
Abstract
People living with HIV (PLWH) are dying of non-AIDS associated conditions, including type 2 diabetes and chronic kidney disease (CKD), but the impact of diabetes and CKD on HIV survival rates is unknown. The purpose of this retrospective longitudinal study was to investigate the impact of diabetes and CKD on the survival rates of PLWH, using a secondary analysis of data from the Centers for AIDS Research Network of Integrated Clinical Systems (N = 10,043 PLWH). The sample was divided into three comorbidity groups: HIV alone, HIV with diabetes, and HIV with diabetes and CKD. Kaplan–Meier analysis was used to examine survival rates; Cox regression was used to assess relationships between variables. Overall mean survival time was 19.7 years (95% CI, 19.57–19.8). For HIV alone (n = 8266), the mortality rate was 3.6%; for HIV with diabetes (n = 1720), mortality was almost three times higher (12.0%); and for HIV with diabetes and CKD (n = 57), survival was less than three times higher (36.8%) than for HIV alone. Knowing that diabetes mellitus decreases survival rates, healthcare providers need to halt or delay the onset of type 2 diabetes by more aggressively assessing for prediabetes and treating it.
Background
Globally, at the end of 2018, approximately 36.9 million people were living with HIV 1 ; in 2014, the mortality rate for people living with HIV (PLWH) was 4.7 per 100,000. 2 Since the development of combination antiretroviral therapy (cART) in the mid-1990s, 3 the life expectancy of PLWH has increased to approach that of the general population,4,5 with the result that PLWH are now dying increasingly from other causes, such as heart disease, diabetes, kidney disease, and cancer.
Among PLWH over 50 years old, approximately 60% have at least one comorbid condition. 6 Diabetes mellitus (DM) is one of the most common,7–9 in part because HIV causes inflammation through the secretion of pro-inflammatory cytokines, which can lead to insulin resistance.10,11 In addition, because certain cART treatments themselves cause insulin resistance, cART can lead to DM as well. 12 PLWH with DM have higher rates of cardiovascular and renal damage than do those with HIV alone.13,14
Another comorbid condition among PLWH is chronic kidney disease (CKD), with a prevalence three times higher in PLWH than in the general population.15–17 In PLWH, DM is a major risk factor for developing CKD 18 due to increased systemic inflammation, 19 increased insulin resistance, 12 and damaged nephrons (the functional units of the kidney). 20 A small percentage of those with CKD progress to end-stage renal disease21,22 – irreversible kidney damage. 23 The development of CKD in the presence of DM indicates progression and sub-optimal control of DM.
Survival in PLWH is affected by adherence to treatment, weight loss, and opportunistic infections.24–26 Comorbid conditions, such as infection with hepatitis C virus, can also reduce survival to varying degrees. 27 The extent to which other comorbid conditions decrease survival, however, remains unknown. The purpose of this study was to ascertain the impact of DM and CKD on survival in PLWH.
Methods
Study setting and participants
This was a longitudinal comparison study using multisite national HIV cohort data from the Centers for AIDS Research (CFAR) Network of Integrated Clinical Systems (CNICS). The data are from CNICS patients over 18 years old who had received cART for over six months and had visited at least one of the eight CNICS clinics. The clinics are located at Case Western Reserve University, the University of Alabama at Birmingham, University of California San Francisco, the University of Washington, University of California San Diego, Fenway Health/Harvard University, the University of North Carolina at Chapel Hill, and Johns Hopkins University. The data were extracted from the CNICS medical records for people who visited a clinic at least once from 2006 to 2015. Post hoc analysis indicated that a sample size of 183 participants would be sufficient for this study; the size of the sample obtained from CNICS was much larger (N = 10,043 PLWH). The study was exempted by the Institutional Review Board at the University of Texas at Austin because the data were de-identified.
Disease verification and survival ascertainment
CNICS defines a diagnosis of DM as HbA1c >6.5 mmol/mol or taking DM-related medications. Diagnosis of CKD is defined by the CKD Epidemiology Collaboration (CKD-EPI) equation, in which creatinine levels <60 ml/min/1.73 m2 are considered indicative of CKD. 28 Diagnosis for both DM and CKD was verified via medical record review and/or adjudication, as part of CNICS protocol. Diagnosis status was assessed at all visits for patients. Mortality data from the CNICS medical records, which include mortality certification from state vital records and the National Death Index (NDI+), enabled us to ascertain survival rates. We examined survival rates in three groups.
Variables
Age was treated as a continuous, bivariate variable with two groups (≤50 years, >50 years). Current gender had three options: male, female, or transgender. Ethnicity was treated as nominal data (White, White-Hispanic, African American, African American-Hispanic, Hispanics, and Other). Two lab values were included: HbA1c and CD4 cell count. Viral load (VL) had too many missing data (90%) and could not be included in the analysis. All demographic variables had missing data less than 3%; no imputation was needed. We divided the patient population into three groups: HIV alone (PLWH-only), HIV with comorbid DM (PLWH + DM), and HIV with comorbid DM and CKD (PLWH + DM + CKD). Four groups were originally intended, but there were no instances of HIV with comorbid CKD alone (PLWH + CKD) in the dataset. To examine CKD occurrence, we used a dichotomous variable (0 = have CKD, 1 = do not have CKD).
Statistical analysis
Descriptive statistics included means, frequencies, standard deviations, and percentages. Before conducting the analyses, the accuracy of the data was assessed to exclude bias due to missing data. Missing data were assessed as missing at random and were excluded. Kaplan–Meier analysis was used to examine survival rates. Survival time was based on the number of deaths per 100 person-years of follow-up time. Factors included type of disease (PLWH-only, PLWH + DM, PLWH + DM + CKD), age, ethnicity, current gender, CD4 cell count, HbA1c level, age at initial clinic visit, and the two age groups (≤50 years old, >50 years old). We compared survival analysis of each group and by age at patients’ initial clinic visits, because comorbid conditions occur more frequently in older adults.29–31 Survival rates across groups were compared using the log-rank test. We assessed the relationships between variables (two age groups, current gender, ethnicity, HbA1c, CD4 cell count, age at initial clinic visit, and comorbidity groups) with survival rates using Cox regression. We adjusted confounding factors, which included current gender, ethnicity, HbA1c level, CD4 cell count, age at initial clinic visit, and condition type (PLWH, PLWH + DM, PLWH + DM + CKD) using a backward-stepwise approach. All analyses were performed using IBM SPSS version 23.0 and assessed for significance with α*** set at .01.
Results
Participants’ characteristics
Of the 10,043 HIV-infected persons enrolled in CNICS from 2006 through 2015, a total of 8266 had HIV without DM or CKD (see Table 1); 1720 were PLWH + DM; and 57 were PLWH + DM + CKD. Most PLWH-only were younger than 50 years (69.8%), male (84.7%), and White (51.3%). In addition, most were fairly healthy, and only about one third (36.7%) had CD4 cell count of fewer than 500 cells/µl. The dominant age group of PLWH-only at initial clinic visit was 30–39 years (34.6%).
Study characteristics by disease groups (PLWH, PLWH + DM, PLWH + DM + CKD).
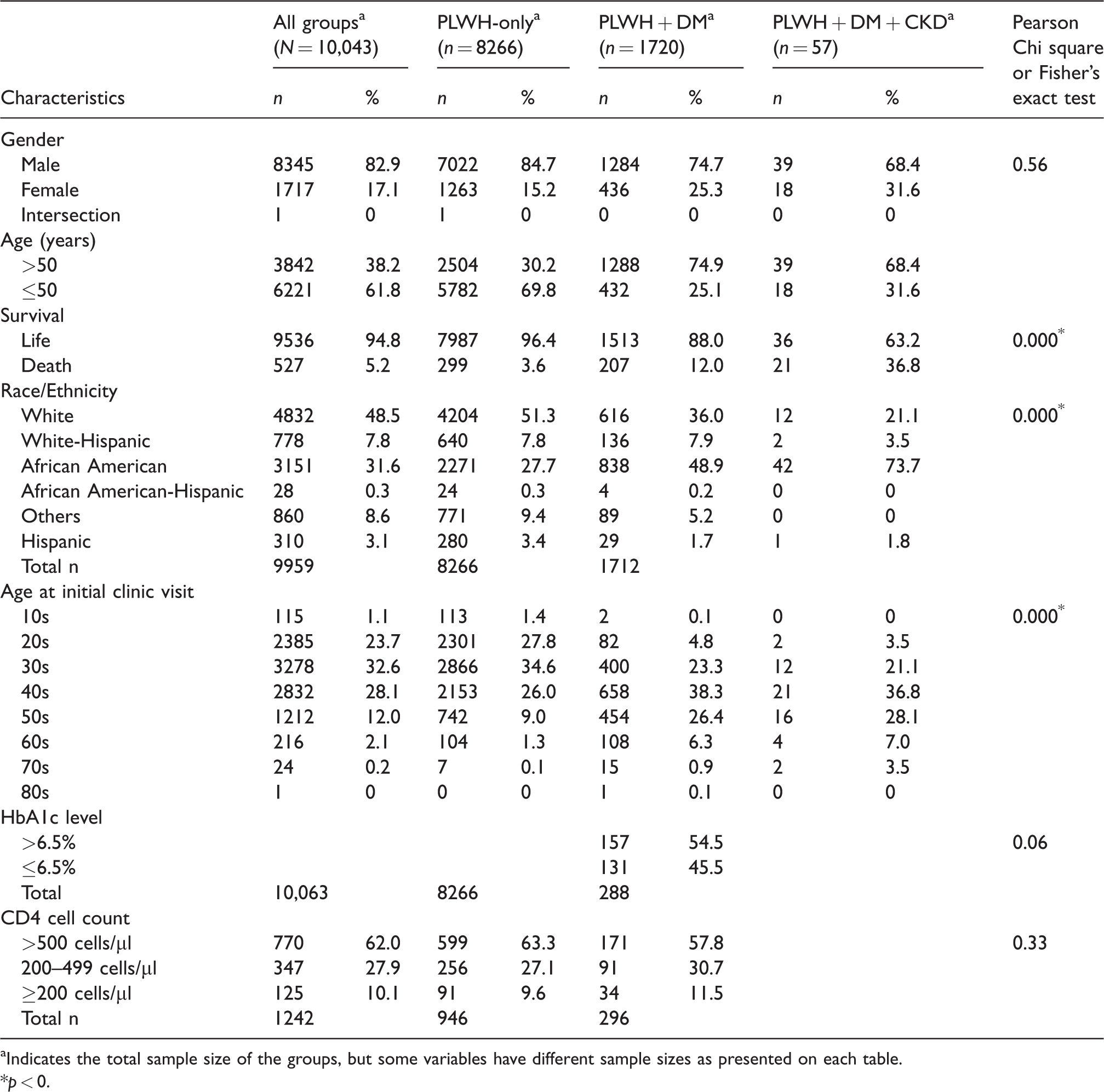
aIndicates the total sample size of the groups, but some variables have different sample sizes as presented on each table.
*p < 0.
Most PLWH + DM were male (74.7%), over 50 years old (74.9%), and African American (48.9%). The dominant age group for PLWH + DM at initial clinic visit comprised those in their 40s (38.3%). Most (54.5%) had a baseline HbA1c >6.5 mmol/mol. Most PLWH + DM + CKD were male (68.4%), over 50 years old (68.4%), and African American (73.7%). As with PLWH + DM, the dominant age group at the initial clinic visit consisted of those in their 40s (36.8%).
The prevalence of concurrent DM and CKD increased with age. PLWH-only were predominantly younger, with most of them under 50 years, but PLWH + DM and PLWH + DM + CKD were mostly over 50. Survival rates decreased with comorbid conditions. Three times as many PLWH + DM + CKD (37%) as PLWH + DM (12%) and three times as many as PLWH-only (3.6%) died from 2006 through 2015 (p = .0001).
Survival analysis
Overall, 494 people died in the study period (see Table 2). The mean survival time was significantly higher for PLWH (20.1 years per 100 person-years, 95% CI 20.0–20.2) than for PLWH + DM (18.7 years, 95% CI 18.4–19.0, p < .01) and PLWH + DM + CKD (15.4 years, 95% CI 13.6–17.3, p < .01). (For survival rates, see Table 3.)
Survival rates for each group.
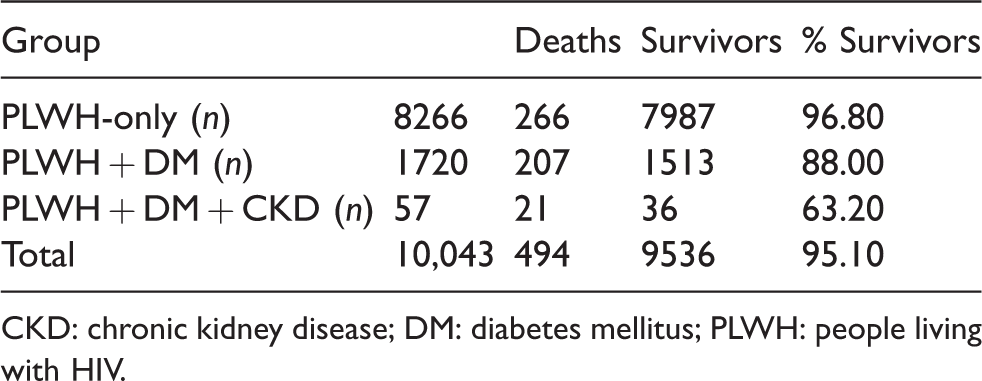
CKD: chronic kidney disease; DM: diabetes mellitus; PLWH: people living with HIV.
Survival time means according to disease categories.
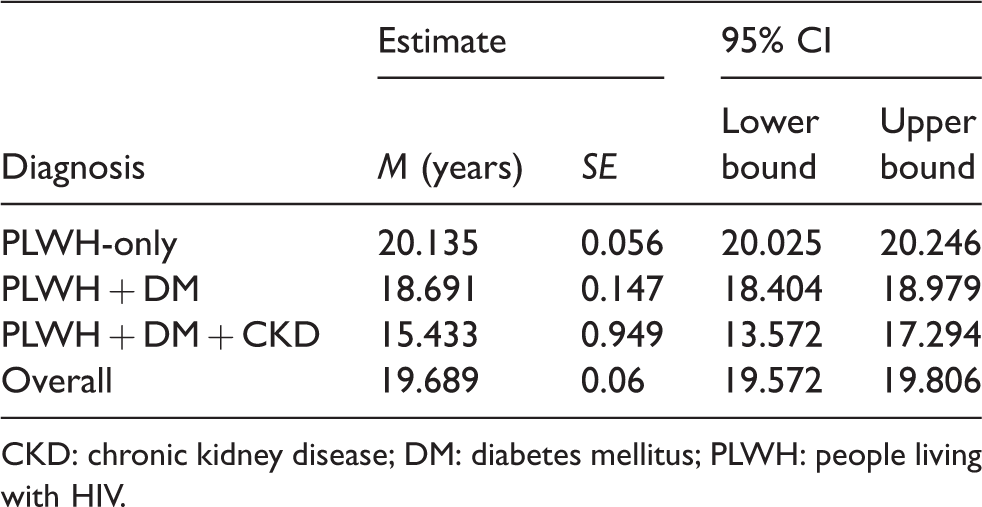
CKD: chronic kidney disease; DM: diabetes mellitus; PLWH: people living with HIV.
Of PLWH-only, most were less than 30 years old at their initial clinic visit, and the group with the lowest survival rate was less than 30 years old. However, PLWH + DM and PLWH + DM + CKD were older than 30 at their first clinic visit, and most died when older than 30 years (see Table 4).
Distribution of age at initial clinic visit and survival.
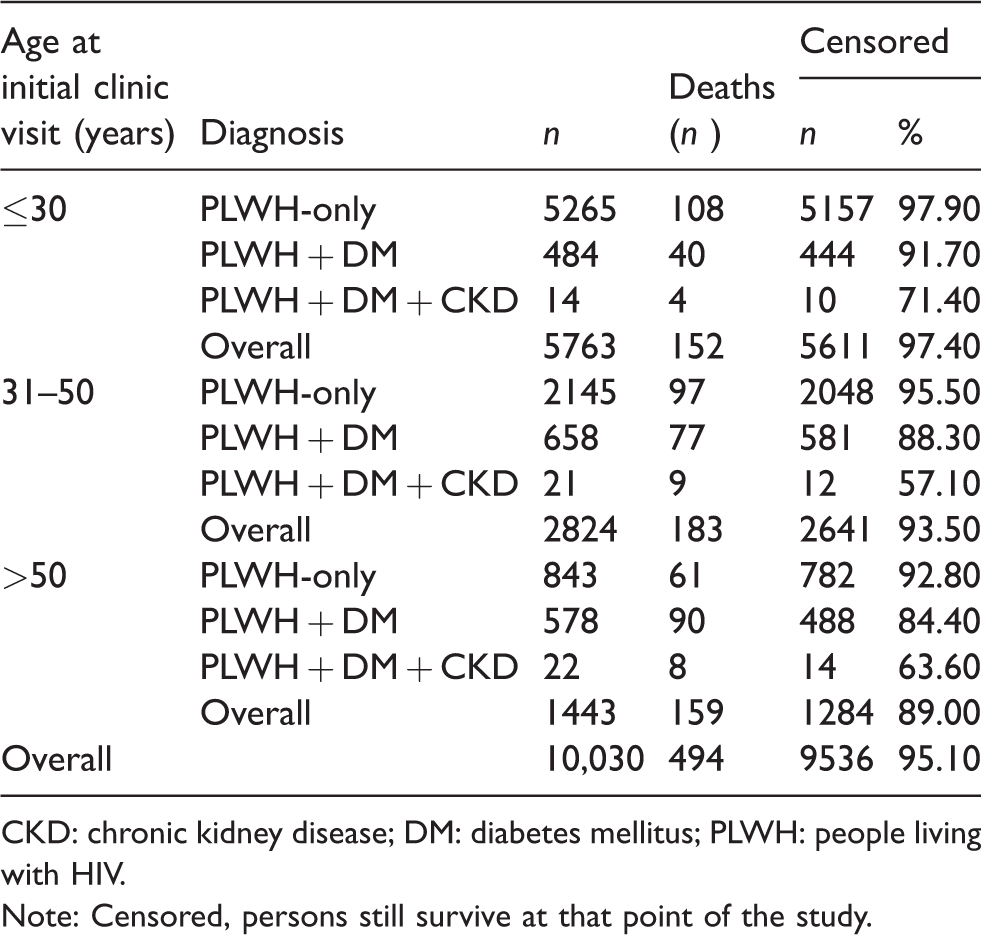
CKD: chronic kidney disease; DM: diabetes mellitus; PLWH: people living with HIV.
Note: Censored, persons still survive at that point of the study.
Survival time refers to the difference from the beginning of a period of observation (in this study, the age at initial clinic visit) until an event (in this study, the patient’s death). Comparison of survival times showed that when age at initial clinic visit was older, the survival time was reduced regardless of comorbidity group (see Table 5). In PLWH-only, age at the initial clinic visit was usually less than 30 years, and patients lived on average 20 years after the initial clinic visit, whereas patients whose age at initial clinic visit was more than 50 years lived only about 18 years. In PLWH + DM, if the age at initial clinic visit was less than 30 years, survival time approached 20 years, but if the initial clinic visit occurred at more than 50 years of age, the survival time decreased to about 17 years. PLWH + DM + CKD whose age at initial clinic visit was less than 30 years lived more than 18 years, but if their age at initial clinic visit was more than 50 years, their survival time was less than 13 years. Thus if PLWH have comorbid conditions, their survival time is significantly reduced (see Figure 1).
Survival time means by age at initial clinic visit by disease categories.
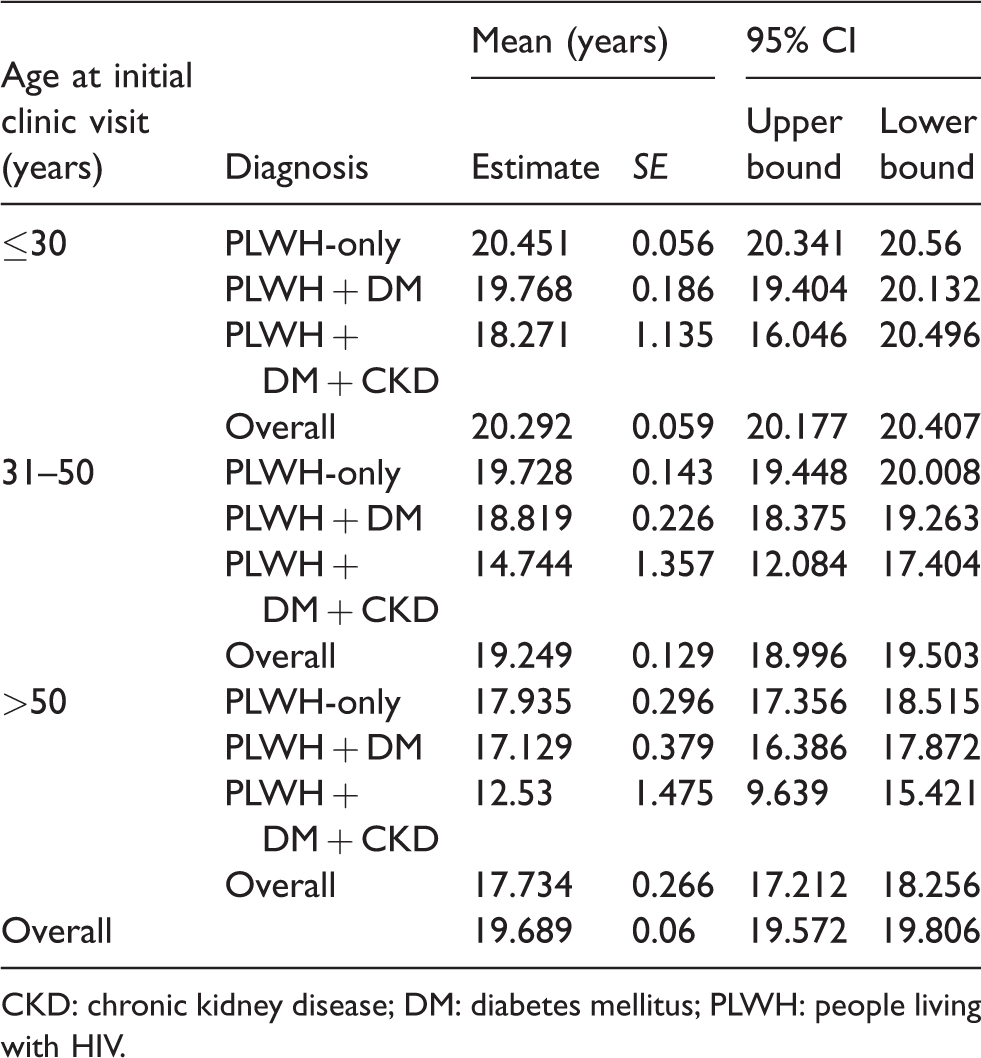
CKD: chronic kidney disease; DM: diabetes mellitus; PLWH: people living with HIV.

Kaplan–Meier survival curves for all-cause survival rates among patients classified by all age disease group (PLWH, PLWH + DM, PLWH + DM + CKD), log rank p < 0.01. Note: Censored: persons still survive at that point of the study; DM: diabetes mellitus; Dx: diagnosis; PLWH: people living with HIV.
Cox regression analysis was conducted for risk factors associated with survival rates. We controlled ethnicity, current gender, age groups (≤50 years old, >50 years old), baseline CD4 cell count, baseline HbA1c level, age at initial clinic visit, and comorbidity group. Only age at initial clinic visit and comorbidity group significantly influenced survival rates. Patients 31–50 years old at the initial clinic visit had a survival rate 2.2 times lower than did those less than 30 years old at initial clinic visit (p < .01, CI 1.8–2.7; see Table 6). Those over 50 years old at initial clinic visit had a survival rate 4.3 times lower than the rate for those less than 50 years at the initial clinic visit (p < .01, CI 3.4–5.4). Compared with PLWH-only, PLWH + DM had a 1.787 times lower survival rate (p < .01, CI 1.5–2.2), and PLWH + DM + CKD had a 4.7 times lower survival rate (p < .01, CI 3.0–7.4).
Risk factors in survival rates.

CKD: chronic kidney disease; DM: diabetes mellitus; PLWH: people living with HIV.
Discussion
This analysis of the CNICS dataset shows that DM and CKD in PLWH negatively impacted survival rates (p < .01). PLWH-only lived almost 5 years longer than PLWH + DM + CKD and almost 1.5 years longer than PLWH + DM. Expected survival times were each reduced by comorbid conditions. These findings agree with previous survival analyses in which comorbid DM decreased survival rates of those with all types of cancer, 32 heart failure, 33 and strokes. 34 In a previous study of PLWH that investigated baseline kidney function (N = 20,132), high and low kidney function were associated with increased mortality. 35 That study did not have data for DM, so whether or not DM was an influential variable is unknown. Knowing that DM decreases survival rates, healthcare providers need to halt or delay the onset of DM by more aggressively assessing for prediabetes and treating it.
In addition, CKD decreased survival rates for PLWH + DM. The survival rates were four times lower for PLWH with co-occurring chronic diseases than for those with HIV alone. No persons in the database had HIV + CKD without also having DM. Thus, PLWH + DM should be screened routinely for CKD and given medication and treatments that are less damaging to the renal system in order to prevent CKD.
The survival analyses show that PLWH who presented at an early age for their initial clinic visit survived longer even if they had comorbid DM or DM + CKD. This finding may point to the benefit of being retained into care as early as possible after diagnosis, 36 because early retention in care positively affects VL suppression and controls CD4 cell count, which are protective against the development of AIDS.16,37,38 It is expected that the older cohort had a decreased life expectancy in comparison with the younger group. It would be important to follow the current CNICS cohort prospectively and compare their survival rates to see whether earlier initial clinic visit ultimately lengthens their life or whether the earlier diagnosis of HIV negates the benefit of long-term care.
Limitations and future research
Although the sample for this study was large, the study has limitations. This was a secondary analysis, limited to the variables included in the dataset. Thus, for example, we were unable to ascertain the date or the order of DM diagnosis. Yet the date of DM diagnosis may not be definitive, because it cannot always be interpreted as the date of DM acquisition; people can live with DM for a long time before diagnosis and treatment.39,40 Weight and BMI, though collected, had too many missing or incorrect data to be included in this analysis. Also, although we had access to medication records, we did not have information on corticosteroids, and medications such as steroids may be prescribed by healthcare providers other than those seen at the CNICS clinics. Future researchers might include countries with national electronic medical systems, which would include more detailed histories of medications prescribed across providers and systems.
As a secondary analysis of an existing dataset, this research is dependent on other researchers’ data collection; we could not control the amount of missing data or errors in data entry. In addition, the date of the patient’s initial clinic visit marked the beginning event in the survival analyses, as a substitute for the date of the patient’s exposure to HIV. It is possible that the survival analyses were biased if the patients contracted HIV long before their initial visits. Finally, the definition of DM using HbA1c as a measure may be inadequate in PLWH, because HbA1c underestimates their glucose levels; in PLWH, the life cycle of the red blood cell is often shorter due to hemoptosis.41,42 Future research could investigate the impact of prediabetes on mortality, because the threshold of DM may be set artificially too high to prevent the negative impact for PLWH. Clinicians and researchers should investigate the possibility of adjusting the recommended DM diagnosis HbA1c levels to better reflect this population’s pathophysiology. Using kidney function in conjunction with HbA1c may provide a more complete picture of overall health; previous studies have reported that kidney function at the initiation of HIV treatment can predict mortality in PLWH. 43
Nevertheless, the study’s large sample, enrolled from eight clinics across the U.S. and representing a diverse patient population in both ethnicity and age, does contribute to generalizability to other regions with similar DM prevalence.
Conclusion
This study provides new information about survival rates in PLWH with comorbid conditions that points to the importance of early and consistent monitoring of glucose and kidney function in PLWH. As people live longer with HIV, comorbid chronic conditions must be tightly managed. Traditional methods of monitoring may be insufficient, and earlier intervention for DM along with careful monitoring and tailoring of treatment may be required to preserve kidney function. These findings are important for healthcare providers, researchers, and PLWH with comorbid conditions.
Footnotes
Acknowledgement
The CFAR sites involved in CNICS include the University of Alabama at Birmingham (P30 AI027767); University of Washington (P30 AI027757); University of California, San Diego (P30 AI036214); University of California, San Francisco (P30 AI027763); Case Western Reserve University (P30 AI036219); Johns Hopkins University (P30 AI094189, U01 DA036935); Fenway Health/Harvard (P30 AI060354); and the University of North Carolina at Chapel Hill (P30 AI50410). Editorial support with manuscript development was provided by the Cain Center for Nursing Research and the Center for Transdisciplinary Collaborative Research in Self-Management Science (P30, NR015335) at The University of Texas at Austin School of Nursing. This manuscript contributed to a dissertation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CNICS is an NIH-funded program (R24 AI067039) made possible by the National Institute of Allergy and Infectious Diseases (NIAID) and the National Heart, Lung, and Blood Institute (NHLBI).