
Abstract
The CD4/CD8 ratio is an indirect marker of immune activation, immune senescence, and inflammation in HIV infection. We performed a prospective study of the CD4/CD8 ratio evolution in 245 virally-suppressed (median, 55 months) HIV-infected patients (29% females) who had switched to four dual antiretroviral regimens. At baseline, the median CD4/CD8 ratio was 0.71 (interquartile range, IQR, 0.46–0.97), associated with duration of HIV infection, nadir CD4+ cell count, and AIDS diagnosis. It was lower in the case of hepatitis C virus coinfection and cardiovascular disease (p = 0.09), but the ratio was higher in patients with chronic kidney disease, proteinuria, or osteoporosis. At 48 weeks, the median CD4/CD8 ratio increased by 3% (+0.02; IQR, –0.07, +0.09; p = 0.07); greater improvement was observed in patients with lower baseline ratios and previous AIDS diagnosis. The slope of increase was slower in patients with the highest baseline values. Also, there were no differences in the CD4/CD8 ratio increase according to type of dual regimen, after adjusting for baseline and HIV-related values. In conclusion, CD4/CD8 ratio increase is observed during suppressive dual regimens, and its extent is related to baseline values and previous HIV-related factors. Longer duration on antiretroviral therapy and drug toxicity could affect the evolution of this marker in the presence of comorbidities.
Keywords
Introduction
Dual therapies are being evaluated as alternative treatments in a population of HIV-1-infected patients with increasing age and comorbidities. 1 Although several studies suggest adequate efficacy with fewer adverse events, concern exists about the possibility of a lower antiviral action than triple therapy, resulting in higher residual viremia, systemic inflammatory activity, and immune activation. 2
The CD4/CD8 ratio has become an indirect marker of persistent immune activation, immune senescence, and inflammation, suggesting that the measurement of this ratio might serve as an adequate surrogate for the HIV reservoir. 3 Lower values have been associated with a higher risk of different non-AIDS-associated events and mortality. 4 However, there are no data about the evolution of this marker when using dual regimens.
Thus, we collected prospective data about the CD4/CD8 ratio evolution and the relationship with comorbidities of those patients switching from triple to different dual therapies, due to toxicity or simplification.
Methods
Participants in this study were sampled from two cohorts in our Unit: ComorVIH, a cohort of around 300 HIV-1-infected patients being observed for renal and bone toxicity and its evolution after the change of antiretroviral therapy (NCT 02116751); and the Dolbi cohort study, evaluating those patients switching to a dual regimen including dolutegravir (DTG) (NCT02491242). For this study, we selected those patients virologically suppressed for at least 12 months that switched to a dual regimen, due to toxicity, drug interactions, or simplification. Patients with previous use of mono or dual therapies, or with a detectable HIV viral load (blips or virologic failure) at the time of change or in the last six months before inclusion, were excluded. No cases of pregnancy or chronic hepatitis B virus were included. The study was approved by our IRB (EC 139/18).
Laboratory studies, including CD4+ and CD8+ by flow cytometry (Becton-Dickinson Diagnostics, San Jose, California, USA), and HIV RNA level (Versant HIV-1 RNA 1.0 [kPCR], Siemens Diagnostics, Erlangen, Germany; quantification limit 37 copies/mL), serum creatinine, transaminases, and lipid parameters were performed for the study at inclusion and then every three to four months. The glomerular filtration rate (eGFR) was estimated by using the CKD-EPI equation, and a urinary analysis including determinations of protein–creatinine ratio (uPCR) was determined. Also, a bone DXA (Dual X-ray absorptiometry) scan was performed at baseline (Hologic 4500, Bedford, USA).
Different active or recent comorbidities were collected at inclusion. Hepatitis C virus (HCV) coinfection was considered if the patient had a positive serology and positive HCV RNA PCR or a history of untreated infection. Cardiovascular disease (CVD) was a composite variable defined as a previous diagnosis of ischemic heart disease, non-fatal stroke, acute myocardial infarction, or peripheral artery disease. A previous diagnosis of cancer was obtained from the patient history, considering those diagnoses in the last year. Proteinuria was defined as an uPCR ≥150 mg/g creatinine. Chronic kidney disease (CKD) was established if the eGFR value was lower than 60 mL/min/1.73 m2 in two determinations separated by three months (CKD stage 3 or higher) according to the National Kidney Foundation guidelines for CKD. Osteoporosis was defined as a T-score ≤−2.5 SD at the lumbar spine and/or femoral neck, according to World Health Organization criteria.
The primary predictor of interest was the difference in the CD4/CD8 ratio after the first 12 months of dual therapy. The secondary end-points were the differences in the ratio according to the different dual therapies, and the outcome in relation to different comorbidities (HCV coinfection, CVD, cancer, CKD, proteinuria, osteoporosis at the hip and at the spine). A CD4/CD8 ratio ≤0.3 was used as cutoff value of increased risk for the emergence of comorbidities, as found in other studies.4,5
Characteristics of patients according to baseline CD4/CD8 ratio were compared for statistical significance using the Mann–Whitney U-test for continuous variables and the Chi square test for categorical variables. At 48 weeks, differences with respect to baseline were compared by the Wilcoxon rank test for paired samples. Correlations between quantitative factors and ratio were assessed using the Spearman correlation coefficient. To evaluate the association of dual therapies with baseline ratio and subsequent CD4/CD8 slope, we used a linear mixed-effects regression model, including age, nadir CD4+ cell count, time of HIV infection, time on antiretroviral therapy, and previous AIDS diagnosis as fixed covariates. A two-tailed p value <0.05 was considered statistically significant.
Results
From 2015 to 2017, 245 ART-suppressed patients (29% females, 100% white ethnicity) met inclusion criteria and were enrolled in this study. These patients switched to the combination of DTG plus rilpivirine (RPV; 96 patients; 39%); lamivudine (3TC) plus boosted darunavir (bDRV; 81 patients, 33%); bDRV+DTG (53 patients, 22%), or bDRV+RPV (15 patients, 6%). Characteristics of the patients, overall and according to dual therapy received, are shown in Table 1.
Baseline characteristics of the 245 patients receiving a dual regimen, and according to the different dual therapy combinations.
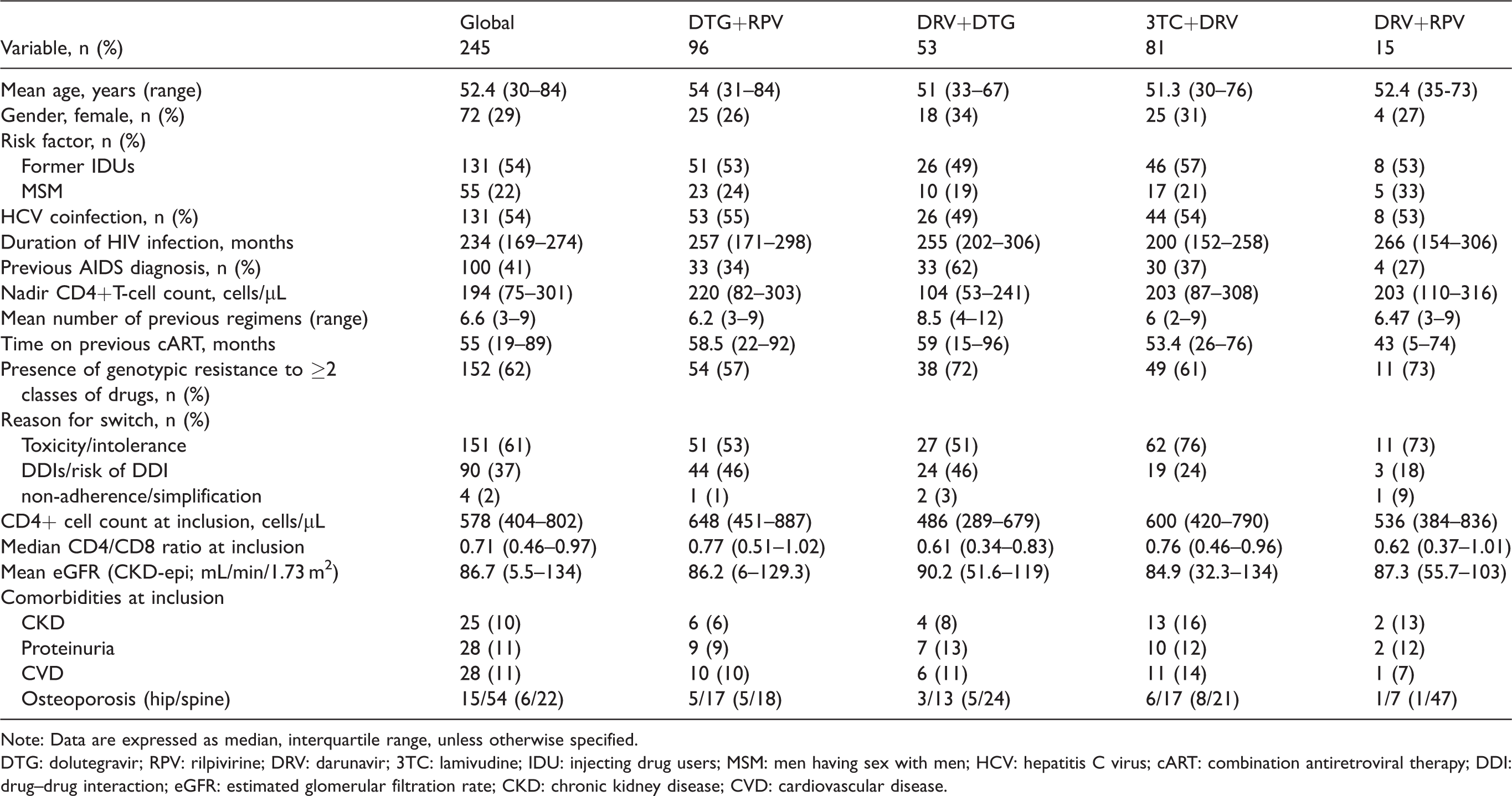
Note: Data are expressed as median, interquartile range, unless otherwise specified.
DTG: dolutegravir; RPV: rilpivirine; DRV: darunavir; 3TC: lamivudine; IDU: injecting drug users; MSM: men having sex with men; HCV: hepatitis C virus; cART: combination antiretroviral therapy; DDI: drug–drug interaction; eGFR: estimated glomerular filtration rate; CKD: chronic kidney disease; CVD: cardiovascular disease.
Globally, the mean age was 52 years, median nadir CD4 cell count was 194 cells/μL, and 41% had a prior AIDS diagnosis. At baseline, the median CD4 cell count for all the subjects was 578 cells/μL, and the median CD4/CD8 ratio was 0.71 (interquartile range, IQR, 0.46–0.97), with 10% of patients ≤0.3. This baseline ratio was inversely correlated with the duration of HIV infection (rho= –0.14, p = 0.039), and directly correlated with the nadir CD4+ cell count (rho= 0.23; p < 0.01). Of note, patients a with previous AIDS diagnosis had a significantly lower ratio (0.55 vs. 0.78; p < 0.001).
At inclusion, the CD4/CD8 ratio was lower in the case of HCV coinfection (0.65 vs 0.83, <0.01), with a trend for CVD (0.62 vs. 0.72; p = 0.09). Although not significant, the median ratio was lower for osteoporosis at the hip (0.55 vs. 0.77; p = 0.98) and cancer (0.63 vs. 0.71; p = 0.9), but it was equal or greater in patients with CKD (0.86 vs. 0.70; p = 0.28), proteinuria (0.77 vs. 0.73; p = 0.61), or osteoporosis at the spine (0.85 vs. 0.77; p = 0.56).
As shown in Table 1, dual regimens showed a different baseline median ratio, higher in the case of DTG+RPV (0.77) and 3TC+bDRV (0.76), and lower in patients switching to bDRV+DTG (0.61), which could be explained by the different baseline characteristics of the patients, with fewer previous failures, and less previous AIDS diagnosis in the case of the highest values.
There was a significant correlation between the increase in the CD4/CD8 ratio and the time on dual therapy (rho= 0.24; p < 0.01; Figure 1). At 48 weeks, all patients but four (1.6%) had virologic suppression; the CD4+ cell count increased from 578 to 645 cells/µL (median difference, +62; IQR −66, +129; p = 0.03; from 29% to 29.8%), the CD8 decreased significantly (from 40.9% to 39.2%, p = 0.01), and the CD4/CD8 ratio rose to 0.76 (IQR, 0.5–1.02). The median of the difference was +0.02 (IQR, −0.07, +0.09; p = 0.07), representing a 3% increment relative to baseline value, and reducing the number of patients with a ratio ≤0.3 to 6%. The number of patients reaching the 0.8 threshold value increased from 41% to 45%. This increase was directly proportional to the increase in CD4 cell count (rho= 0.2; p < 0.01), and inversely related to age (rho = −0.15, p = 0.04), and to the ratio at baseline (rho = −0.25, p < 0.01). Indeed, the increase was non-linear and was higher in patients with a lower baseline CD4/CD8 ratio (–0.017 vs. +0.07; p < 0.01 for patients above/below 0.8; Figure 2).
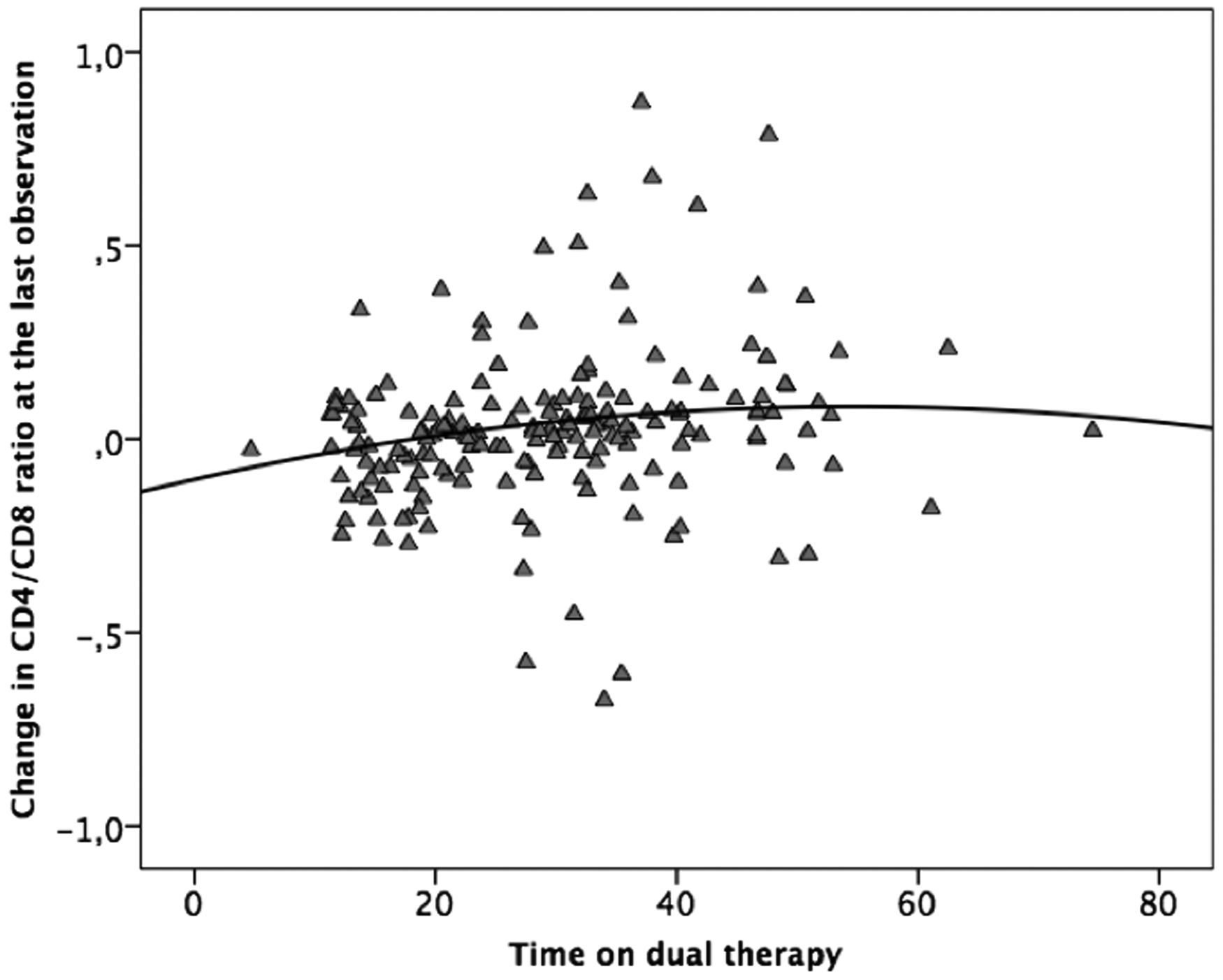
Correlation between time on dual therapy and CD4/CD8 ratio change.
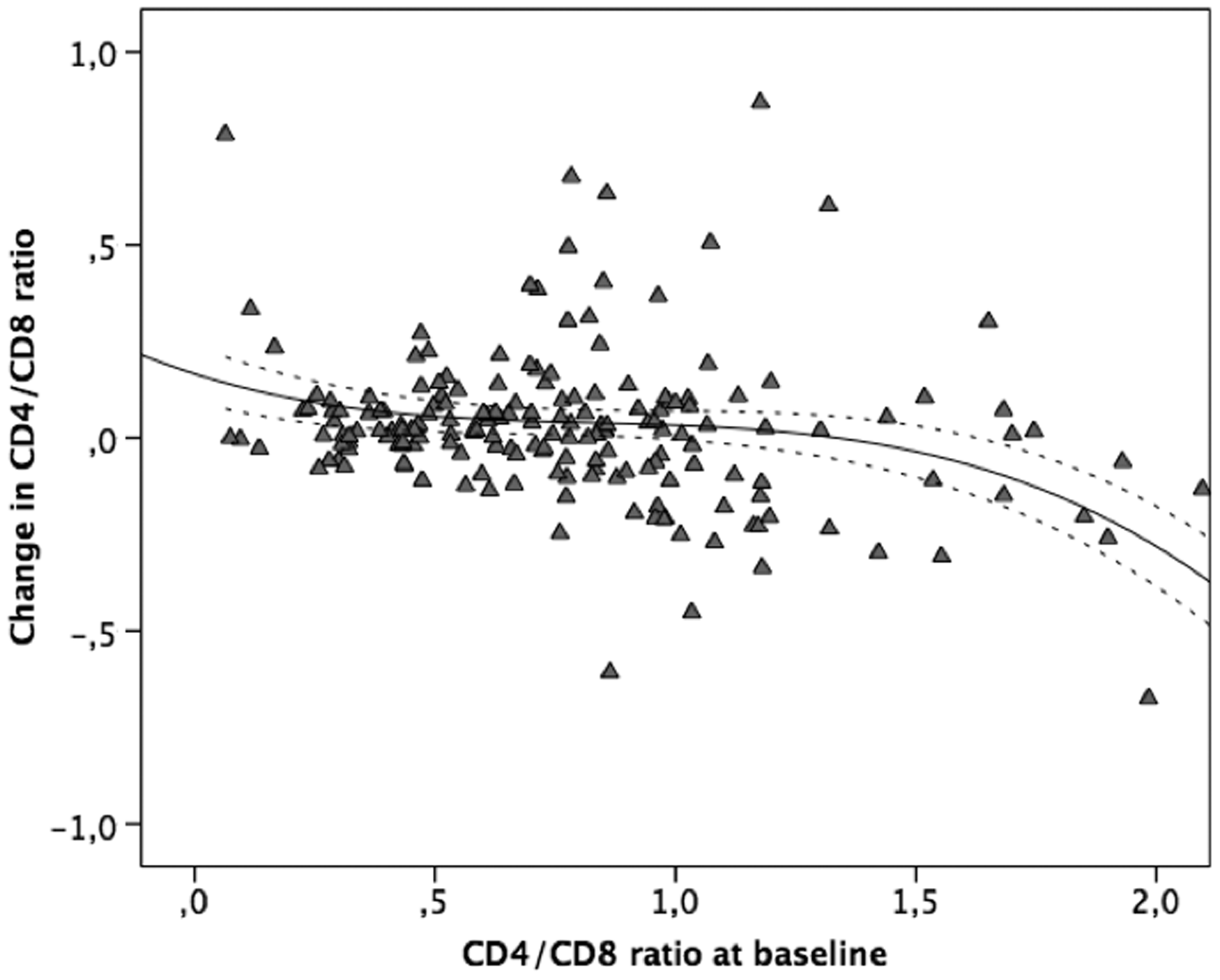
Changes in CD4/CD8 ratio according to values at inclusion.
There was an improvement in all the different dual regimens (Figure 3), which was statistically significant for 3TC+bDRV (median difference, +0.05; IQR, –0.06, +0,14; p = 0.01; +8%). The combination of bDRV+DTG rose by 3% (+0.017; IQR, –0.06, +0.07; p = 0.6), whereas both the combination of DTG+RPV (median difference, 0.008; IQR –0.09, +0.06; increase 1%), and bDRV+RPV (median difference, 0.0007; <1% increase) showed 48 weeks values similar to baseline. According to the different comorbidities, there was a similar increase at 48 weeks in all cases that was statistically significant only for HCV coinfection (median difference, +0.02; IQR, –0.04, +0.09; p = 0.012). Of note, 32 patients received treatment with direct-acting antiviral agents against HCV coinfection during the study, achieving sustained virological responses, and this might have contributed to the CD4/CD8 response, in spite of a similar increment to that observed in non-treated HCV coinfected patients (0.024 vs. 0.019; p = 0.3).
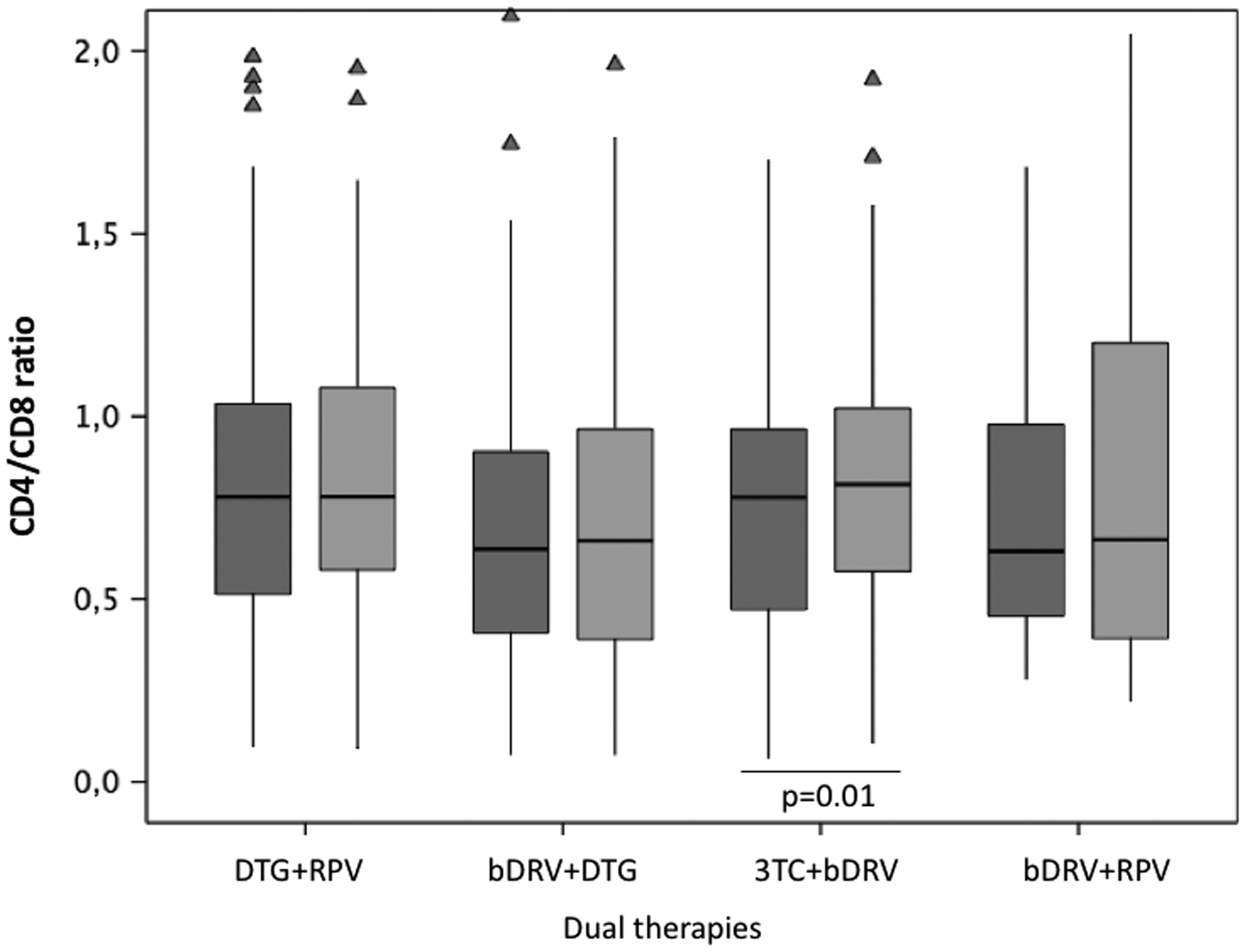
CD4/CD8 ratio at baseline and after 48 weeks according to the different dual regimens. Boxplot indicates median (central line) and interquartile range, lines indicate 95% confidence interval, triangles represent extreme values (outliers).
In the mixed-effects linear model, the CD4/CD8 change was associated with the baseline ratio (estimate, –0.27; 95% CI –0.08, –0.25; p < 0.01) and previous AIDS diagnosis (estimate, –0.08; 95% CI –0.03, –0.14, p = 0.04), and the model did not change after including the different dual regimens. Moreover, the model remained unchanged after adding the different comorbidities.
Discussion
It is known that CD4/CD8 ratio values tended to increase over time with the maintenance of virologic suppression. However, some retrospective or observational studies suggest less benefit when using a dual antiretroviral regimen, attributed to the loss of control of HIV replication.2,6 This is important, since patients with a low CD4/CD8 ratio on therapy, or less improvement in the CD4/CD8 ratio, could have persistent immune activation, immune senescence phenotype, residual viremia, and worse clinical and immunological outcomes. 7
However, for the first time, here we demonstrate that the use of different dual therapies as a switching strategy is associated with an increase in the CD4/CD8 ratio, a median difference of +0.02 (+3%), and a decrease in the percentage of CD8 T cells. Furthermore, we confirm that the HIV-related characteristics of the patients, such as time on antiretroviral therapy, nadir CD4+ cell count, or previous AIDS diagnosis, determine the baseline ratio, as previously described, 8 and that the baseline CD4/CD8 value is a fundamental factor. Moreover, we observed a lower increase in those patients with the highest baseline values, suggesting a decreased slope as has previously been described in the evolution of the CD4+ cell count after several years of gain. 9
There are few studies detailing the quantitative evolution of the CD4/CD8 ratio to compare our data, since most of them were analyzing the rate of patients reaching threshold values of 1 or of 0.8 without considering baseline values and slope. Castilho et al. described a median CD4/CD8 increase of 0.17 (IQR, 0.06–0.28) after three years in 2006 naïve patients starting antiretroviral therapy with a baseline ratio of 0.57,8 a result higher to that observed in our study taking into account that the highest benefit, in terms of inflammation or immune activation, is achieved during the first years in therapy. 10 There are even fewer available data for dual therapies. In a retrospective study of 570 patients and 1068 regimens, Masia et al. described an overall unadjusted median CD4/CD8 increase of +0.0245 per year on therapy, considering a linear evolution, and this increment was lower in the case of treatment simplification (dual and monotherapies). 2 However, this study did not specify the baseline value or other HIV-related factors at the time of simplification. In a cohort study collecting data from 104 patients, Mussini et al. described an increase of 0.12 with triple therapy and 0.04 with dual regimens at 48 weeks after switching, but the baseline ratios were of 0.76 and 0.85, respectively, and patients receiving dual therapies were older than triple-therapy patients. 6 In accordance with our data in the clinical setting, a panel of different inflammatory markers did not change at 48 weeks after switching from a suppressive regimen to a dual regimen consisting of DTG plus RPV, in comparison with continued triple therapy (SWORD study). 11 Moreover, the ASPIRE study has shown similar residual viremia at 48 weeks in patients receiving a triple therapy or a lamivudine plus DTG dual regimen. 12
We also analyzed the association with different comorbidities. Except for HCV coinfection and a trend for CVD, the tested comorbidities were not associated with a lower CD4/CD8 ratio. Indeed, CKD, proteinuria, and osteoporosis showed a similar or greater ratio, a possible effect of the long-term suppressive antiretroviral therapy but with associated toxicity. 13 Thus, in experienced patients, the ratio could lose its suggested predictive value, as it has also been suggested in a large number of patients in a collaborative cohort. 14 In this study, including nearly 50,000 patients from 13 cohorts, a U-shaped relationship between CD8 and outcome was found, suggesting that there is little evidence that CD4/CD8 ratio could be prognostic for non-AIDS mortality. Also, though lower ratios during suppressive cART have been associated with persistently higher HIV–DNA, 15 a high ratio alone is not representative of a lower reservoir, particularly in older patients with late initiation of treatment. 3
The optimal treatment regimen for CD4/CD8 ratio normalization is unknown. Some studies have suggested a role for the integrase inhibitor family, since a faster CD4/CD8 ratio normalization was observed with raltegravir vs. efavirenz in a subanalysis of the STRTMRK study. 16 In contrast to this result, there was a better evolution with efavirenz vs. DTG in a subanalysis of the SINGLE study. 17 However, most of the studies analyzed time to reach the considered adequate threshold values of 0.8 or 1 by the Kaplan-Meier method, assuming a linear increase, and did not consider the relative changes in the ratio. Indeed, we found a better evolution for boosted protease inhibitor plus lamivudine than that observed with DTG or/and RPV, but the type of dual regimen was not significant after adjusting for baseline ratio and HIV-related factors.
Our study has several limitations. The lack of a control group receiving triple therapy does not allow us to observe the improvement in this population. Second, the comorbidities evaluated were obtained from the clinical record. Thus, we have not studied subclinical atherosclerosis in patients without clinical CVD, a fact that could underestimate our rate of comorbidities. 18 Finally, we did not include in our study cytomegalovirus (CMV) infection, which could modify the CD4/CD8 ratio through the expansion of CMV-specific CD8 cells, 19 and we did not include the role of therapy against HCV coinfection and achievement of sustained virologic response during the study in some patients, although few patients received therapy against HCV during their dual regimen, and this does not seem to alter the CD4/CD8 evolution. 20
In conclusion, this work offers useful data for the clinical management of patients and the interpretation of the CD4/CD8 ratio, and especially for HIV-1-infected patients on dual regimens. For the first time, we confirm that the CD4/CD8 ratio changes are the result of a complex interplay between baseline CD4/CD8 ratio, HIV-related factors, and time on virologic suppression, and that dual therapy does not seem to alter the evolution of this marker. Moreover, our observations suggest that the utility of the CD4/CD8 ratio and its changes as a potential clinical marker for some comorbidities might differ after longer duration on antiretroviral treatment, due to the possible toxicity of some antiretroviral drugs.
Footnotes
Acknowledgements
We would like to thank Ana Abad for their important contribution in database management.
Authors’ contribution
JLC and MM conceived and designed the study and were responsible for patient enrollment, data analysis, and drafted and finalized the article, and MF, AV, PV, and MJV were responsible for patient enrollment, clinically followed up patients, and helped to write the work. All coauthors revised the article and read and approved the final version. All research was conducted within the guidelines of ethical principles, and local legislation.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.