
Abstract
Lenacapavir is now approved for highly treatment experienced persons living with HIV (PLWH) and for HIV pre-exposure prophylaxis (PrEP). Limited lenacapavir clinical data exist with real-world drug-drug interactions. We report two possible drug-drug interactions with ambulatory lenacapavir subcutaneous injections in two PLWH prescribed long-acting injection therapy. Case 1 describes a PLWH prescribed clopidogrel after an acute cerebrovascular event receiving an antiretroviral (ARV) regimen including subcutaneous lenacapavir and ibalizumab biweekly infusions. The clopidogrel was discontinued with no harm noted. Case 2 is a highly treatment experienced PLWH prescribed an ARV regimen including subcutaneous lenacapavir and intramuscular cabotegravir/rilpivirine injections on concomitant inhaled and nasal fluticasone. Symptoms consistent with adrenal insufficiency were reported with immediate fluticasone discontinuation and transition to beclomethasone. The patient’s baseline cortisol concentration was low with improvement after fluticasone discontinuation. The electronic medical record alerts were customized to note these possible lenacapavir drug-drug interactions, similar to protease inhibitors/pharmacokinetic boosters (ritonavir and cobicistat) to prevent future events. This case series highlights possible lenacapavir drug-drug interactions and is a precautionary tale to other institutions to consider customizing electronic medical alerts for this novel long-acting injection.
Keywords
With the recent Federal Food and Drug Administration approval of lenacapavir for pre-exposure prophylaxis (PrEP) and highly treatment experienced persons living with HIV (PLWH), real-world drug-drug interaction data are necessary for this long acting injectable (LA-I) antiretroviral (ARV).1–4 Lenacapavir is a substrate and moderate cytochrome P450 (CYP) 3A4 and P-glycoprotein inhibitor with additional metabolism via uridine diphosphate glucuronosyl transferase, 1A1.1–4 Lenacapavir oral lead in for 2 days and every 6-months subcutaneous injections for highly treatment experienced PLWH is expanding with published data demonstrating successful use with concurrent intramuscular cabotegravir/rilpivirine (CAB/RPV) injections for a complete parenteral regimen.5–7 Vigilance is necessary to avoid concurrent use of medications with possible drug-drug interaction potential. We report two possible drug-drug interaction cases (with patient consent) with lenacapavir necessitating a closer evaluation of our institutional processes for LA-I medication review.8,9
Patient case characteristics.
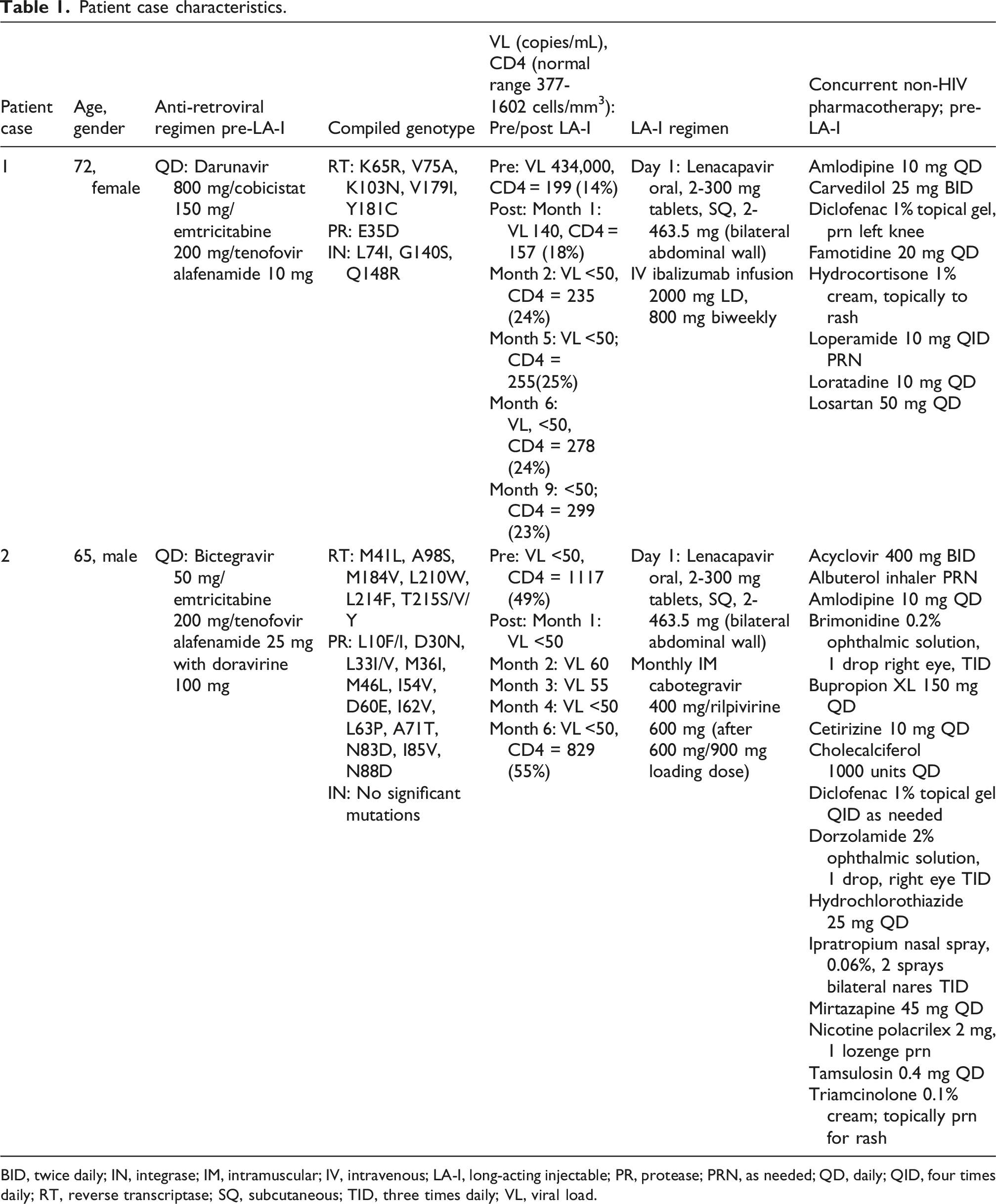
BID, twice daily; IN, integrase; IM, intramuscular; IV, intravenous; LA-I, long-acting injectable; PR, protease; PRN, as needed; QD, daily; QID, four times daily; RT, reverse transcriptase; SQ, subcutaneous; TID, three times daily; VL, viral load.
Case 2: A 65-year-old highly treatment experienced male PLWH requested transition to intramuscular CAB/RPV with lenacapavir (Table 1). Inhaled/nasal corticosteroids at lenacapavir initiation were not noted. At the second monthly CAB/RPV injection, prescription refills for nasal/inhaled fluticasone were reviewed with patient report of daily use. The patient noted dizziness, fatigue and two recent falls. A random afternoon cortisol concentration was 4.0 µg/dL [reference range before 10 AM (3.7−19.4 µg/dL) and after 5 PM (2.9−17.3 µg/dL)] with immediate fluticasone discontinuation. Three days later a morning cortisol stimulation test demonstrated a baseline value of 6.0 µg/dL and 60-min result of 14.7 µg/dL after intramuscular adrenocorticotropic hormone 250 mcg, denoting a partial response. Based on the patient’s hemodynamic stability, the fluticasone prescriptions were transitioned to inhaled beclomethasone inhaler with continuation of ipratropium nasal spray with no oral hydrocortisone initiated.
12
At the 3rd CAB/RPV injection, the patient noted no further dizziness or falls with a repeat morning cortisol = 7.2 µg/dL. A repeat random afternoon cortisol 1 month later = 5.8 µg/dL. Patient education and a clinic medication drug-drug interaction card (Figure 1) with continued beclomethasone and ipratropium use was emphasized with this possible adverse event.
9
Corticosteroids and lenacapavir wallet card.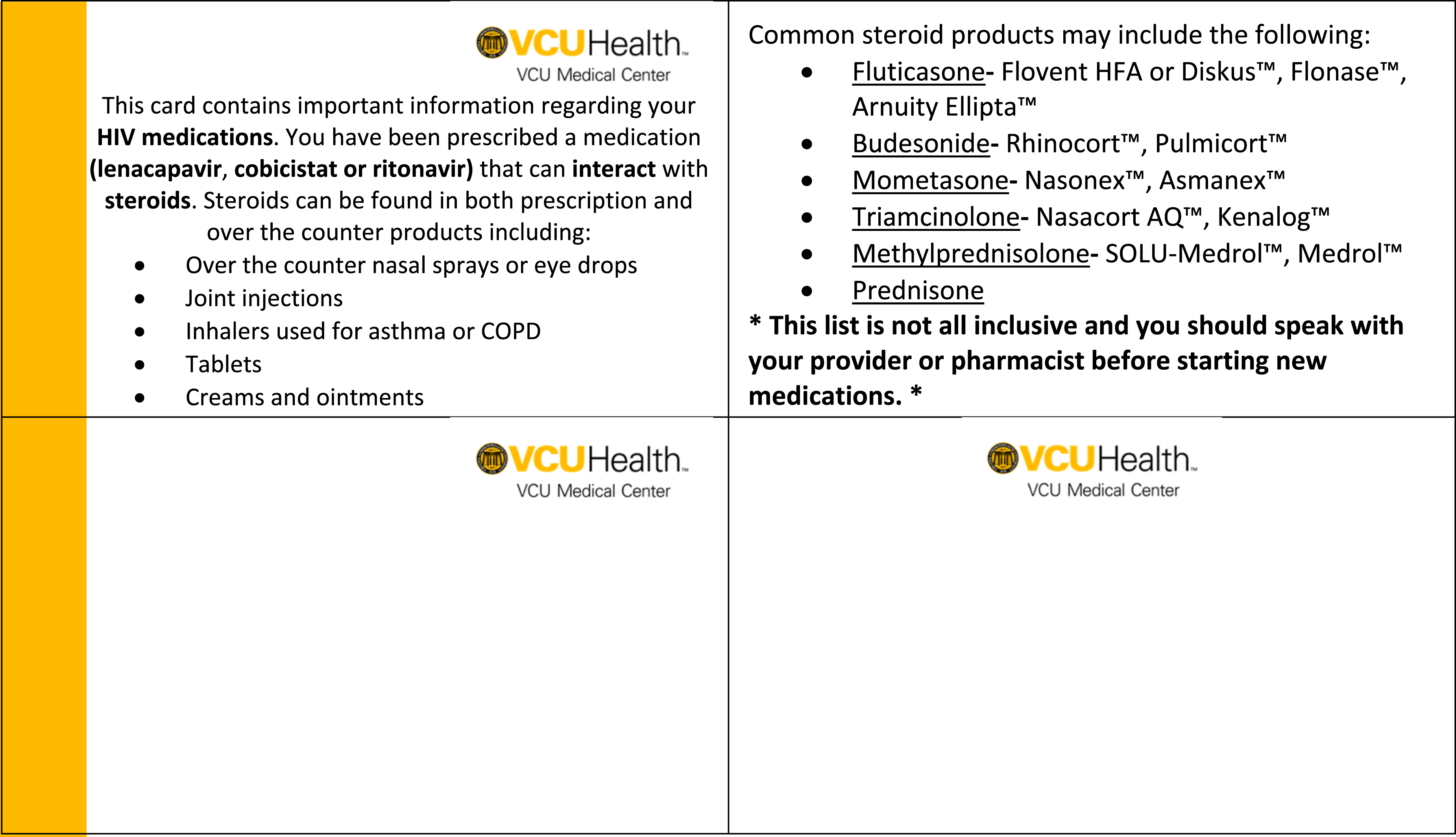
Lenacapavir is a substrate and moderate CYP 3A4 inhibitor with additional metabolism via uridine diphosphate glucuronosyl transferase 1A1. Minimal data to evaluate potential drug-drug interactions are published in real-world studies. In the CAPELLA lenacapavir study for highly treatment experienced PLWH, only 72 persons were followed with no description on drug-drug interactions but exclusion criteria included persons on concurrent corticosteroids, strong CYP 3A4 inducers or uridine diphosphate glucuronosyl transferase inhibitors or inducers. 5 A recent study evaluated the potential for drug-drug interactions in HIV negative persons receiving non-lenacapavir PrEP prescriptions between January 1-December 31, 2024 utilizing the IQVIA LRx Dx database. 13 The primary outcome included a description of concurrent CYP 3A4 and P-glycoprotein medications concomitantly prescribed to PrEP persons and to determine if significant drug-drug interactions would exist with a new lenacapavir prescription. 13 The results demonstrated a primarily male (90.9%) young adult (mean age = 38 years) population. Only 0.5% of PrEP users would necessitate a lenacapavir dose adjustment with concurrent strong CYP 3A4/P-glycoprotein inducers (rifampin, carbamazepine, oxcarbazepine). In 12.6% of persons, a concomitant medication would necessitate a dose adjustment or monitoring before lenacapavir for PrEP is prescribed with the erectile dysfunction medication class [tadalafil (7.45%), sildenafil (4.07%) and vardenafil (0.07%)] representing the most common interacting agents.
In contrast, PLWH prescribed lenacapavir for highly treatment experienced multidrug resistance are usually older (similar to our cases) and are receiving more concomitant medications. Recent data from the Swiss HIV Cohort study highlights increasing polypharmacy trajectories as PLWH age >50 years. 14
No case reports or drug-drug interaction studies are published with lenacapavir and clopidogrel or inhaled/nasal corticosteroids as reported in this case series. Ritonavir is a strong CYP 3A4 inhibitor with numerous contraindicated concurrent medications including both clopidogrel and corticosteroids.8,11 Lenacapavir is a moderate CYP 3A4 inhibitor and guidance recommends consideration for using the lowest corticosteroid dose with adrenal suppression monitoring and avoiding concurrent clopidogrel administration.8,11 Moderate CYP 3A4 inhibitors have less significant drug-drug interactions and may allow concurrent dosing with narrow therapeutic window agents. As an example, diltiazem is a moderate CYP 3A4 inhibitor and published studies may provide guidance with potential lenacapavir drug-drug interactions. 15 In a small analysis of 17 heart transplant patients receiving a median tacrolimus dose of 5.8 mg twice daily, diltiazem [60 mg (N = 5); 90 mg (N = 12)] was prescribed for concurrent hypertension. After diltiazem initiation, a 54% reduction in tacrolimus elimination necessitated dose reduction to 2.8 mg twice daily. Thus, evaluating the literature for drug-drug interactions with moderate CYP 3A4 inhibitors may provide real-world lenacapavir guidance. Of note, a recent case report describes lenacapavir use in a person with a massive hemorrhage during a liver transplantation. 16 The authors noted no observed tacrolimus drug-drug interactions, but details on the specific doses or trough concentrations are not included in the report to determine if any decreased clearance resulted.
These two cases resulted in a review of our lenacapavir drug-drug interaction alerts to allow proper monitoring with recommendations for customizing the electronic medical record. Additional considerations will need to include the lenacapavir long elimination (9 months) half-life as PLWH may continue to be at risk for drug-drug interactions even after discontinuation. 1 Case 2 did not have any adverse events or adrenal insufficiency with concurrent lenacapavir use and inhaled/nasal corticosteroids, but additional data are needed to determine the true clinical significance of this drug-drug interaction. As a safety precaution, we updated our drug-drug interaction card for protease inhibitors used in our clinic with the addition of lenacapavir to assist patient education at treatment initiation (Figure 1). Currently, the FDA label provides the most comprehensive data for lenacapavir DDIs.1,2 These cases serve as precautionary tale for health systems to ensure proper drug-drug interaction monitoring with LA-I lenacapavir as this agent expands use in highly treatment experienced PLWH and PrEP.
CPD questions
(1) Lenacapavir is a substrate of which metabolic and transport proteins? (a) Cytochrome P450 1A2 (b) Multidrug and toxin extrusion protein-1 (c) Cytochrome P450 3A4, uridine diphosphate glucuronosyl transferase 1A1 and p-glycoprotein (d) Organic cationic transporter −2
The correct answer is C.
Lenacapavir is a substrate of cytochrome P450 3A4, uridine diphosphate glucuronosyl transferase 1A1 and p-glycoprotein. Lenacapavir is a moderate inhibitor of CYP 3A4 and p-glycoprotein. (2) A 72-year-old person living with HIV is initiated on concurrent lenacapavir oral and subcutaneous injections with intravenous ibalizumab infusions for highly treatment experienced multidrug resistant HIV. The patient is currently prescribed clopidogrel 75 mg daily for a recent cerebrovascular accident. What are the next steps to avoid a significant drug-drug interaction? (a) Continue clopidogrel with no intervention. (b) Stop clopidogrel and start atorvastatin. (c) Speak with the patient’s prescribing provider and review the potential for decreased antiplatelet activity with lenacapavir and clopidogrel and review treatment alternatives. (d) Substitute dipyridamole for clopidogrel.
The correct answer is C.
Explanation: Clopidogrel is a prodrug metabolized by cytochrome P450 3A4, 2C19 and 2B6 to the active drug. Lenacapavir is a moderate CYP 3A4 inhibitor and may decrease the clopidogrel antiplatelet effects by inhibiting the conversion to the active agent. The patient will also require a statin, but this would not substitute for the antiplatelet agent. Dipyridamole would not be recommended as the drug of choice for the recent cerebrovascular accident. (3) A 65-year-old person living with HIV is initiated on intramuscular cabotegravir/rilpivirine with oral and subcutaneous lenacapavir. On medication review, the patient is prescribed fluticasone/salmeterol inhaler. What should be recommended to avoid any adverse effects? (a) Continue fluticasone/salmeterol without intervention. (b) Discontinue fluticasone/salmeterol and substitute with budesonide/formoterol. (c) Recommend to substitute fluticasone/salmeterol for beclomethasone and salmeterol inhalers. (d) Discontinue fluticasone/salmeterol and substitute with ipratropium nebulization.
The correct answer is C.
Explanation: Lenacapavir is a moderate cytochrome P450 3A4 inhibitor and may increase the fluticasone concentrations resulting in Cushing syndrome with subsequent adrenal insufficiency effects. Beclomethasone does not interact with strong inhibitors (e.g., ritonavir) in a drug-drug interaction study and would be a safe option for substitution. Budesonide is similarly metabolized by cytochrome P450 3A4 and thus would not be an option for substitution. Ipratropium is an anticholinergic medication and would not be the best option for substitution.
Footnotes
Acknowledgements
The authors wish to thank Alice Tseng, PharmD., who provided the corresponding author with the manuscript on diltiazem as a moderate CYP 3A4 inhibitor. The authors wish to acknowledge Addison Taylor, PharmD., for her work on the Drug-Drug Interaction card for the ID clinic.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.