
Abstract
A 56-year-old man acquired HIV infection as the result of bites that caused severe tissue injuries. The features of the biting episode that led to transmission of infection were very similar to those in four other patients reported to have acquired HIV infection as the result of bites. Post-exposure prophylaxis should be recommended for people who have suffered bites that caused significant tissue injuries, inflicted by a person with known HIV infection, who had visible blood staining of their saliva at the time of biting, and an HIV viral load known or presumed to be greater than 3.0 log10 copies/ml.
A 56-year-old man (A) suffered bite injuries during a fight with a 34-year-old man with known HIV infection (B). ‘B’, who had visibly blood-stained saliva from injuries, repeatedly bit ‘A’, causing a compound fracture of the left thumb, and deep tissue injuries to the left cheek that required debridement and suturing.
The HIV transmission risk from the bites was not considered sufficiently high for ‘A’ to be provided with post-exposure prophylaxis (PEP). However, 41 days after suffering the bites, ‘A’ presented with a two-week history of lethargy, confusion and ataxia. Acute HIV infection was diagnosed on the basis of an indeterminate Western Blot and a plasma HIV viral load of 6.01 log10 copies/ml. An HIV EIA performed on the day of the fight had been negative. ‘A’ consistently denied behaviour that would have put him at risk of acquiring HIV infection.
The HIV viral load was not measured in ‘B’ immediately following the fight. He had a long history of intermittent adherence to antiretroviral therapy (ART). Approximately 40 months previously, while not receiving ART, his HIV viral load was 4.2 log10 copies/ml. After approximately six months during which he had not been dispensed ART, he recommenced ART, which he took consistently for six weeks prior to the fight, and for many weeks following the fight. His HIV viral load 29 days after the fight was 2.30 log10 copies/ml. Genotypic HIV resistance testing performed on blood samples, collected from ‘B’ three years prior to the fight, and from ‘A’ 43 days after the fight, showed 99% (329/331) homology of the reverse transcriptase and protease amino acids.
Discussion
A recent systematic review 1 identified four published reports of ‘confirmed’ or ‘highly plausible’ transmission of HIV infection as the result of bite(s) inflicted by people with HIV infection (Table 1).2–5 Three cases considered ‘confirmed’ fulfilled all of the following criteria: the bitten person had a documented negative HIV test in close temporal proximity to the bite; seroconversion was documented in the bitten person within two months of the bite; phylogenetic analysis showed a high degree of similarity between the viruses infecting the biter and the bitten person, and no other risk factors for HIV infection could be identified in the bitten person. One case in which a phylogenetic analysis had not been performed, but which fulfilled all the other criteria, was considered ‘highly plausible’. Using the same criteria, the present case would be considered a ‘confirmed’ case of HIV transmission via a human bite.
Reported cases of confirmed or highly plausible transmission of HIV infection by bites.
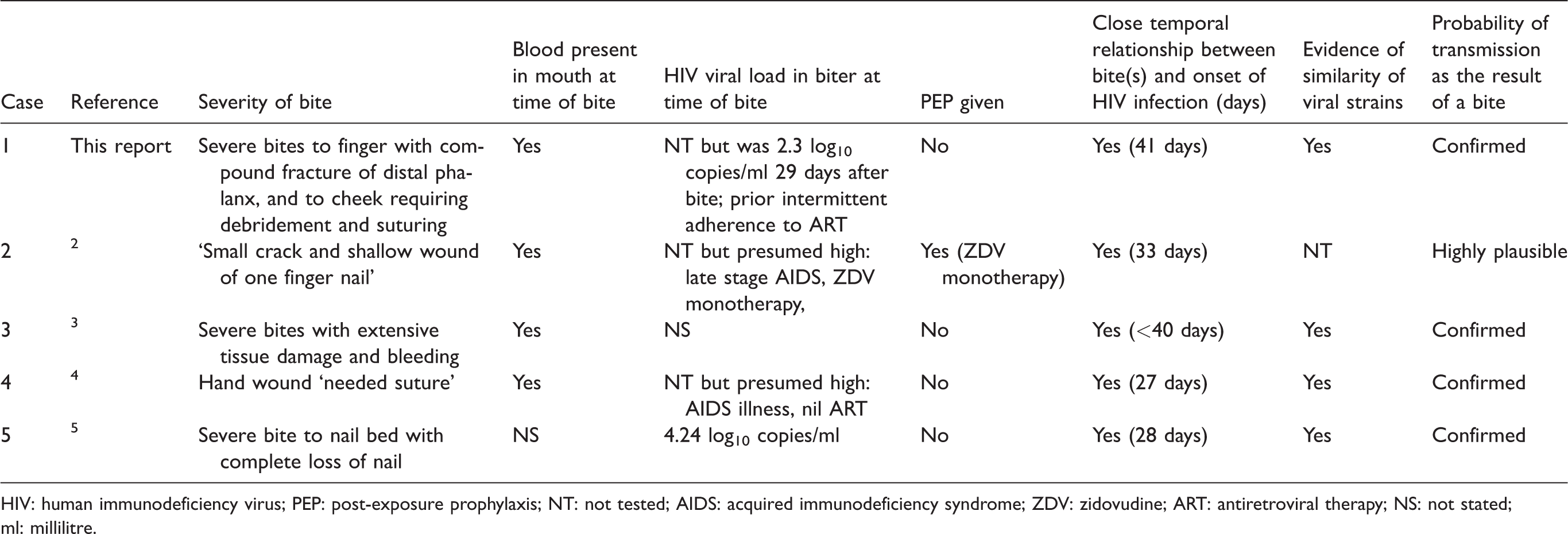
HIV: human immunodeficiency virus; PEP: post-exposure prophylaxis; NT: not tested; AIDS: acquired immunodeficiency syndrome; ZDV: zidovudine; ART: antiretroviral therapy; NS: not stated; ml: millilitre.
Of these five cases with confirmed or highly plausible transmission, blood was noted to be present in the saliva of the biter in four cases; significant HIV viraemia (>3.0 log10 copies/ml) in the biter close to the time of the incident was confirmed in one case, and presumed very likely in three cases; and the bitten person’s injury was described as ‘deep’ and/or ‘severe’ in four cases, two of whom required suturing (Table 1). In two confirmed cases, the biter had a history of recently receiving ART, although in both cases therapy was sub-optimal, and neither of the two biters had documented viral suppression at the time the bites were inflicted.
The small number of published case reports strongly suggests that transmission of HIV infection as the result of a bite by an infected person is extremely rare. However, these five cases suggest that bites that have been inflicted by a person with visible blood contamination of the saliva, and that cause severe and/or deep tissue injury, pose a definite risk of transmitting HIV infection. There are insufficient data to estimate the magnitude of this risk. Current guidelines state that the risk of transmission is <1/10,000 6 or ‘negligible’ 7 from human bites, but recommend that non-intact skin contamination with ‘any body fluid that is visibly contaminated with blood’ should be considered for PEP.6,7
Based on the features in five cases with confirmed or highly plausible transmission of HIV infection as the result of a bite, we recommend that PEP should be recommended for patients who fulfil all of the following criteria: (a) The biter’s saliva was visibly contaminated with blood; (b) the biter is known or suspected to have a plasma HIV viral load >3.0 log10 copies/ml and (c) the bite has resulted in severe and/or deep tissue injuries. Although the biter’s history of ART should be considered, a history of recent ART should not necessarily exclude the prompt provision of PEP. Of course, if the HIV viral load is undetectable then there is no risk of transmission (U = U) and PEP is not required.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.