
Abstract
A 27-year-old Peruvian woman living with human immunodeficiency virus (HIV) in clinical stage B3 and not on antiretroviral therapy presented with a ten-day history of fever, chills, night sweats and a two-day history of skin lesions. On physical examination, several erythematous-purplish lesions were found on the face and legs. Meningococcal infection was suspected and ceftriaxone was started. Blood culture grew nontyphoidal Salmonella enterica. A biopsy of the skin lesions showed leukocytoclastic vasculitis (LCV); therefore, corticosteroids were added. After two weeks of antibiotic and corticosteroid treatment, the lesions had resolved, but they recurred two days after treatment with prednisone was stopped. Corticosteroids and combination antiretroviral therapy were started simultaneously and the lesions resolved without recurrence. HIV infection has been associated with higher rates of skin lesions in salmonellosis. LCV has been described both in the setting of HIV infection and salmonellosis. However, our review of the literature found no previous cases of LCV in concurrent HIV and salmonellosis.
Keywords
Introduction
Leukocytoclastic vasculitis (LCV) is a histopathological term used to describe a small-vessel vasculitis of the skin. Its physiopathology results in the formation of immune complex deposition in the affected vessels of the skin secondary to infectious, pharmacologic, malignant, collagen vascular disease or idiopathic antigen stimuli.1,2 In this case report, we present nontyphoidal Salmonella bacteremia-associated LCV in the context of advanced untreated human immunodeficiency virus (HIV) infection.
Case report
A 27-year-old woman from Lima, Peru living with treatment-naïve human immunodeficiency virus (HIV) infection in clinical stage 3 according to the World Health Organization classification (CD4+ T lymphocyte cell count: 1 cell/µl; viral load: 61,496 copies/ml), with no antiretroviral therapy, was admitted for evaluation of a ten-day history of fever, chills and night sweats. Two days before admission, she developed purplish-red, painful, symmetric lesions on her thighs, knees, buttocks, nose and auricles. Her medical record was relevant for a history of successfully-treated pulmonary tuberculosis five years prior to the current admission.
Physical examination revealed an acutely ill, febrile (102°F), hypotensive (blood pressure: 80/50 mmHg), tachycardiac (116 bpm) patient, with 96% oxygen saturation. Multiple 10 × 5 cm erythematous-purplish lesions were found on the thighs, knees and buttocks. Smaller 2–3 cm lesions were found on her auricles and nose (Figure 1). Multiple small, superficial, nontender lymph nodes were palpable on her neck and groin. There were no further positive findings. Her analytical results showed: hemoglobin: 8.2 g/dl (normal range [nr]: 11.6–15 g/dl); leucocyte count: 1320 cells/ml (nr: 4500–11,500 cells/ml) (segmented: 83%, bands: 2%, lymphocytes: 8%, monocytes: 4%, eosinophils: 3%), platelets: 68,000 (nr: 150,000–450,000), C-reactive protein: 304 mg/dl (nr < 10 mg/dl), erythrocyte sedimentation rate: 90 mm/h (nr < 20 mm/h), normal liver enzymes electrolytes and total calcium.
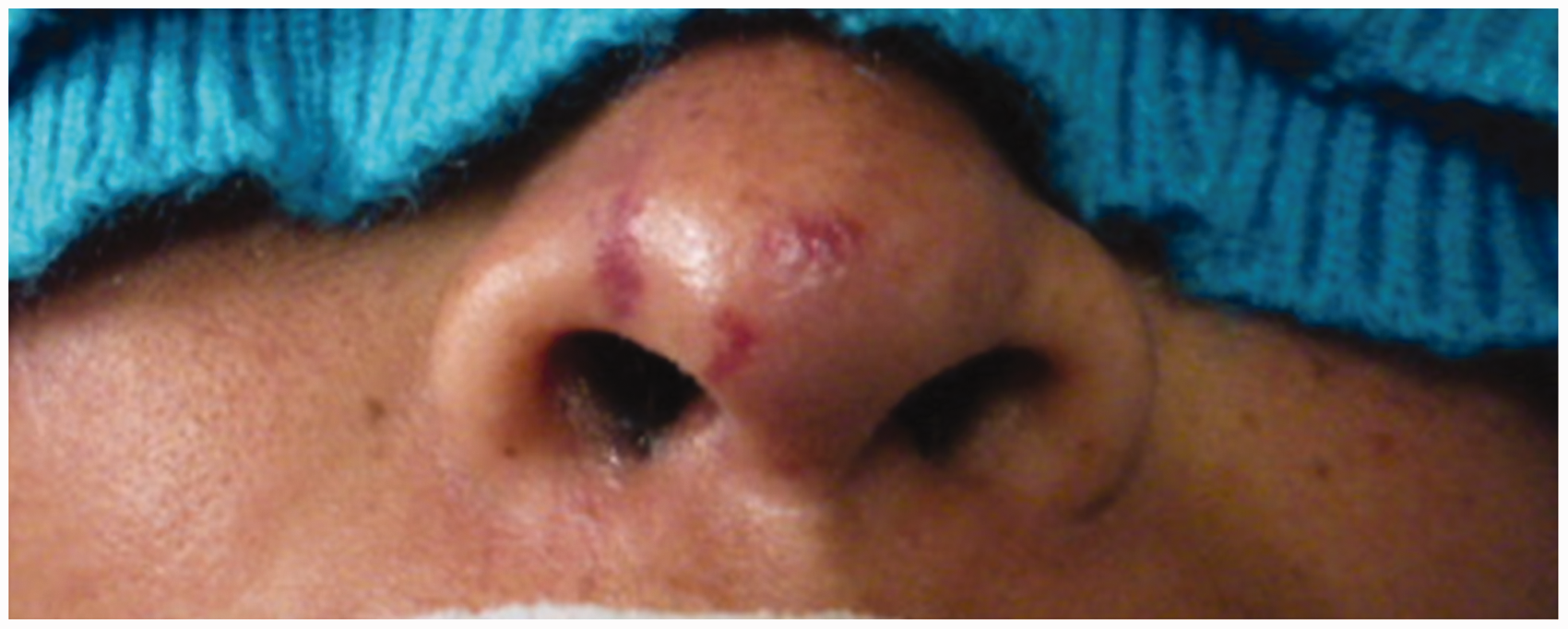
Erythematous-purplish lesions on the patient’s nose upon admission.
The presumptive diagnosis of meningococcemia or streptococcemia was proposed; blood cultures and a lumbar puncture were performed; and the patient was started on empiric ceftriaxone (2 g bid IV). Cerebrospinal fluid exam showed hypoglycorrachia: 38 mg/dl (nr: 40–80 mg/dl) with simultaneous serum glucose: 99 mg/dl; no pleocytosis: 2 cells/µl (nr: 0–5 cells/µl), no hyper proteinorrachia: 42 mg/dl (nr: 15–60 mg/dl) and negative cultures. Blood cultures grew nontyphoidal Salmonella enterica with intermediate susceptibility to nalidixic acid and fully susceptible to ciprofloxacin, chloramphenicol, cefotaxime and cotrimoxazole. Antibiotic therapy was therefore shifted to high dose ciprofloxacin (400 mg tid IV). Other etiologies for LCV were investigated for which the patient tested negative, including infections (hepatitis B, hepatitis C, syphilis, human T cell lymphotropic virus, urine culture, herpes simplex virus 1–2, cytomegalovirus, toxoplasmosis, yellow fever, dengue fever, leptospirosis, rickettsiosis), neoplastic (CA125 and alpha-1-fetoprotein) and rheumatologic disorders.
A bone marrow aspiration showed increased cellularity, low hemosiderin, reactive plasmacytosis and reactive phagocytosis, compatible with a current infection. Finally, a skin biopsy of the lesions was performed, and the diagnosis of LCV was established. Corticosteroids were then added to the patient’s management.
During her hospital stay, the central areas in the patient’s lesions turned into necrotic ulcers (Figure 2); and after two weeks of antimicrobial and corticosteroid therapy, the lesions had resolved. There was remission of facial lesions and healing in other locations. Two days after removing the corticosteroids, lesions on her nose, right ear and toes recurred. She was re-started on corticosteroids and combination antiretroviral therapy (cART) consisting of tenofovir disoproxil fumarate (TDF) + lamivudine (3TC) + efavirenz (EFV), which led to remission of the new lesions.

Central necrotic ulcers on the patient’s inner thigh.
The patient was discharged due to her favorable course with physiologic doses of prednisone for three months, until her CD4+ cell count was >200 cells/µl. After six years of follow up there has been no relapse.
Discussion
Cutaneous lesions in salmonellosis is an infrequent sign, described in only 1–10% of cases. Rose spots, erythematous, blanching, maculopapular lesions measuring 2–4 mm are the most common presentation.3,4 HIV infection has been associated with increased risk of bacteremia and skin lesions in salmonellosis. 5 Our review of the literature found no case reports of patients with LCV associated with Salmonella bacteremia in an HIV-infected patient.
LCV is a small-vessel vasculitis of the skin. 6 Its physiopathology involves immune complex deposition in small vessel walls. This leads to the activation of the complement system and recruitment of neutrophils, which results in vessel wall damage and formation of a perivascular exudate.7,8 Infectious causes of LCV include nontuberculous mycobacteria, Salmonella paratyphi, streptococci, 9 hepatitis B, hepatitis C 10 and syphilis. 11 Amongst pharmacologic causes are warfarin, 12 erlotinib 13 and rifamycin. 14 While LCV has also been associated with neoplasia, hematologic disorders and connective tissue diseases, the most common aetiology remains idiopathic. 8
LCV usually manifests as erythematous macules with palpable purpura bilaterally. The lesions may be asymptomatic, painful or itchy. Extracutaneous manifestations include systemic nonspecific symptoms such as low-grade fever, malaise, myalgia and arthralgia. 8 These symptoms are compatible with the findings in our patient.
Previous reports of Salmonella-associated LCV include patients with Mendelian susceptibility to mycobacterial disease (MSMD), a rare congenital immunodeficiency in the interleukin 12/interferon gamma pathway.15–17 Patients with this condition show predisposition to recurrent infections by usually nonvirulent pathogens such as environmental nontuberculous mycobacteria, nontyphoidal Salmonella and certain Candida species. It is commonly caused by mutations in the IL12RB1 gene, which encodes the β1 chain of interleukin 12 receptor. 18 Unfortunately, resources are not available to know whether our patient had this particular syndrome.
LCV reports in HIV infection are rare and usually describe patients in early stages of the infection, unlike our patient. The most common location is skin vessels, but it has also been described in the vasa vasorum of larger vessels. Previously, LCV in HIV infection has been treated with non-steroidal anti-inflammatory drugs, topical corticosteroids, antihistamines and cART.19–21
Because there are no guidelines on the recommended duration of corticosteroid therapy in the setting of LCV, our steroid therapy was empiric and based on the clinical response, including the relapses of the patient. Finally, we suggest that cART therapy in association with corticosteroids controlled this rare immune phenomenon in the patient. Immune recovery, thanks to the virological control obtained by cART, made possible the gradual tapering of the corticosteroids without recurrence of the lesions.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.