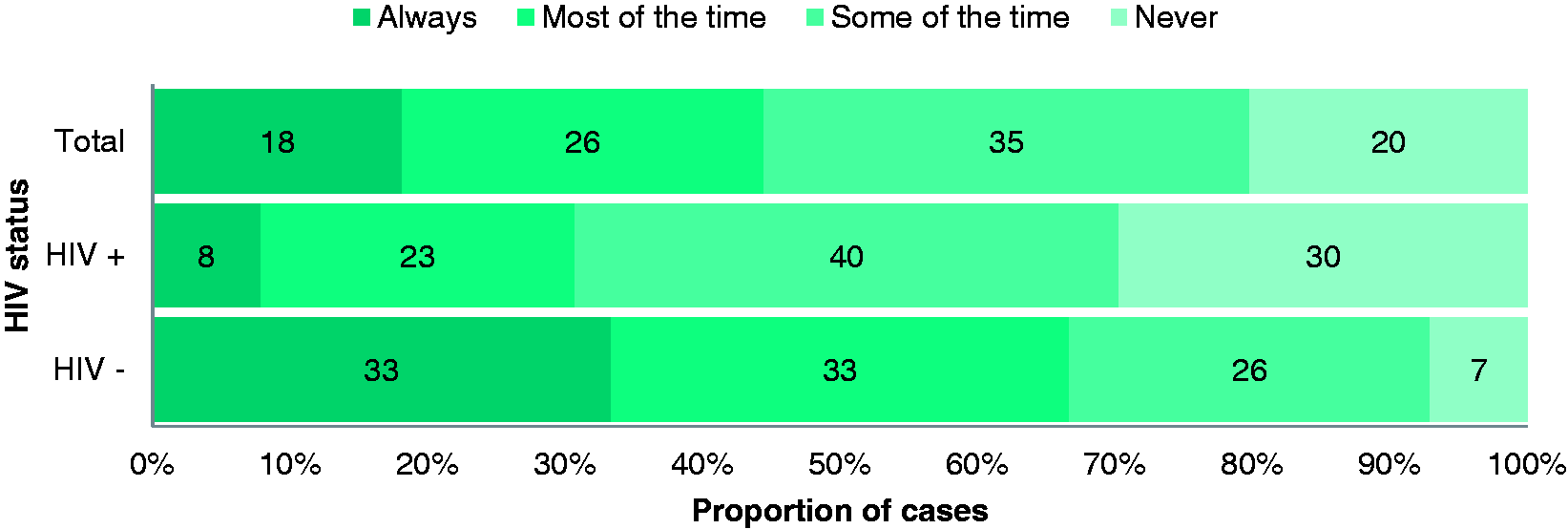
Frequency of condom use for sex in the previous three months by HIV status.
Eighty-nine patients responded to a question about sex without condoms with people of the same HIV status, including 14 who reported that they always used condoms for anal or vaginal sex in the previous three months (excluded from analysis). Of the remaining 72 respondents, 38% reported that all such partners were of the same HIV status as themselves (17/47 HIV-positive men and 10/25 HIV-negative men). Sero-discordant sex without condoms was reported by 46% of respondents (23 HIV-positive men and 10 HIV-negative men), with 17% reporting that they did not know (15% of HIV-positive men and 20% of HIV-negative men).
Information on whether they engaged in group sex in the previous three months was reported for 95 respondents. Of these 32% (30/95) reported group sex (36%, 20/55 in HIV-positive men versus 24%, 9/37 in HIV-negative men, Chi square = 1.49, p = 0.22). For those reporting engaging in group sex (19 HIV-positive and 9 HIV-negative), the maximum number of partners involved at one time ranged from 2 to 12 with a median of four (IQR 4–5).
Two individuals reported that they had been paid for sex in the previous three months. A further two reported that they had paid for sex during this period.
Ninety-one respondents reported using apps/websites or venues to meet sexual partners. Of four who did not, two reported no sexual contacts in the previous three months. For the remainder, the proportions using either apps/websites or venues to meet partners were similar (80% venues versus 79% apps), with venues significantly more frequent among HIV-negative men (92% versus 71%, Fisher’s exact p = 0.03) (Table 2).
Apps/websites and venues used to meet sexual partners in the previous three months.
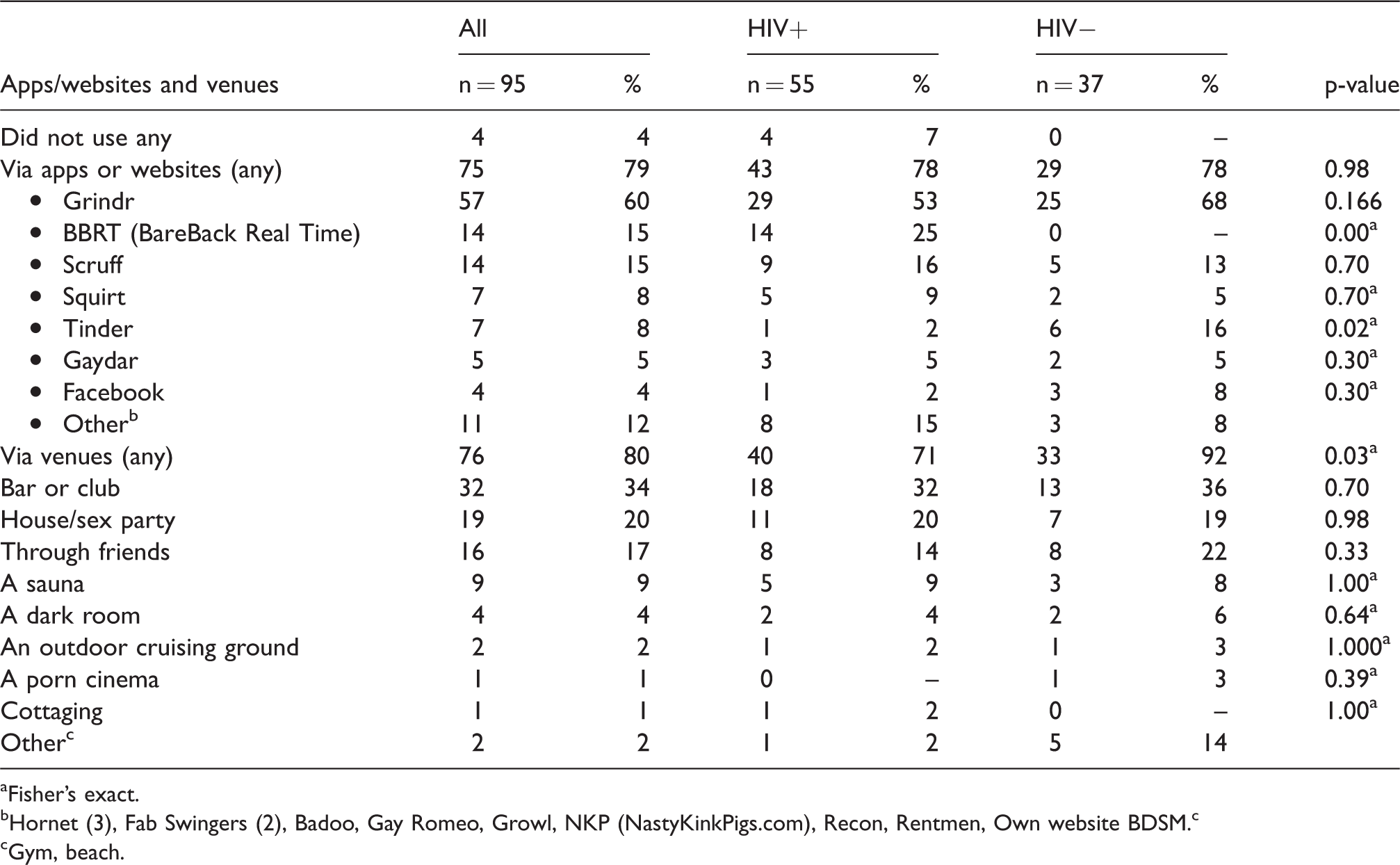
aFisher’s exact.
bHornet (3), Fab Swingers (2), Badoo, Gay Romeo, Growl, NKP (NastyKinkPigs.com), Recon, Rentmen, Own website BDSM. c
cGym, beach.
Among venues, meeting via bars and clubs was the most popular, followed by house/sex parties. Among apps and websites, Grindr was the most frequently used, followed by Scruff and BBRT, although the latter was not reported by any HIV-negative men, who in contrast were more likely to report using Tinder compared to HIV-positive men (16% versus 2%, p = 0.02).
Sixty-nine per cent of respondents (68/98) reported that they had used alcohol or drugs during sex in the previous three months, with equal proportions among HIV-positive and HIV-negative respondents. The most frequent substance reported was alcohol (45%), followed by mephedrone (28%), GHB/GBL b (28%), and crystal methamphetamine (25%).
Use of any drug during sex was reported by 47% (46/98) of respondents overall, with similar proportions by HIV status (30/56, 14/39, p = 0.089). However, HIV-positive men were more likely to report use of methamphetamine (30% versus 13%, p = 0.046) and almost twice as likely to report use of any of the three main ‘chemsex’ drugs 11 (46%, 26/56) compared to HIV-negative men (26%, 10/39, p = 0.040). Use of injected drugs was reported by five individuals (four of whom were HIV-positive), who all reported using methamphetamine.
Of the 92 individuals for whom this information was reported, the majority (63%) preferred to receive health information and messages about syphilis via a sexual health advisor (SHA) at a SHC (Table 3). This method was particularly popular among HIV-positive men, among whom 75% expressed a preference for this means. For those who did not indicate this means, use of Google/Wikipedia was the most frequent alternative.
Preferences for accessing health information and messages about syphilis (n = 92).
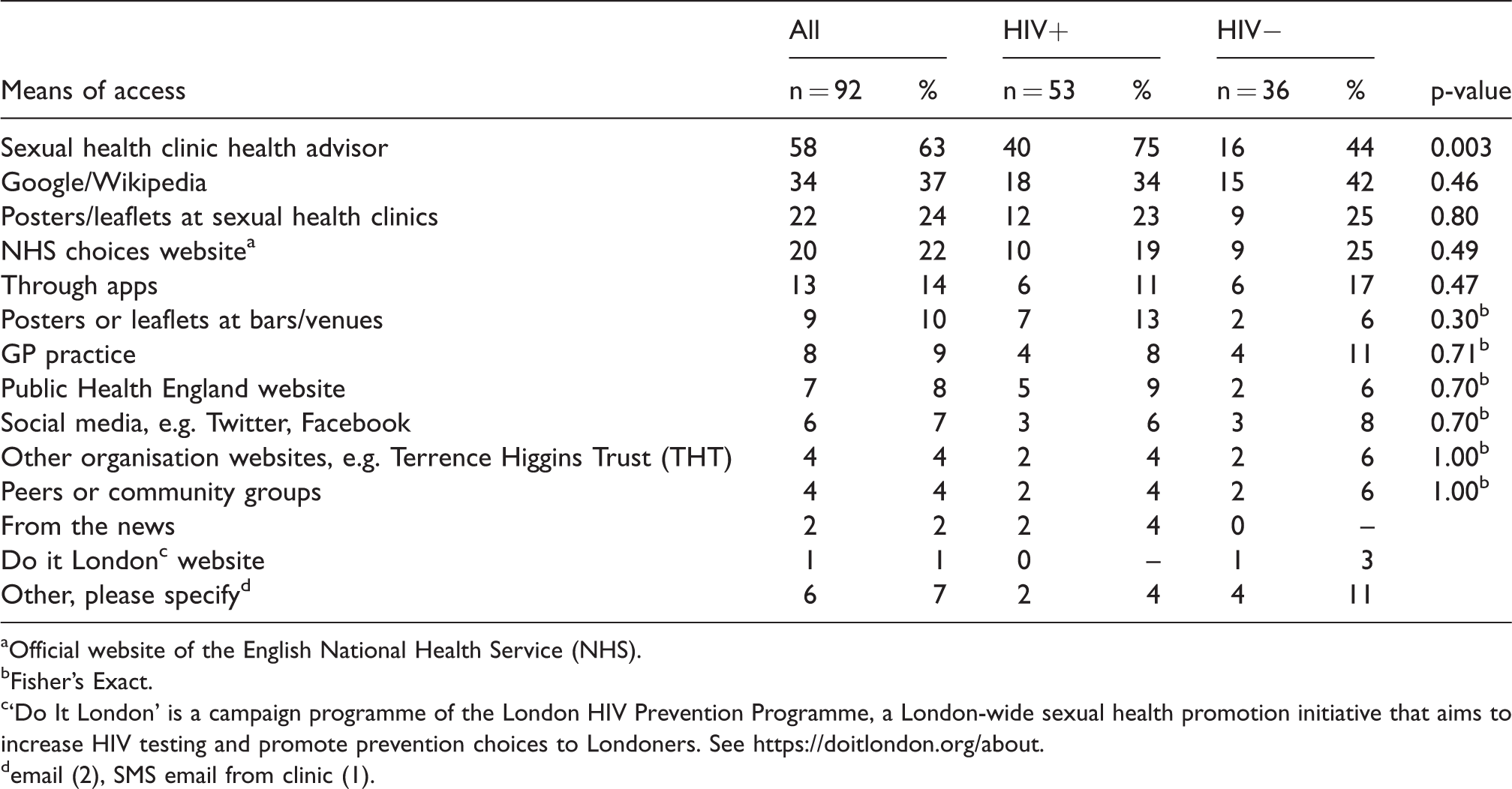
aOfficial website of the English National Health Service (NHS).
bFisher's Exact.
c‘Do It London’ is a campaign programme of the London HIV Prevention Programme, a London-wide sexual health promotion initiative that aims to increase HIV testing and promote prevention choices to Londoners. See https://doitlondon.org/about.
demail (2), SMS email from clinic (1).
The main reasons for clinic attendance reported were for a routine STI screen, reported by almost half, and being symptomatic, reported by a third. Partner notification was reported as the reason for attending by 8% of all respondents overall (9/107). This proportion was higher than the proportion of cases identified through partner notification in London overall (5%). 2 Four respondents reported attending due to a referral from another health professional (4/23).
Discussion
This enhanced surveillance of MSM diagnosed with syphilis at high volume central London clinics provides important information to inform content and channels of health promotion and messaging. The information collected complements existing demographic information, particularly by providing current information on sexual risk behaviours, and specific preferences for receiving health promotion messages.
Lack of condom use, serosorting, multiple partners and group sex (including where partners are untraceable), chemsex, and the use of apps to meet sexual partners may be important factors in fuelling the rise in syphilis in MSM. This is consistent with factors associated with outbreaks of other infections in MSM in London such as LGV and Shigella,3,5 as well as contributing factors cited in increases in syphilis in MSM seen in the U.S. and Western Europe,12–14 however, do not negate the likely contribution of high-risk sexual networks.
The proportion of respondents surveyed who were HIV-positive (57%) is comparable with the 51% of syphilis HIV coinfection identified in MSM in London in 2015. 2 HIV-positive men were significantly more likely to report they had engaged in sex without condoms, and for a third, to report the complete absence of condom use in their recent sexual relations. The reported HIV status of the partners involved indicated a degree of serosorting was occurring; however, only 36% of the HIV-positive men engaging in sex without condoms reported that this was always with people of the same HIV status. A similar proportion, 40%, of the HIV-negative men engaging in sex without condoms reported that this was always with people of the same HIV status.
The level of condom use reported both in HIV-positive and HIV-negative men was lower than has been reported previously in MSM in London and Europe.15–17 This is likely to reflect the higher risk population targeted in surveillance of syphilis cases and may also reflect changing risk patterns over time. For respondents who knew the HIV status of their sexual partners, both sero-concordant and sero-discordant sex without condoms were also higher than previously reported.15,16 The higher level of condom use in HIV-negative respondents in comparison to HIV-positive respondents was consistent with previous studies. 15
Almost a third of respondents (32%, 30/95) reported group sex, similar in both HIV-positive and HIV-negative respondents. This is consistent with levels reported in enhanced surveillance of Shigella flexneri outbreaks in MSM in England and Wales. 18 Although transmission routes for syphilis and S. flexneri differ, both can be sexually transmitted and can be a reflection of high-risk sexual behaviours. Median numbers of sexual partners reported, while lower than reported in Shigella enhanced surveillance, were consistent with levels reported for MSM in England overall.18,19
Given the range of opportunities for MSM to meet sexual partners in London, it is perhaps not surprising that no particular type of venue was revealed as contributing to syphilis transmission. Dating apps were commonly used, and those more frequently reported can potentially be used as channels for health promotion messages.
Reported drug use in respondents was consistent with high rates reported previously in MSM attending London SHCs, as was the higher rate of use of ‘chemsex’ drugs in HIV-positive men in comparison to HIV-negative men. 20 The use of any drugs or alcohol reported during sex was low in the context of overall drug and alcohol use reported by MSM in England in the Gay Men’s Sex Survey, 21 although comparable to reported drug and alcohol use during sex reported in the MRC Gay Men’s Sexual Health Survey (Scotland, 2011). 22 This may reflect under-reporting due to social desirability bias, as questioning was performed by healthcare staff.
Despite the popularity of apps like Grindr, only a minority reported that they would prefer to receive health promotion messages through such means. Sixty-three per cent overall and three-quarters of HIV-positive men preferred to receive such information from a SHC/SHA. Respondents were surveyed in clinics by SHA, and as such this may reflect a sample population with familiarity with and trust in clinics and their staff. However, this may also reflect a diversity of preferences for health promotion messaging between the population reflected in this surveillance and that reflected in other existing studies. Within the literature, several exploratory studies have evaluated the potential for social media targeting of sexual health messaging, including for MSM.23–27 Effective messaging campaigns utilised targeting of populations (e.g. MSM) and situations (e.g. when anonymity is desired) with social media messaging to reflect target population preferences.26,27
Half the sample reported attending clinic for a routine STI screen, and a third reported attending because they were symptomatic. The finding that only 8% attended because of partner notification suggests there is scope for more effective means of facilitating partner notification among MSM at risk of syphilis in London, although the lack of traceability of partners is an obvious limitation. This is important in the context of continuing increases in diagnoses of syphilis in MSM in SHCs in London, which reached 2557 in 2016. 28
As highlighted above, access to HIV PrEP through the internet and research trials providing access to PrEP may influence sexual risk behaviours in MSM in London and contribute to syphilis transmission. However, as this was not addressed in the questionnaire, it cannot be described in the context of this surveillance. Future surveillance may benefit from the inclusion of PrEP use in the questionnaire.
This investigation had a number of additional limitations overall. The overall sample size was limited, and opportunistic sampling resulted in a sample biased to the recruiting clinics. Likewise, numbers and characteristics of respondents differed between clinics, which skewed results towards the highest volume clinic participating, and questionnaire method and completeness of data differed between clinics as well. For example, as reported above, HIV status varied significantly by clinic. The highest proportion of HIV-positive respondents (73%) was reported from the clinic reporting the largest number of questionnaires (64/107), therefore having the greatest impact on overall proportion of HIV-positive respondents. However, these clinics are likely to be representative of overall trends, and they comprise a large proportion of syphilis cases in London (just over half of all syphilis cases in London in 2015). 2 As noted, the proportion of respondents surveyed who were HIV-positive (57%) is comparable with the 51% of syphilis HIV coinfection identified in MSM in London in 2015. 2
For one of the participating clinics, information was often incomplete. This was likely due to clinic notes being the source of information and not all items for collection being routinely recorded in these notes. Attempts were made to augment these data gaps by telephoning patients, however with limited success. It is also unknown how many cases attending clinics during the study period declined to participate or were otherwise not included. Responses reflecting a preference for health promotion messaging via an SHC/SHA may reflect response and interviewer bias, as SHAs were interviewing clients and recording questionnaire information, rather than self-reporting from clients.
Syphilis transmission can occur through oral, vaginal, or anal sex. Focusing on condom use for anal and vaginal sex in questionnaires may have misclassified transmission risk from condomless oral sex.
Additionally, the prevalence of suspected risk factors reported should be interpreted with caution, as there was no comparison group to control for biases and quantify risk factors. Many of the issues investigated, for example serosorting, are complex and multidimensional, and also require greater exploration. These issues may be suited to further investigation utilising qualitative methods. Finally, the short period of observation for this surveillance did not allow for identifying emerging or changing trends.
Despite these limitations, this enhanced surveillance has provided insights into likely drivers sustaining the high levels of syphilis transmission observed in MSM in London, to inform health promotion effects and guide further investigations. The insights from this enhanced surveillance may not be generalisable beyond the specific context assessed of MSM visiting clinics in London; however, it is hoped that the data collected will contribute to the developing global evidence base on syphilis in MSM. Syphilis rates have not only been increasing in MSM in London and England, but also in Western Europe and the U.S.1,13,14
The results from this surveillance support continuation of prevention activities focussed on tackling the identified risk factors: condomless sex, serosorting, concurrent sexual partners, high numbers of sexual partners, and chemsex. The results also suggest consideration of further attention to the provision of sexual health promotion advice within SHCs, including: a focus on clinics and other services that serve HIV-positive men; and continuing work to improve rates of partner notification. Both risk factors and preferences for channels to receive health promotion warrant further investigation, to build the global evidence base and further support public health efforts to combat rising syphilis rates in London and globally. Health promotion messaging that emphasises any sex as a risk factor is also important, encouraging frequent screening of all MSM.
Conclusion
There is a need for targeted public health efforts to address the high rates of syphilis in MSM in London. Behavioural risk factors, including lack of condom use, multiple partners and group sex, serosorting, chemsex, and the use of apps to meet sexual partners are important factors in fuelling the rise in syphilis. Despite the popularity of apps for meeting sexual partners, most respondents preferred to receive health promotion information from a SHC advisor.
Footnotes
Acknowledgements
We would like to thank patients and staff at the participating London sexual health clinics for completing the enhanced surveillance questionnaires and contributing to questionnaire design.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.