
Abstract
Human papillomavirus (HPV) infection acquisition is a necessary step in the development of cervical cancer. No study has systematically quantified the rate of newly acquired HPV infections from the published literature and determined its relationship with age. We performed a systematic review and meta-analysis to describe incident HPV infections in women. Medline® and Thomson Reuters Web of Science via PubMed® databases were searched. A total of 46 of 5136 studies met inclusion criteria and contributed results. We conducted a meta-regression analysis of 13 studies, which reported incidence rate estimates on over 13 high-risk HPV types, to provide pooled stratum-specific incidence rates and rate ratios for key population and study characteristics among 8488 women. Studies with mean age < 30 years had relatively higher HPV incidence rates compared to studies with mean age ≥30 years: relative risk = 3.12; 95% CI: 1.41–6.93. HPV-16 was most frequently detected, followed by HPV-18: relative risk = 0.47; 95% CI: 0.33–0.67, and by HPV-58: relative risk = 0.45; 95% CI: 0.27–0.74. Younger age is a key predictor of genital HPV incidence in women. These data on the relative distribution of incident HPV infections will provide a baseline comparison for monitoring of changes in HPV incidence following the implementation of population-level HPV vaccination.
Introduction
Infection with human papillomavirus (HPV) is a necessary cause of cervical cancer,1,2 the fourth most diagnosed cancer in women worldwide. 3 Acquisition of HPV infection is a prerequisite step for development of cervical intraepithelial neoplasia (CIN) and cervical cancer. Two prophylactic vaccines including oncogenic HPV types 16 and 18 were the first to be approved and were shown to successfully reduce persistence of newly acquired incident HPV-16 and -18 infections and associated cervical lesions.4–7 Recently, a nonavalent vaccine has been approved in the United States for the prevention of HPV types 16, 18, 31, 33, 45, 52, 58, 6, and 11. 8
HPV incidence rates have been observed to be higher in women under age 30 years,9,10 with rates of acquisition highest in years closely following sexual debut.10,11 However, other population-based studies have shown that relatively older women also remain at risk for incident HPV infection.9,12–15 While these studies define incident HPV as newly detected infections across the study period, HPV incidence may represent both newly acquired HPV infections as well as recently reactivated latent HPV among women previously exposed.9,15–17 Definitions of HPV incidence across studies vary by HPV laboratory detection methods, testing intervals, HPV status (e.g., type-specificity), HPV categories included (e.g., overall, carcinogenic, individual types), and baseline HPV status.
Systematic reviews of the point-prevalence of HPV infection show that cervical HPV infection in women varies across age and geographic region.18,19 A similar systematic review of global patterns of the incidence of HPV infection would be helpful to obtain a clearer understanding of how studies have estimated HPV incidence. Thus, we performed a systematic review and meta-analysis to describe the magnitude of and variations in HPV incidence among women worldwide, and influence of population and study design characteristics on observed incidence estimates.
Methods
We identified original peer-reviewed journal articles published without language restriction by searching Thomson Reuters Web of Science and Medline® via PubMed® databases through 1 July 2010. We also searched article reference lists from all eligible articles and relevant review articles. Broad search term categories included HPV; human papillomavirus, papilloma virus and incidence; incidence, acquisition, cohort study, newly detected, over time, and natural history (see Supplementary Appendix 1).
Eligible articles were required to present one or more estimates of incident HPV infection, regardless of baseline HPV infection status. Studies testing for cervical HPV infections at more than one-time point using polymerase chain reaction (PCR) or Hybrid Capture (HC; QIAGEN Gaithersburg, Inc.) DNA-based detection methods were included. Serology-based results, male-based results, and studies reporting low-risk HPV (LR-HPV)-only were excluded. Studies reporting baseline cervical abnormalities in excess of 15% were excluded to reflect the characteristics of populations of average risk; however, a study was included if it did not state a baseline prevalence of cervical abnormalities. Articles reporting human immunodeficiency virus (HIV) prevalence in the study population over 5% were excluded, unless stratified by HIV status. If an article did not state the prevalence of HIV in the study population, it was assumed to be less than 5% and was included.
Abstracted incidence data included (i) incidence rate (IR) of HPV infection and the standard error (SE) or confidence interval (CI), (ii) cumulative incidence and SE or CI along with the time interval over which incidence was measured, and (iii) HPV incidence estimates extracted from Kaplan–Meier curves. For studies in which estimated SE for cumulative incidence was not reported, it was calculated as
Number and proportion of HPV incidence estimates were calculated for each category of a given study characteristic. If an article reported multiple results that fell into different categories of study characteristics, the article was included in all relevant categories; consequently, the proportion of study results could add to over 100%. Plots of cumulative incidence and IR were generated for overall (e.g., any tested type), HR, and LR-HPV groups and HPV-types with at least eight results using GraphPad Prism, (GraphPad Software, San Diego, CA).
Some articles that met inclusion criteria were based on the same study populations. To maintain independence of results, we chose the article with the larger number of women in the HPV incidence analysis, or the most recent date of published study results if study sample sizes did not vary. Most articles presented multiple IR estimates of HPV incidence. Therefore, a set of decision rules was applied to select one IR result for inclusion into the meta-regression analysis. Rules to choose a result for each analysis were to select the overall-HPV grouped IR estimate first. If no overall-HPV IR was reported, then the HR-grouped IR estimate was selected.
To formally compare HPV IRs across studies by key study characteristics, meta-regression was used to produce absolute and relative pooled stratum-specific estimates of HPV incidence per 100 women-years. 20 Only studies which employed HPV testing methods that measured at least 13 HPV types were included in meta-regression to ensure data comparability across studies. Random-effects meta-regression was used, with among-study variance estimated by restricted maximum likelihood. 20 Models were adjusted for categories of age (<30/≥30 years), as other characteristics were not statistically significant. Relative measures of effect presented in these models may be interpreted as the ratio of average rates of incident HPV infection between two strata, and are reported as rate ratios (RRs). Pooled stratum-specific estimates allowed descriptive comparisons across individual categories of study characteristics by providing separate estimates and 95% CI for each category. Heterogeneity was assessed by the I2 statistic 21 which is based upon Cochran’s Q. Meta-regression analysis was conducted in STATA version 11 (StataCorp, College Station, TX).
For type-specific HPV analyses, the meta-regression model included all grouped and type-specific IR results, adjusted for categories of age (<30/≥ 30 years) using a random effects model. When a study provided more than one result for HPV incidence, an indicator term was included for each result to control for potential non-independence of results within a given study.
Results
Of 5136 abstracts identified, 46 studies met inclusion criteria. Over half of studies were among women with an average age of 30 years or younger (59%) (Table 1). Study populations consisted of women who attended gynecologic clinics or hospitals (41%), population-based screening programs (24%), college-aged women at university clinics (20%) and women who served as controls in HPV vaccination trials (15%). Nearly half of studies were conducted in North America (46%), with remaining studies conducted in Europe (20%), Central and South America (20%), and other countries (15%). Most studies (87%) reported one or more measures of HPV cumulative incidence, whereas slightly more than half reported IRs (59%).
Characteristics of HPV incidence studies and study results.
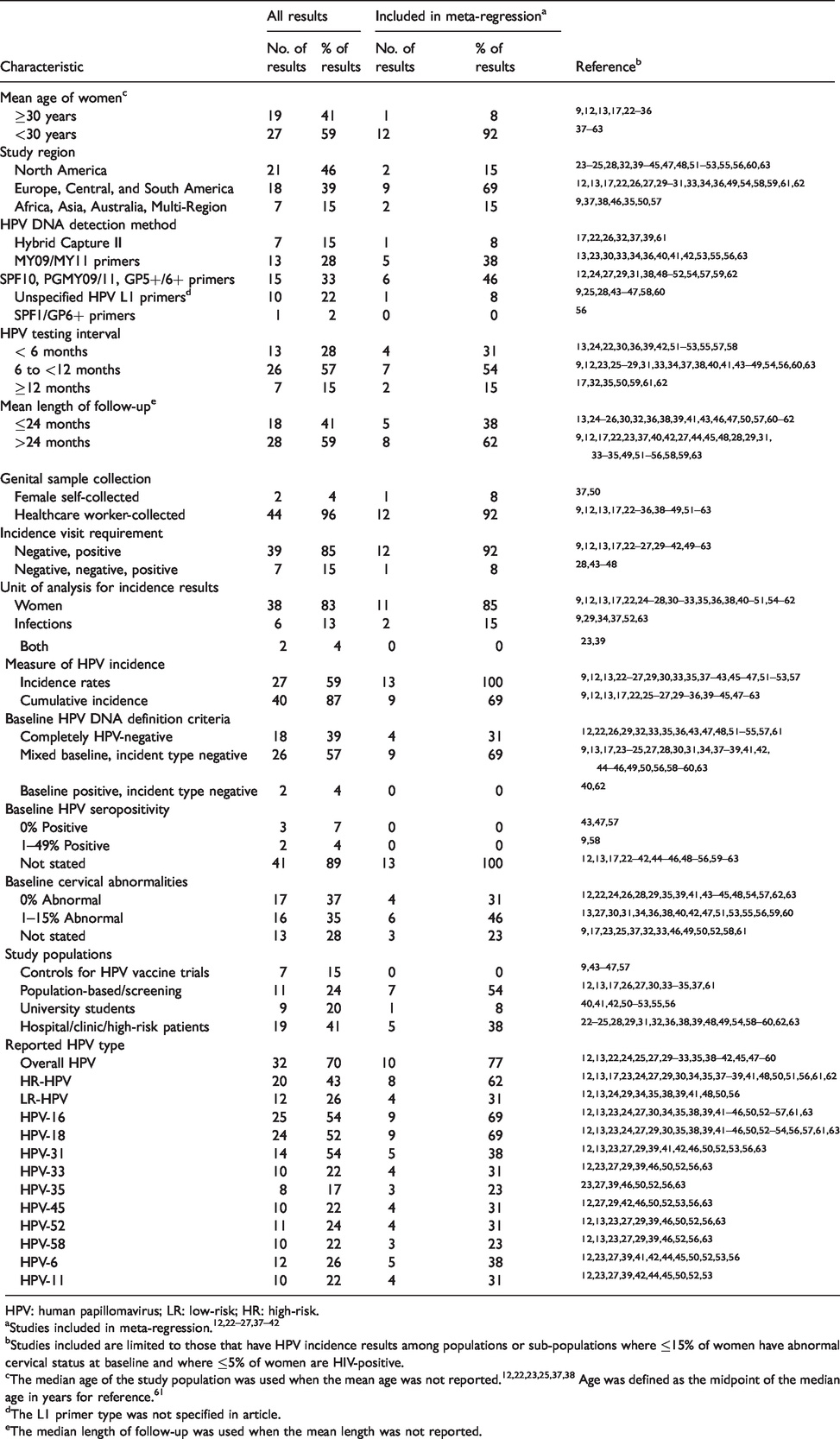
HPV: human papillomavirus; LR: low-risk; HR: high-risk.
bStudies included are limited to those that have HPV incidence results among populations or sub-populations where ≤15% of women have abnormal cervical status at baseline and where ≤5% of women are HIV-positive.
cThe median age of the study population was used when the mean age was not reported.12,22,23,25,37,38 Age was defined as the midpoint of the median age in years for reference. 61
dThe L1 primer type was not specified in article.
eThe median length of follow-up was used when the mean length was not reported.
Most studies defined an incident HPV infection as a single negative HPV test result followed by a single positive HPV result, at any point during study follow-up (85%), while others defined incident infection as two consecutive negative HPV test results followed by a positive result (Table 1). Most studies reported overall HPV incidence (70%) and type-specific results for HPV types −16 (54%) and −18 (52%). Incidence of any HR-HPV type detected was reported in 43% of eligible studies. SPF10, PGMY09/11, and GP5/GP6+ primers were used in 15 studies (33%), while MY09/11 primers were used in 13(28%), and unspecified L1-based primers in 10 studies (22%). HC was used for HR-HPV detection or initial triage of specimens in seven studies (15%). More than half of studies (61%) enrolled populations with some level of HPV DNA positivity, and thus women were at risk for other type-specific incident HPV infections. Remaining studies included women who were completely negative for all HPV tested types at baseline (39%).
Study populations with mean age less than 30 years had higher HPV incidence (range: 1.9–2.9 infections/100 woman-months across studies) than populations with an average age of 30 years and older (range: 0.1–1.4 infections/100 woman-months) (Figure 1). The same pattern was evident for HR-HPV incidence in younger (range: 1.4–1.7 infections/100 woman-months) compared to older populations (range: 0.3–0.9 infections/100 woman-months). Reported incidence for most commonly reported type, HPV-16, was also higher in younger populations (range: 0.4–0.9 infections/100 woman-months) than in older populations (range: 0.0–0.2 infections/100 woman-months). The range of point estimates for HPV-18 appeared to overlap for results from younger (range 0.1–0.5 infections/100 woman-months) and older populations (0.0–0.1 infections/100 woman-months). Among four studies presenting age-stratified incidence,9,13,22,37 rates generally decreased with increasing category of older age (Figure 2). Furthermore, plots of cumulative incidence estimates against study follow-up time (Supplementary Appendix 2), showed a similar age-related pattern of incidence, with younger populations having higher HPV incidence than older participants.
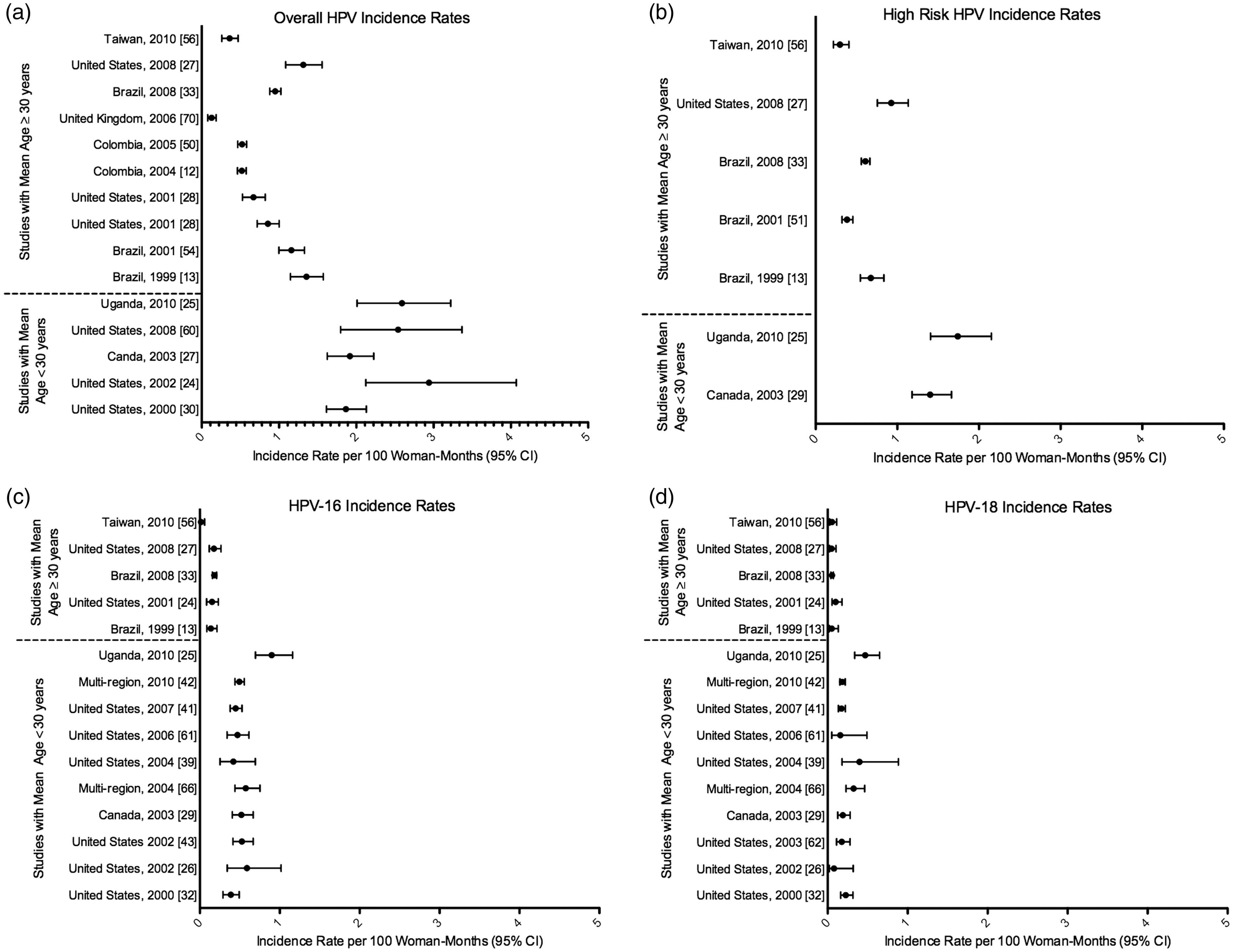
HPV incidence rates, stratified by HPV type.
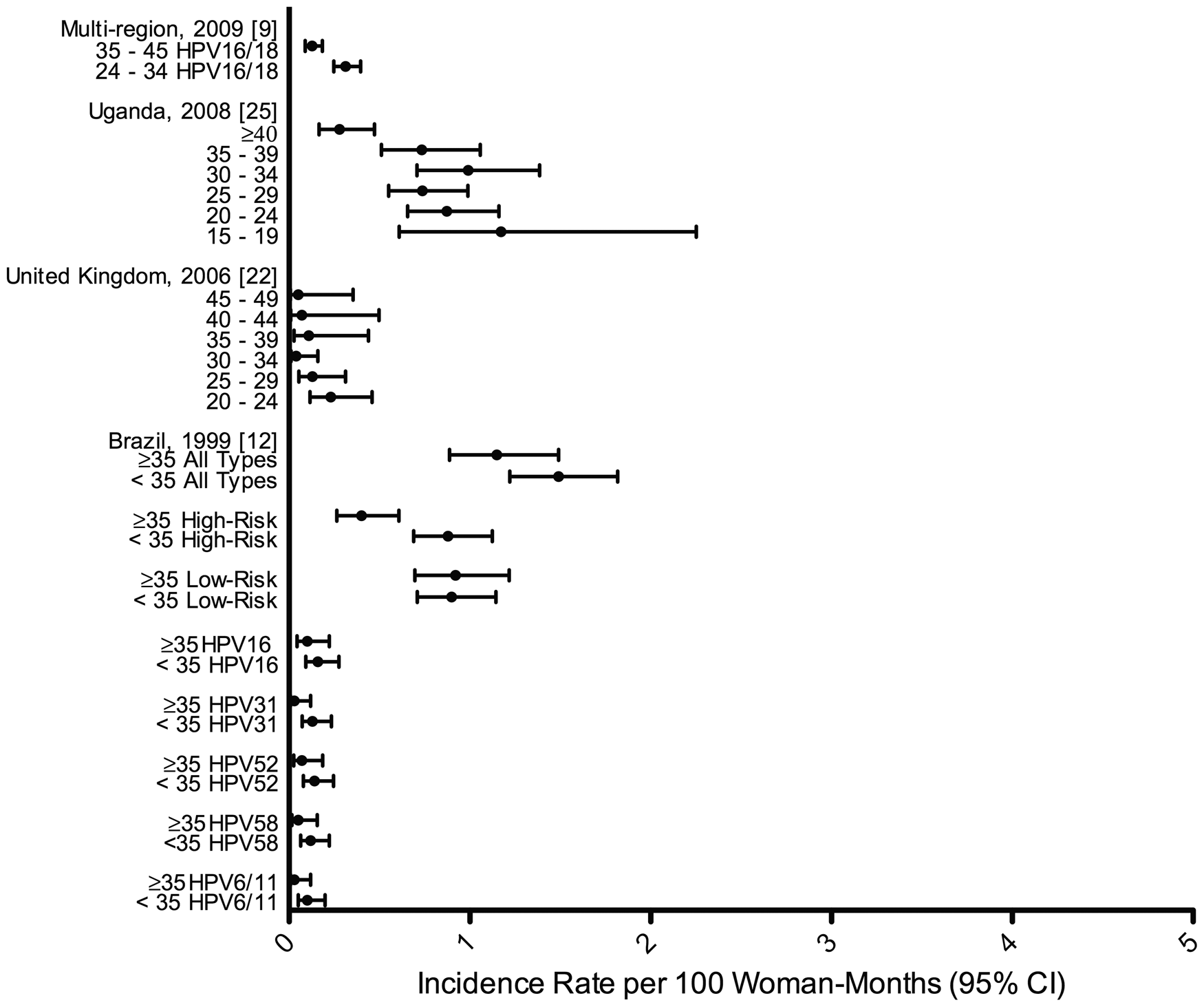
HPV incidence rates, stratified by age in years.
Of 27 studies reporting HPV IRs, 13 studies12,22–27,37–42 met selection criteria for inclusion into meta-regression models that included 8488 women (Table 2). Younger age was associated with higher HPV incidence (p < 0.05): studies with a mean age <30 years had a stratum-specific pooled IR of 1.56 infections/100 woman-months (95% CI: 0.98–2.48) compared to 0.51 (95% CI: 0.37–0.69) infections/100 woman-months in studies with mean age ≥30 years: RR: 3.12 (95% CI: 1.41–6.93). After controlling for age (Table 2), RRs for most study characteristics attenuated after age-adjustment; lower HPV IRs were noted for studies with >24 months follow-up, indicating potential confounding by age. High I2 residual (>90%) in all meta-regression models is indicative of substantial heterogeneity arising from differences between study populations that could not be explained by model terms. 21 Age appeared to be the only factor explaining significant heterogeneity (p value for Cochran’s Q < 0.001) in estimates of HPV incidence.
Meta-regression analysis of independent HPV incidence rates by study characteristics among 13 studies assessing 13 or more HPV types.
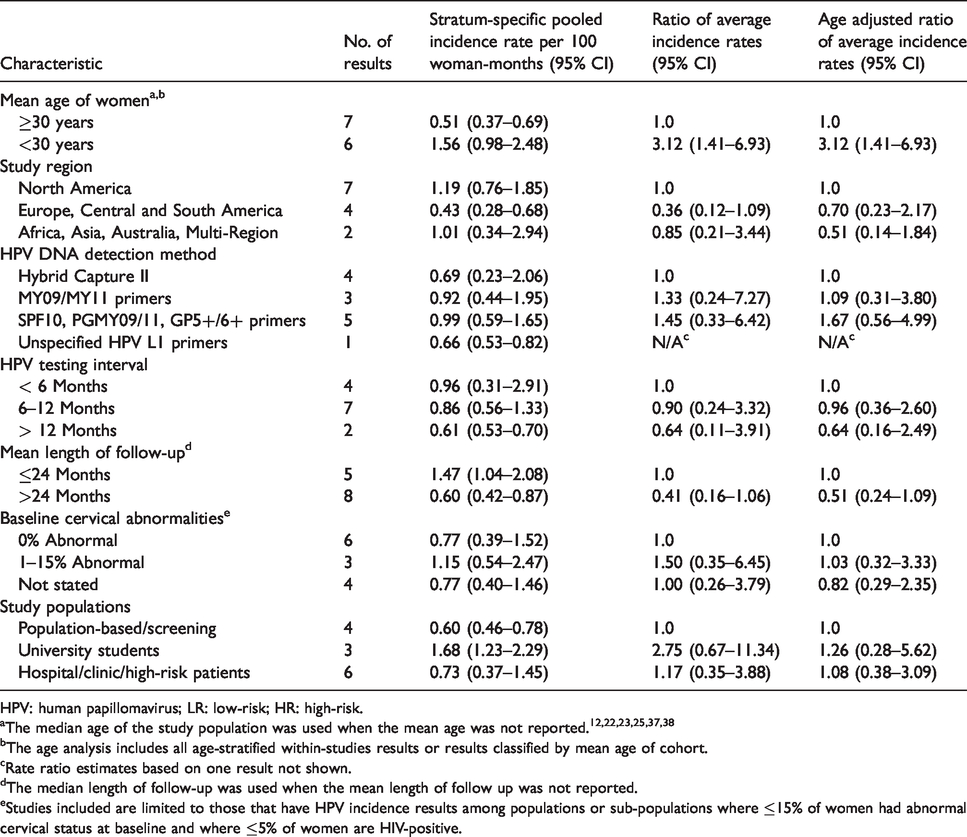
HPV: human papillomavirus; LR: low-risk; HR: high-risk.
aThe median age of the study population was used when the mean age was not reported.12,22,23,25,37,38
bThe age analysis includes all age-stratified within-studies results or results classified by mean age of cohort.
cRate ratio estimates based on one result not shown.
dThe median length of follow-up was used when the mean length of follow up was not reported.
eStudies included are limited to those that have HPV incidence results among populations or sub-populations where ≤15% of women had abnormal cervical status at baseline and where ≤5% of women are HIV-positive.
Analyses of HPV incidence, stratified by HPV type group (Table 3) and genotype (Table 4), included a total of 80 HPV group-based and type-specific results from the 13 studies. The stratum-specific pooled rate of overall HPV infection was 0.63 (95% CI: 0.43–0.92) infections/100 woman-months, and stratum-specific pooled rate of HR-HPV was 0.53 (95% CI: 0.33–0.83) infections/100 woman-months. Incident infection with any LR-HPV type compared with any HR-HPV type was less frequent: RR: 0.59 (95% CI: 0.34–1.00). Highest type-specific HPV IR occurred for type HPV-16 at 0.14 (0.08–0.25) infections/100 woman-months, which is at least twice the rate as infection with the next most common infections: HPV-18 at 0.07 (0.04–0.12), HPV-31 at 0.06 (0.04–0.12) and HPV-52 at 0.06 (0.03–0.12). Age-adjustment resulted in negligible changes to type-specific HPV IR ratios when comparing individual types with HR-grouped types.
Meta-regression analysis of grouped-type HPV incidence among 13 studies assessing 13 or more HPV types.
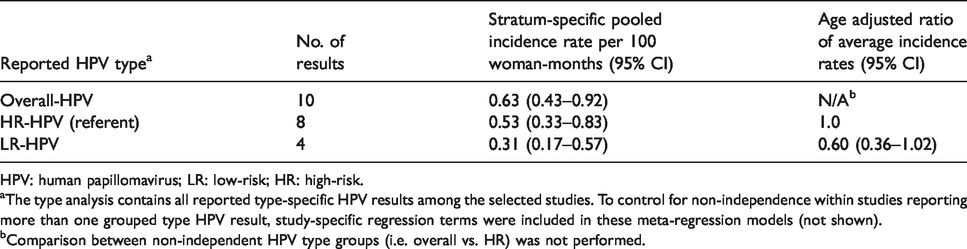
HPV: human papillomavirus; LR: low-risk; HR: high-risk.
aThe type analysis contains all reported type-specific HPV results among the selected studies. To control for non-independence within studies reporting more than one grouped type HPV result, study-specific regression terms were included in these meta-regression models (not shown).
bComparison between non-independent HPV type groups (i.e. overall vs. HR) was not performed.
Meta-regression analysis of type-specific HPV incidence among 13 studies assessing 13 or more HPV types.
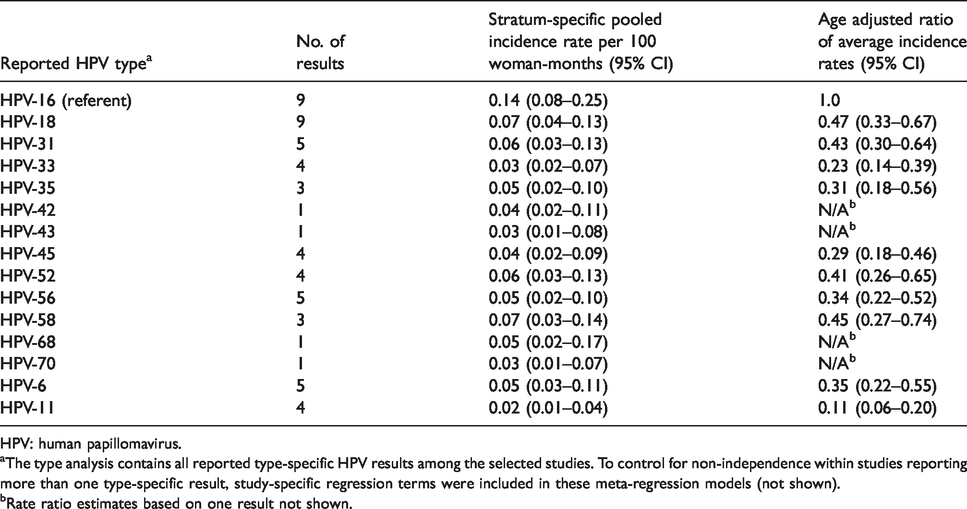
HPV: human papillomavirus.
aThe type analysis contains all reported type-specific HPV results among the selected studies. To control for non-independence within studies reporting more than one type-specific result, study-specific regression terms were included in these meta-regression models (not shown).
bRate ratio estimates based on one result not shown.
Discussion
To our knowledge this review, of 43,598 women, is the first systematic review of the incidence of cervical HPV infection worldwide. Age was the main predictor of HPV incidence, with younger populations (<30 years) having over three times HPV incidence rates than relatively older populations. Nevertheless, newly detected HPV infections in women 30 years and older were non-negligible with a stratum-specific pooled HPV IR of 0.56 infections/100 woman-months. The rate of HR-HPV infection was 1.7 times that of LR-HPV, while HPV-16 had at least twice that of any other individual high-risk HPV type (e.g., HPV-18, HPV-31).
This systematic review of incident HPV infections builds upon previous reviews describing worldwide HPV point prevalence, stratified by age.18,19 HPV point prevalence has peak at varying ages for different geographic regions, with Central and South America and Africa showing higher HPV point prevalence among women aged 45 and older than relatively younger women.18,19 One large incidence-based study in Colombia noted similar age-related patterns of incidence, with peak overall and HR-HPV incidence between ages of 15 and 20 and a minor increase in HPV incidence around age 50, before declining again at relatively older ages. 12 Findings in our meta-analysis show a consistently higher risk of HPV acquisition among relatively younger-aged women. However, limited data were available on age-stratified HPV incidence with sufficiently large sample sizes, limiting our ability to thoroughly explore relationships between HPV incidence and age groupings. Our age-based dichotomization of studies at mean/median population age of 30 years was a relatively crude method for classifying a study population's age distribution in the meta-regression analysis that may have masked subtle differences in HPV incidence within relatively broad age categories. We found significant heterogeneity (p values for Cochran’s Q < 0.001) in estimates of HPV incidence that could partially be explained by age. This is consistent with systematic reviews of HPV prevalence, which noted heterogeneous estimates of HPV prevalence across global studies and a clear influence of age.18,19
Since this review was conducted, there have been a number of studies that have reported on HPV incidence, including large studies from China, 64 India, 65 the Netherlands, 66 and smaller studies from Finland 67 and Tanzania. 68 Reported incidence of type-specific HPV infections observed in these studies is comparable to published results from this review; with high rates of HPV-16 infection compared to other tested HPV types.
Current models of the natural history indicate that HPV infection is generally acquired shortly after sexual debut. A proportion of these HPV infections persist, increasing risk high-grade precancerous cervical lesions that either regress or develop into cancer. 16 While newly detected HPV infections seem to decline with age, those in older women may result from both newly acquired HPV infection or reactivation of previously acquired infections. 17 A more recent study of 35- to 60-year-old US women found that most newly detected HPV infections occurred in sexually active women who self-reported no new sexual partners or during periods of abstinence. 15 Together, these data imply that HPV viral latency and subsequent reactivation may represent an important source of “incident” HPV infections in older women. 16 We were unable to examine the role of individual or population-level measures of sexual behavior in younger and older women in our analysis to examine these potentially mediating risk factors.
Major strengths of this investigation are the notably large sample size, based on inclusion of a broad range of original peer-reviewed journal articles dating back to 1995. Further, publications were systematically identified after careful review using an a priori inclusion and exclusion criteria. Two independent readers entered study results to ensure accuracy of transcription. Our use of random effects meta-regression is unique and allowed for weighting of relative contributions of multiple studies while accounting for between-study and within-study variability.
Limitations of this study include a relatively small number of articles (n = 13) reporting HPV IRs with 13 types or more limited precision of our meta-regression analysis. For articles that only reported cumulative HPV incidence, we were unable to convert cumulative HPV incidence results into HPV IRs using formulaic conversion (i.e., based on the exponential distribution). This is because a sensitivity analysis among the small subset of studies reporting both cumulative and rate-based incidence measures showed that HPV IRs were not constant across study follow up. Additionally, we had limited covariate data on other factors that influence observed differences in HPV incidence (e.g. type-specific seropositivity, sexual partnerships, smoking status).
Understanding differences in HPV detection methods and definitions is crucial to describing HPV incidence. Most studies defined type-specific incident HPV infection as a subsequent positive test result following a negative result for that HPV type. To limit large differences in the sensitivities of detection assays, we restricted our review to PCR and HC-II detection methods. While HPV DNA detection methods are highly sensitive, the possibility of a sample containing HPV below the detection limit may have resulted in misclassification of HPV incidence. Seven studies defined type-specific infection as a subsequent positive test result following two consecutive negative results28,43–48; their inclusion may have led to a potential underestimation of HPV incidence. Alternatively, a single detection of HPV DNA may indicate only recent exposure to HPV without establishment of a true infection, leading to a potential overestimation of incidence of HPV infection.
Current U.S. Advisory Committee on Immunization Practices guidelines recommend universal vaccination for girls aged 11–12 years before the onset of sexual intercourse given relatively high rates of HPV acquisition following sexual debut and the high vaccine efficacy in HPV-naïve vaccine recipients.69–71 A study of the quadrivalent HPV vaccine in women aged 24–45 years observed high efficacy against HPV infections appearing after the seventh month of follow-up. 72 However, this study did not provide specific estimates of vaccine efficacy for individual HPV types in this 24–45 age group, and also found that prophylactic HPV vaccination was less effective among women with pre-existing infection at enrollment. The question remains as to what extent vaccination should be recommended in women ≥26 years. Our results indicate that while women ≥30 years are less likely to have newly detected infections, HPV-16/18 accounts for many of these infections.
Acquisition of cervical HPV infection presents a risk to women’s health as a necessary cause of high-grade lesions and cervical cancer. Worldwide, women ≤30 years present with a higher rate of incident HR-HPV infections, yet older women also remain at risk of incident infection. Though we present no single estimate of HPV incidence, the summary data presented here highlight the distribution of incident HPV infection prior to the global introduction of prophylactic HPV vaccines, and will be useful for the monitoring of changes in HPV incidence after implementation of population-level HPV vaccination.
Supplemental Material
STD824441 Supplemental Material1 - Supplemental material for Patterns of incident genital human papillomavirus infection in women: A literature review and meta-analysis
Supplemental material, STD824441 Supplemental Material1 for Patterns of incident genital human papillomavirus infection in women: A literature review and meta-analysis by Bradford S Wheeler, Anne F Rositch, Charles Poole, Sylvia M Taylor and Jennifer S Smith in International Journal of STD & AIDS
Supplemental Material
STD824441 Supplemental Material2 - Supplemental material for Patterns of incident genital human papillomavirus infection in women: A literature review and meta-analysis
Supplemental material, STD824441 Supplemental Material2 for Patterns of incident genital human papillomavirus infection in women: A literature review and meta-analysis by Bradford S Wheeler, Anne F Rositch, Charles Poole, Sylvia M Taylor and Jennifer S Smith in International Journal of STD & AIDS
Supplemental Material
STD824441 Supplemental Material3 - Supplemental material for Patterns of incident genital human papillomavirus infection in women: A literature review and meta-analysis
Supplemental material, STD824441 Supplemental Material3 for Patterns of incident genital human papillomavirus infection in women: A literature review and meta-analysis by Bradford S Wheeler, Anne F Rositch, Charles Poole, Sylvia M Taylor and Jennifer S Smith in International Journal of STD & AIDS
Supplemental Material
STD824441 Supplemental Material4 - Supplemental material for Patterns of incident genital human papillomavirus infection in women: A literature review and meta-analysis
Supplemental material, STD824441 Supplemental Material4 for Patterns of incident genital human papillomavirus infection in women: A literature review and meta-analysis by Bradford S Wheeler, Anne F Rositch, Charles Poole, Sylvia M Taylor and Jennifer S Smith in International Journal of STD & AIDS
Supplemental Material
STD824441 Supplemental Material5 - Supplemental material for Patterns of incident genital human papillomavirus infection in women: A literature review and meta-analysis
Supplemental material, STD824441 Supplemental Material5 for Patterns of incident genital human papillomavirus infection in women: A literature review and meta-analysis by Bradford S Wheeler, Anne F Rositch, Charles Poole, Sylvia M Taylor and Jennifer S Smith in International Journal of STD & AIDS
Footnotes
Authors’ contributions
BSW collected data, performed analyses, and prepared the manuscript. AFR reviewed data collection, provided analytic support and assisted with manuscript preparation. CP provided methodological support. SMT provided manuscript feedback. JSS directed the research process and provided manuscript feedback. All authors revised the manuscript, approved of the final version, and agreed to be accountable for all questions regarding the accuracy and integrity of the manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sylvia Taylor is an employee of the GlaxoSmithKline group of companies and holds shares as part of her employee remuneration. Jennifer Smith has received unrestricted research grants or served on paid advisory boards for BD, GlaxoSmithKline, Hologic, Merck, and Trovagene over the past five years.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by GlaxoSmithKline Biologicals SA, Wavre, Belgium.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.