
Abstract
Pregnant and postpartum women in Southern Africa are at increased risk of HIV infection. Pre-exposure prophylaxis in pregnancy and postpartum periods could significantly reduce the risk of HIV acquisition and transmission in pregnancy. Participants at a community health clinic in Cape Town completed a survey about demographic and sexual risk behaviors, and prior knowledge of pre-exposure prophylaxis. We evaluated factors associated with knowledge of pre-exposure prophylaxis using multivariable logistic regression. We enrolled 50 pregnant and 37 postpartum women, of whom 51% were HIV-uninfected. Twenty-nine (33%) knew about pre-exposure prophylaxis, most from their healthcare provider (69%). Older age (adjusted odds ratio [aOR]/year = 1.09, 95% CI = 1.00–1.19), unintended pregnancy (aOR = 3.36, 95% CI = 1.06–12.12), and more than one sex partner in the last year (aOR = 5.31, 95% CI = 1.12–30.07) were associated with pre-exposure prophylaxis knowledge. Our study identified low levels of pre-exposure prophylaxis knowledge in pregnant and breastfeeding women, but increased knowledge in higher risk women. These results provide guidance to develop interventions to increase pre-exposure prophylaxis knowledge and uptake.
Introduction
Pregnant and early postpartum women in Africa are at increased risk of incident HIV infection, likely due to a combination of behavioral and physiologic changes.1,2 Incident HIV infection in this vulnerable population is challenging because, if not treated to reduce viral load, perinatal transmission of HIV can occur. HIV acquisition during pregnancy or breastfeeding is a major factor in perinatal transmission of HIV, contributing to 25% or more of such transmissions by recent estimates.3,4
Public health interventions to reduce the risk of HIV transmission continue to emphasize safe sex practices, especially regular condom use. 5 Viral suppression of the HIV-infected partner via antiretroviral therapy (ART) also significantly reduces the risk of HIV transmission in serodiscordant couples.5–7 However, those methods require couples testing or disclosure of status, and then partner buy-in to take ART when HIV-infected status is known, or to agree to condom use and the implication of HIV risk. These factors, coupled with gender power differences in some relationships, have led to significant barriers to preventing sexual transmission of HIV.8,9 Research has demonstrated that in pregnant women, condom use decreases by up to half compared to before pregnancy, and HIV incidence increases twofold, a fact that is partly attributable to behavioral factors, in addition to biological factors such as hormone and immune system changes in pregnancy.1,10
To protect women and contribute to the elimination of vertical (mother-to-child) transmission of HIV, the World Health Organization (WHO) recommends offering tenofovir (TFV)-based oral pre-exposure prophylaxis (PrEP) to pregnant and postpartum women at risk for HIV in high-burden settings.11–14 PrEP became available in South Africa when tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) was approved for this use in 2015. In May 2016, South Africa updated their guidelines to “offer and promote PrEP as an additional option in the context of combination prevention”. 15 Despite WHO guidance, however, PrEP has not yet been approved for use in pregnant or breastfeeding women in South Africa. 16 Lack of comprehensive safety data led the South African Department of Health to recommend against PrEP for pregnant mothers stating that it is “contra-indicated”.16,17 Use of PrEP during pregnancy is gaining attention as studies demonstrate that TDF/FTC is safe and effective at preventing HIV acquisition in pregnancy.13,14,18–20 Despite clear evidence that PrEP use prevents HIV acquisition, studies in heterosexual couples have seen mixed results, perhaps due to social and behavioral factors that lead to decreased uptake and adherence.21–23 Such factors likely include stigma against HIV and ART leading to hesitancy to take a similar HIV medication, as well as a lack of awareness and understanding of the science underlying PrEP itself, particularly as PrEP is in the early stages of rollout to the public at large.12,24,25 To ensure that PrEP has a maximal benefit as it is publicly available, characterizing public knowledge of PrEP is an important step to identifying opportunities for enhanced education.
In this study, we surveyed pregnant and postpartum women, both HIV-uninfected and -infected, about their knowledge of PrEP, as part of a broader study evaluating sexual behaviors and relationships during pregnancy. By identifying personal, demographic, and relational factors associated with PrEP knowledge, we aim to provide insight into current levels of understanding of this prevention option and potential gaps in knowledge and future uptake. We included HIV-infected pregnant and postpartum women to evaluate if their knowledge about PrEP was greater than HIV-uninfected women, and to understand if they may influence their peers to take (or not take) PrEP once it becomes available. This analysis will inform the educational component of future research into PrEP interventions, which will be critical to developing strategies to maximize PrEP uptake and adherence in this vulnerable population.
Methods
From September 2016 to December 2016, we consented and enrolled pregnant and postpartum women at an urban maternal obstetrics unit in a community health clinic in an informal settlement outside Cape Town, South Africa. This site is a highly active clinic: it serves a population of 350,000 and has an estimated HIV prevalence of 30%, compared with an average prevalence across urban informal settlements in South Africa of 20%.5,26 The clinic as a whole receives about 4800 new antenatal care visits annually.26,27 Although the clinic has a well-established research site, all participants are recruited from the clinic population at large; there is no specific booking for research study participation prior to self-referring to the clinic.
Enrolment in this study took place as part of a larger study on sexual behavior changes during pregnancy and postpartum periods.2,28 A trained counselor informed all eligible women of the risks and benefits of participation prior to consenting. Women received reimbursement for transportation (R100; about 8 USD) and a snack during their study visit.
The counselor administered a 30-min survey in English or the local language, isiXhosa. The survey consisted of demographic, behavioral, and relationship questions.
At the end of the survey, the counselor gave participants a brief explanation of PrEP, including a definition of the term, the process of taking PrEP as a daily drug, and a note that recent studies showed safety in pregnancy and breastfeeding: “PrEP is short for pre-exposure prophylaxis. It is when antiretroviral drugs, ARVs, that are used to treat those with HIV, are used by people who are HIV negative to prevent them from getting HIV. Research has shown that it is almost 100% effective at preventing HIV if taken every day.”
Participants
We enrolled pregnant and postpartum women (child ≤18 months old) who were attending perinatal care visits. A study counselor screened potential participants for eligibility: criteria for inclusion in the study were (1) ≥18 years old, (2) pregnant or postpartum (6- to 18-month infant), (3) able to speak English or isiXhosa, and (4) willing to participate in the study. For this pilot study, we aimed to enroll 90 women who were enrolled in the larger study on HIV-associated risk behaviors.
Ethics
The Human Research Ethics Committee of the University of Cape Town Faculty of Health Sciences, as well as the Institutional Review Board at the University of California, Los Angeles approved of the study protocol. Trained study staff conducted interviews in private rooms with regular review by the study coordinators. All study materials were coded to maintain participant privacy. No one involved in data analysis had access to identifying information.
Analysis
This was a secondary analysis conducted within a broader study on sexual behaviors among pregnant and postpartum women in Cape Town. 2 We describe continuous variables using means and standard deviations, where normally distributed, and medians with interquartile ranges (IQRs) otherwise. Categorical and binary variables are described using frequencies and percentages. Univariate analysis of categorical variables was conducted using Chi square test or Fisher’s exact test when individual cell counts were small (less than ten). We evaluated the association between demographic and behavioral variables and knowledge of PrEP via logistic regression modeling. We included a priori variables that may be confounders in the model based on prior research on this topic. All analysis was conducted using the R statistical computing package.
Results
We surveyed 87 pregnant and postpartum women about their knowledge of PrEP (50 pregnant [57%], 37 postpartum [43%]) as a subset of a larger study on sexual risk behaviors and substance use in pregnant and postpartum women. Of those, 51% (n = 44) were HIV-uninfected (28 pregnant [56%], 16 postpartum [43%]) and 49% (n = 43) were HIV-infected (22 pregnant [44%], 21 postpartum [57%]). Median age was 29 years (IQR 23, 34) and did not differ by pregnancy status, but HIV-infected women were slightly older (median age = 30, IQR 26–33; vs. HIV-uninfected women’s median age = 27, IQR 22–35). Results are shown in Table 1.
Demographic, relationship, and behavioral data of pregnant and postpartum women by PrEP knowledge (n = 87).
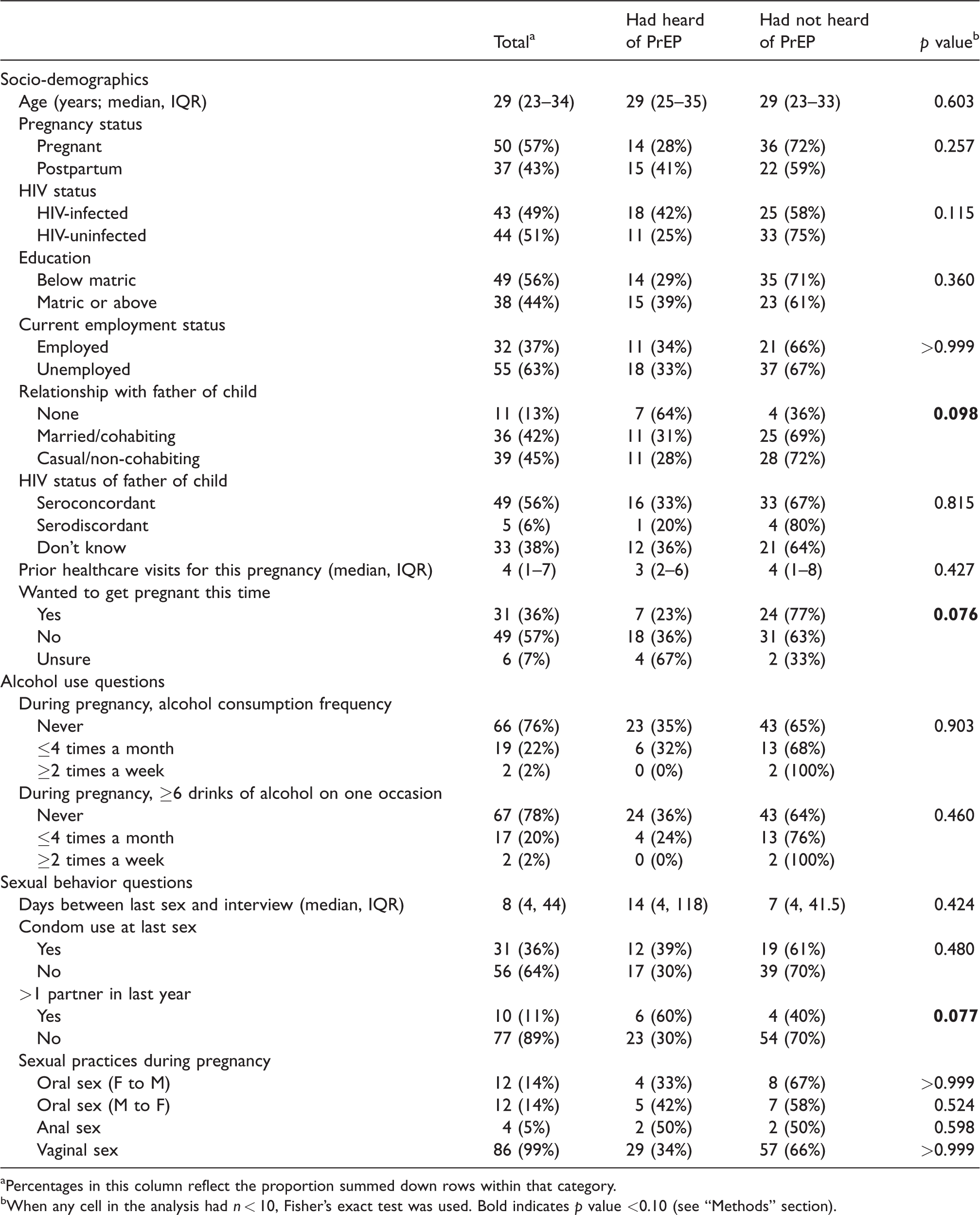
aPercentages in this column reflect the proportion summed down rows within that category.
bWhen any cell in the analysis had n < 10, Fisher’s exact test was used. Bold indicates p value <0.10 (see “Methods” section).
When comparing women by HIV status, there were differences in partner serostatus: 77% of HIV-uninfected women reported being in a seroconcordant relationship versus 35% of HIV-infected women, none serodiscordant (vs. 12% among HIV-infected women), and 23% unsure compared to 53% among HIV-infected women (p < 0.001). There were no other differences by HIV status.
When considering pregnancy status, more postpartum women reported condom use the last time they had sex compared with pregnant women (51% of postpartum and 24% of pregnant women, p = 0.016). No pregnant women reported anal sex during pregnancy, compared with 10% of postpartum women (p = 0.030). In addition, 20% of pregnant women reported having more than one partner in the past year compared to 0% of postpartum women (p = 0.004). Finally, pregnant women attended fewer clinic visits for the index pregnancy, with a median of one visit, versus seven for postpartum women (p < 0.001).
In total, 29 women (33%) reported having heard of PrEP before, while 58 (67%) had not. All 29 women who stated they knew what PrEP was correctly explained it as a medication taken daily to prevent acquisition of HIV. There was no difference in the proportion of women with knowledge of PrEP by age, pregnancy status, or HIV status.
Participants in married/cohabiting or casual/non-cohabiting relationships reported a trend towards less awareness of PrEP than those in no relationship, though this did not reach significance (30.6% vs. 36.0%, p = 0.098). Women who did not intend to get pregnant or were unsure reported non-significantly higher knowledge of PrEP versus women who wanted to get pregnant (40.0% vs. 22.6%, p = 0.076). Finally, of those reporting more than one sexual partner in the past year, 60% heard of PrEP previously, compared to 30% of those with one partner or fewer (p = 0.077).
Those who had previously heard of PrEP cited several sources of information, summarized in Table 2. Data regarding source of PrEP knowledge were missing for two of the women who reported prior knowledge. Table 2 presents data on sources of knowledge by age and pregnancy status. In all groups, the clinic was the most common source of knowledge about PrEP.
Sources of knowledge about PrEP by age cohort and pregnancy vs. postpartum status (n = 27).
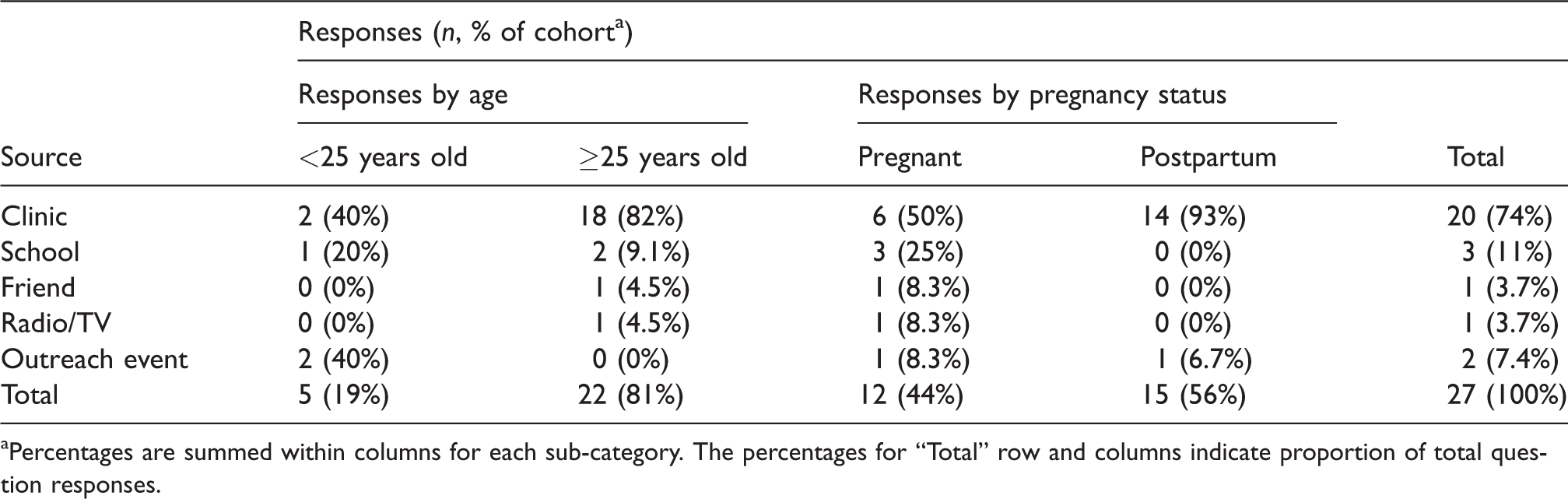
aPercentages are summed within columns for each sub-category. The percentages for “Total” row and columns indicate proportion of total question responses.
Factors associated with prior knowledge of PrEP
We evaluated the association between PrEP knowledge and demographic and behavioral factors, selecting variables that showed differences by PrEP knowledge that reached p < 0.10. The multivariable model demonstrated that age, pregnancy intention, and multiple partners in the past year were associated with PrEP knowledge, adjusting for HIV status (Table 3). Older age (adjusted odds ratio [aOR] = 1.09, 95% confidence interval [CI] = 1.00, 1.19) was associated with 9% increased odds of knowing about PrEP per year increase adjusting for fertility intentions, relationship status, number of sex partners, and HIV status. Additionally, reporting multiple partners in the past year was associated with 5.3 times increased odds of knowing about PrEP (aOR = 5.31, 95% CI = 1.12, 30.07) adjusting for age, fertility intentions, HIV status and relationship status. Women who did not want to get pregnant or were unsure whether or not they wanted to get pregnant had 3.4-times increased odds of knowing about PrEP (aOR = 3.36, 95% CI = 1.06, 12.12) adjusting for age, multiple partners, HIV status and relationship status.
Evaluation of factors associated with PrEP knowledge in pregnant and postpartum women adjusting for a priori confounders (age and HIV status).
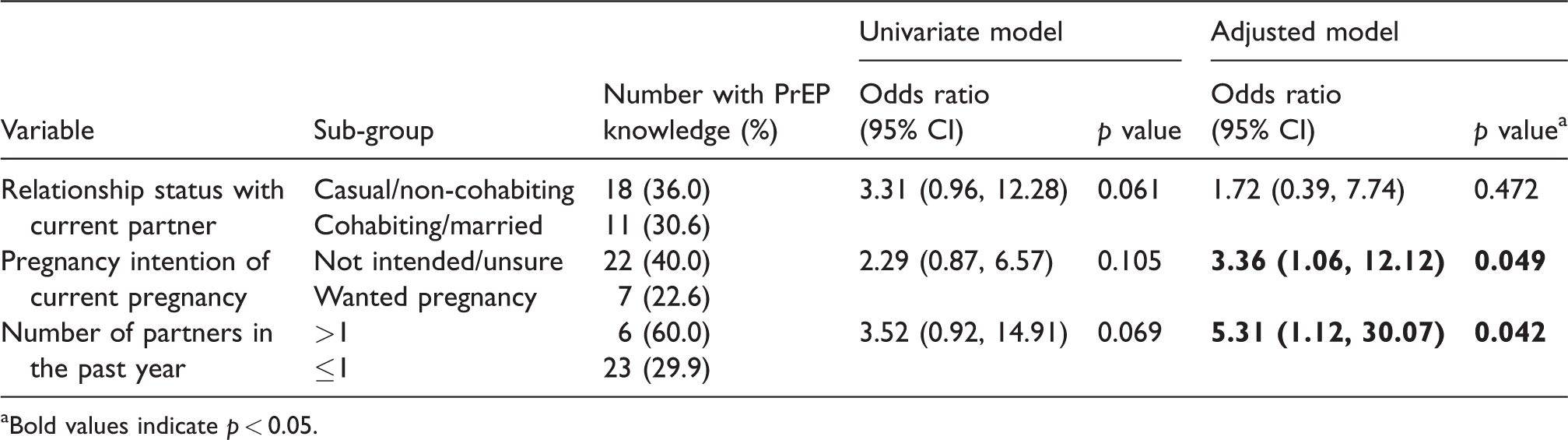
aBold values indicate p < 0.05.
Discussion
Our study identified limited knowledge about PrEP among a sample of pregnant and breastfeeding women in antenatal and postnatal care in Cape Town, where HIV prevalence in pregnant women approaches 30%.5,26 Only one-third of women had heard of PrEP before, in most cases as part of their clinical care. Knowledge was highest in older women, women who reported multiple sex partners and women who did not intend to get pregnant. Taken together, this pilot study provides a foundation for further research into PrEP education and targeting, both in terms of identifying groups among whom PrEP knowledge might be lower, as well as highlighting non-clinic sources as potentially underutilized resources for PrEP education.
Previous research into PrEP in high-prevalence areas has met with mixed success. While some studies have found that PrEP lowers HIV incidence, other studies’ evaluations of PrEP efficacy have been limited by low adherence, especially in women.21,22,29,30 PrEP is now available in public facilities in South Africa, and as it becomes increasingly used as a tool to help prevent HIV, there is increased interest in peoples’ perceptions of PrEP, as this would help develop education and counseling to maximize utilization. Researchers have identified theoretical strategies to improve awareness and decrease stigma through education.25,31,32 However, studies that focus on directly assessing PrEP awareness, particularly in heterosexual couples in high-incidence areas, are limited, even as PrEP becomes more widely available outside of research settings in South Africa. Pregnant and postpartum African women are a population at high risk of HIV acquisition and vertical transmission, yet PrEP remains unavailable to these vulnerable women in South Africa. With ample evidence supporting its safety, there is considerable interest in assessing the benefit of providing PrEP and PrEP counseling in this population.12,18,20
Our study contributes to this question by assessing PrEP awareness and knowledge in pregnant and postpartum women in Cape Town. We demonstrate that overall PrEP knowledge is low, and key socio-behavioral factors, including pregnancy intention and number of sexual partners, were associated with increased PrEP awareness. These findings are consistent with evidence linking these behaviors to increased risk of HIV,33–35 suggesting that women at risk of HIV may be more likely to seek information about PrEP, and that understanding the risk of infection strengthens the desire for information about prevention. Studies of PrEP outreach in other contexts, including for men who have sex with men and female sex workers, suggest that community outreach is valuable for increasing PrEP awareness, but that regular clinic follow-up is a significant barrier to initiating and adhering to PrEP.36–38 For pregnant and postpartum women, clinic visits are already regularly scheduled as part of pre- and perinatal care, which may serve as an ideal outlet for PrEP information but must be combined with community outreach as part of a comprehensive education approach.39,40
This study thus suggests possible future directions for PrEP outreach and implementation research. As this is a small pilot study, future studies are necessary to confirm results and further explore ideal mechanisms of PrEP education prior to implementation of particular strategies. However, our research suggests that future studies should focus on two specific areas of outreach. First, given the importance of clinics in providing PrEP education currently, research may explore strategies to integrate PrEP counseling into existing visits, such as by including a conversation of PrEP, including confirmation of understanding its purpose. Special emphasis should be placed on identifying and educating serodiscordant couples, to provide early prevention strategies, but also implementing couples HIV testing to ensure women have knowledge of their risk. 41 These strategies should be implemented at regular antenatal and postnatal visits, given the possibility of new partners over the course of the pregnancy. Additional research is needed to identify outreach strategies beyond the clinic to increase community awareness of PrEP, for example, for women who may become pregnant (intentionally or otherwise). This outreach would both reduce stigma and misinformation around this prevention strategy to increase acceptability of PrEP early in the antenatal course.
The primary limitation of this study is its small sample size of women who were interviewed about PrEP knowledge as part of a larger study on sexual risk behaviors during pregnancy. 2 Thus, this study provides a preliminary look at factors influencing PrEP knowledge within this population, but is underpowered to explore specifics of PrEP knowledge, such as the importance of adherence to the medication for efficacy, which has been identified as a major challenge of implementing PrEP among serodiscordant couples in previous studies.21,22,42 It also did not explore whether prior knowledge of PrEP affected potential (or real) willingness to take the medication. However, this small study provides important findings that highlight the many factors that influence knowledge of PrEP, which is increasingly an important tool in the effort to prevent HIV. As additional studies in PrEP are conducted, this study can help to contextualize and enrich those findings. This study was also conducted at one HIV research study site, which may have an impact on PrEP knowledge. Although this site did not provide PrEP itself, other public health facilities in the area did; thus, the population at this site lived in an area where PrEP was not solely discussed in a research context. Additionally, while there are limited other studies on PrEP awareness among this population, these results are consistent with overall low rates in the population as a whole, and consistent with higher awareness noted in populations at higher risk of HIV infection.43,44 As PrEP research and overall utilization increases, future studies should explore awareness and education across multiple clinic contexts, including specifically in studies of pregnant and postpartum women.
Conclusion
PrEP has increasingly been recognized as a valuable tool to prevent HIV transmission, starting in highly vulnerable populations such as men who have sex with men, but increasingly in serodiscordant heterosexual couples in high-prevalence areas.16,29,30 PrEP also has substantial potential benefits for pregnant and postpartum women given its safety in this group, and PrEP acceptability studies in pregnant women are ongoing.18,20,45,46 This pilot study is among the first to offer an analysis of factors associated with PrEP knowledge in pregnant and postpartum women. We show that socio-behavioral factors including pregnancy intention and number of partners are associated with increased knowledge, and that clinics remain the most common source of PrEP knowledge. Our results suggest areas for future research, including strategies to integrate PrEP counseling across the antenatal and postpartum care periods to account for continued risk of HIV infection; and the need for further exploration of community-based education and outreach around PrEP in couples seeking to conceive, serodiscordant couples and pregnant women. As PrEP becomes more widespread and reaches a broader audience, studies like this one that focus on education and outreach will be crucial to ensure effective uptake and utilization of this key HIV prevention strategy.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: funding for this study was provided by NIMH (R01MH116771). Dr. Joseph Davey received funding support from Fogarty International Center (K01TW011187).