
Abstract
Organ transplantation among people living with human immunodeficiency virus (PLHIV) is increasing. Guidelines recommend any changes in antiretroviral therapy (ART) prior to transplantation, but there are limited data regarding ART changes post transplantation. We report a case where an ART switch from a protease inhibitor-based regimen to dolutegravir plus emtricitabine/tenofovir alafenamide in a renal transplant recipient led to subtherapeutic tacrolimus concentrations and an increased serum creatinine (SCr). A workup for graft rejection was performed (including kidney biopsy and cytomegalovirus and BK virus polymerase chain reaction) following the rise in SCr, which was higher than expected from dolutegravir initiation (via organ cation transporter 2 inhibition). This case highlights the potential challenges of switching ART regimens in PLHIV post transplantation.
Background
With the improved life expectancy among people living with human immunodeficiency virus (PLHIV), organ transplantation among candidates within this population has increased.1–4 The HIV Organ Policy Equity Act, which permits the use of organs from PLHIV in transplant candidates with HIV, has expanded the pool of potential donors. 5 Management of drug interactions between antiretroviral therapy (ART) and immunosuppressive agents presents a major challenge. Although clinicians have gained experience navigating these complex interactions, there is a paucity of data regarding ART changes during the post-transplantation period.4,6,7 We report a case where an ART switch in a renal transplant recipient led to subtherapeutic tacrolimus concentrations and an increased serum creatinine (SCr).
Case description
A 51-year-old Black male was diagnosed with HIV and end-stage renal disease (ESRD) upon hospitalization for fatigue/weakness (December 2006). ESRD risk factors included HIV associated-nephropathy, hypertensive nephrosclerosis, race, and former injection drug use. After 9 years, the patient underwent a successful post-deceased-donor kidney transplantation (September 2015). Sixteen months post transplantation (January 2017), his HIV provider decided to replace his ritonavir-boosted atazanavir, abacavir, and lamivudine with emtricitabine/tenofovir alafenamide and dolutegravir (note: Pan-susceptible genotype in 2007). Comorbidities included hypertension, benign prostatic hyperplasia, and hypertriglyceridemia, for which he was receiving metoprolol, terazosin, and gemfibrozil. The immunosuppressant regimen consisted of mycophenolate, prednisone, and tacrolimus (goal range 4–8 ng/mL). The viral load remained controlled throughout the post-transplant period, with recent pertinent labs as follows: HIV RNA <20 copies/mL, CD4 count 90 cells/mm3, SCr 1.59 mg/dL, estimated glomerular filtration rate 53 mL/min/1.73 m2, triglycerides 117 mg/dL, and tacrolimus 4.9 ng/dL. Over the past year, the SCr interquartile range (IQR) was 1.31–1.60 mg/dL. Trimethoprim/sulfamethoxazole was prescribed for Pneumocystis jirovecii pneumonia and Toxoplasma gondii prophylaxis.
In anticipation of a tacrolimus exposure reduction after discontinuation of ritonavir-boosted atazanavir, the ART change was communicated to the transplant team. A plan was created to modify the tacrolimus dose based on therapeutic drug monitoring. Initially, the dose was increased from 0.5 mg weekly to 0.5 mg twice daily (Figure 1). Over the next 10 days, several levels were sent and two additional dose adjustments were required to achieve the target trough. Overall, a 70-fold dose increase was required. The SCr levels rose unexpectedly over the next two months. After a SCr result of 2.28 mg/dL on day 70 post-ART switch, a comprehensive workup was performed to rule out graft rejection. A kidney biopsy revealed minimal inflammation, moderate interstitial fibrosis, and tubular atrophy. Immunofluorescence stain did not show the presence of C4d antibodies. This pathology was not consistent with rejection. Cytomegalovirus and BK virus polymerase chain reaction were performed and found no DNA. SCr levels stabilized over 12 months post-ART switch, with a mean of 2.24 mg/dL (2.07–2.4 mg/dL IQR).
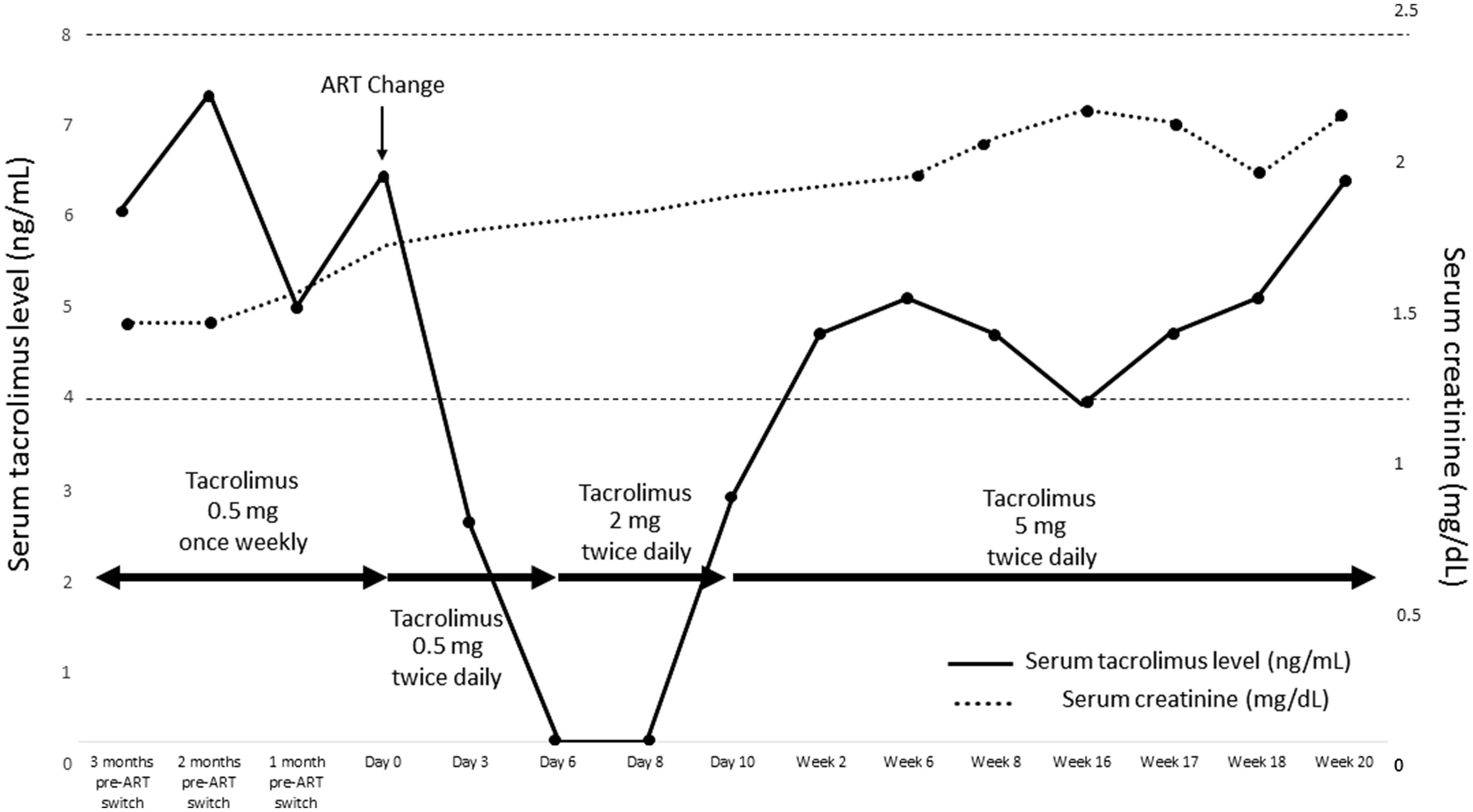
Timeline: Serum tacrolimus level and creatinine pre- and post-antiretroviral therapy change. ART: antiretroviral therapy.
Discussion
Our case describes the complexities that can present when switching ART in a PLHIV post transplantation. Most transplant and infectious disease (ID) specialists are aware of the effect potent inhibitors of cytochrome P450 enzymes and/or drug transporters (e.g. P-glycoprotein), such as ritonavir and cobicistat, can have on the concentrations of coadministered drugs. The consequences of these interactions are especially dire when agents have a narrow therapeutic index.4,6,7 Despite this awareness and close monitoring of patients during any therapeutic changes, accurately predicting the optimal dose adjustments and minimizing collateral damage can still present challenges to even the most experienced clinicians. In organ transplant recipients, tacrolimus dose reductions of up to 120-fold have been required in patients initiated on ritonavir.8–11 Removal of this agent, even through a calculated ART switch, can expectantly also lead to a dramatic change in drug exposures of concomitant medications. In retrospect, the initial titration in our patient could have started higher than 0.5 mg twice daily (14-fold higher than previous dose). However, the transplant team was concerned about overshooting the tacrolimus levels and subsequent risk of nephrotoxicity. We utilized the Drug Interaction Probability Scale (DIPS) to determine if a causal relationship between the removal of a ritonavir-based regimen and subtherapeutic tacrolimus levels was present. The likelihood of this relationship resulting in a drug interaction was probable (DIPS score 5–8). 12
Higher rates of graft rejection have been described among transplant recipients with HIV disease. Poor graft and overall survival in PLHIV may be attributed to the challenges of achieving therapeutic immunosuppressant concentrations due to drug interactions with ART. In particular, protease inhibitor (PI)-containing regimens have been associated with an increased incidence of graft loss and other adverse outcomes in comparison to PI-sparing regimens.13–16 Our patient’s ART regimen was changed in great part due to this concern. Current guidelines recommend that PLHIV who are transplant candidates be switched to regimens that yield minimal effects on the pharmacokinetics of coadministered drugs, such as integrase strand transfer inhibitor (INSTI)-based regimens.4,7,17 Despite switching to a theoretically safer regimen, renal function appeared to decline over the following few months (based on SCr changes). Although our patient’s renal function stabilized, the increased SCr post-switch required more intensive monitoring, additional laboratory testing, and a kidney biopsy. Dolutegravir could have played a role in this SCr elevation, as it inhibits creatinine secretion by organic cation transporter 2 (OCT2). In clinical trials, SCr elevations from dolutegravir were modest (0.1–0.17 mg/dl).18–25 However, a 0.4 mg/dL SCr increase was noted in another renal transplant recipient after a switch from protease inhibitor-based therapy to dolutegravir-based therapy. 26 This interaction would still fail to explain the 0.79 mg/dL increase in our patient, particularly since he was already on another OCT2 inhibitor (trimethoprim). 27 Other drugs were deemed unlikely causes. Interstitial nephritis from sulfamethoxazole would have been identified upon biopsy and renal injury would have progressed. 28 Gemfibrozil has primarily been implicated in renal insufficiency among patients with a baseline SCr > 2 mg/dL. 29 Although the phase III renal safety data with tenofovir alafenamide are encouraging, there is a paucity of these data in the setting of renal transplantation.30–33 Ultimately, the cause of the SCr elevation could not be fully determined. Although the kidney biopsy is the gold standard for the diagnosis of acute antibody-mediated rejection, it inherently samples only one part of the kidney and may lead to a false-negative.34,35 Thus, the negative findings of our patient’s biopsy could have missed pathology in another section. Ideally, additional testing and imaging (i.e. urinalysis, ultrasound) could have been performed to identify other possibly etiologies or rule out the ART switch as the definitive cause. Although the SCr changes experienced by our patient would not be alarming under normal circumstances, the gravity of such changes in this population deems it extremely important that more literature and guidance become available.
Current guidelines recommend switching ART prior to transplantation, however provide no recommendations on how to approach and monitor changes post transplantation. 4 Nonetheless, specialists are often forced to make ART changes post transplantation due to a variety of reasons: to address long-term (or late-onset) toxicities, to avoid drug–drug interactions when a new medication becomes indicated for a comorbidity, and/or if resistance develops. Treatment simplification and switch strategies under less straightforward settings (i.e. to improve quality of life, limit risks for long-term toxicities) have now become standard practice in PLHIV. As the consequences of suboptimal outcomes after any therapeutic changes are significantly higher in transplant recipients living with HIV, a heightened awareness of interactions both upon initiation and discontinuation of these agents remains critical. 36 Despite INSTI-based regimens being the preferred ART in this population, the effect dolutegravir (and the new antiretroviral bictegravir) has on creatinine elimination through the inhibition of SCr tubular secretion should also be considered when first introduced to any regimen. Finally, it remains imperative that a patient’s care be well communicated and coordinated between the ID and transplant teams in this ever-growing population.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.