
Abstract
Women who have a prevention mindset may opt for concurrent use of oral pre-exposure prophylaxis (PrEP) and all forms of contraception; we therefore assessed how contraception may influence PrEP use or vice versa. We analyzed data from Kenyan and Ugandan HIV-uninfected non-pregnant women in sero-discordant partnerships who were participating in the Partners Demonstration Project. Using multivariable generalized estimating equation models, we estimated the associations between effective contraceptive use and 1) PrEP dispensation 2) high effective PrEP use. Among the 311 women (93.1% of all those followed in the Partners Demonstration Project) median age was 29 years (interquartile range [IQR] 24.0–35.0) and 115 (37.0%) reported using effective contraception at baseline. All the women initiated PrEP during the study and moderately high PrEP adherence was recorded at 73.1% of visits over an average 7.5 months following PrEP dispensation. Women (14.8%) consistently used an effective contraceptive throughout study follow-up. PrEP dispensation was more frequent among those concurrently using effective contraception, (adjusted relative risk [aRR] = 1.19; 95% confidence interval [CI] = 1.08–1.32) and contraceptive use was more common among those on PrEP (aRR = 1.63; 95% CI = 1.18–2.25). Among East African women at high risk of HIV infection, PrEP dispensation was more frequent among women using effective contraception, indicating that family planning outlets may be efficient locations to deliver PrEP.
Introduction
High rates of unintended pregnancy are often reported in sub-Saharan Africa, resulting partially from a high unmet need for contraception.1–5 In Kenya, for example, 39% of sexually active unmarried women are not using modern contraceptive methods, and 40% of pregnancies are estimated to be mistimed or unwanted. 6 In parallel, many regions in sub-Saharan Africa with high rates of unintended pregnancies also experience high prevalence of HIV, especially among young women. 7 , 8 Therefore, many women face concurrent risks for unintended pregnancy, HIV, and STIs and need options for prevention that are easily accessible, convenient, and can be used concurrently.
Multiple studies have reported that the integration of family planning (FP) services into HIV clinics has successfully led to increased use of contraceptives and significant reductions in the occurrence of unintended pregnancy among women living with HIV.9–13 Additionally, daily oral pre-exposure prophylaxis (PrEP) is being integrated into existing reproductive health services (e.g. FP, antenatal, and postpartum clinics). 14 , 15 This integration eliminates the need to provide separate referrals for either FP services or PrEP, removing a structural barrier to their uptake, 15 and has potential for decreased stigma (e.g., if PrEP is delivered in FP clinics). However, it is unclear whether use of contraception shows an inclination to a prevention mindset, hence contraception users are more likely to use PrEP. Alternatively, PrEP initiation may reduce the use of contraception among women due to increased pill burden, side effects, or other reasons. Here, we report findings from analyses of effective contraception use on PrEP dispensation and PrEP adherence and vice versa over time among HIV-uninfected women in East Africa.
Methods
Study population
The Partners Demonstration Project (clinicaltrials.gov #NCT02775929) followed 334 high risk HIV-negative women in stable relationships with male partners living with HIV at four research clinics in Thika and Kisumu, Kenya and Kampala and Kabwohe, Uganda, between November 2012 and June 2016. The primary aim of this open-label implementation study was to evaluate PrEP uptake, adherence, and discontinuation when PrEP delivery was integrated into an antiretroviral therapy (ART) program and targeted to HIV-uninfected members of HIV serodiscordant couples. 16 , 17 The study clinics also provided effective contraceptive methods on-site (for injectables and oral contraceptive pills [OCP]) or by referral (for intrauterine devices [IUDs] and implants), if desired. The eligibility criteria included being ≥18 years, planning to remain as a couple at least one year, and no prior use of PrEP or ART within the couple. Additionally, a validated risk score was applied to select couples with high HIV risk based on characteristics associated with HIV incidence rates of >3–4% per year. This risk score was developed from empirical data using standard prediction modeling methods and composed of key predictors for HIV risk, specifically; age of the HIV uninfected partner, married/cohabiting partnership, number of children, unprotected sex, uncircumcised male HIV-uninfected partner, and plasma HIV viral load in the HIV-infected partner with a maximum risk score of 12. 18 , 19
Data collection procedures
HIV-uninfected women attended study visits on a quarterly basis for up to 24 months, were encouraged to come for visits with their male partners living with HIV, and were provided with both PrEP and effective contraception free-of- charge, based on their preferences and pregnancy plans. We used standardized interviewer-administered questionnaires to collect self-reported data on socio-demographics, sexual behavior, fertility desires, and contraceptive use information at each study visit. Data on effective contraceptive use were verified in clinic chart notes if the contraceptive was provided on-site. We defined implants, IUD, surgical methods, OCP, and injectables as effective contraceptive methods. PrEP dispensation was defined as not having discontinued PrEP since the prior visit. Participants were considered to be off PrEP if they refused PrEP or missed a study visit when they would otherwise receive PrEP. Data on PrEP dispensing were captured through pharmacy refills and daily usage data were captured by a medication event monitoring system (MEMS) pill bottle cap that recorded a date-time stamp every time the PrEP bottle was opened and closed. 20 MEMS data were downloaded by the study pharmacist during clinic visits.
In this delivery model of PrEP within HIV-serodiscordant couples, PrEP discontinuation was encouraged when partners living with HIV sustained ART use for ≥6 months, when viral suppression would be expected, and if there were no concerns about ART adherence, the HIV status of additional partners, or plans to become pregnant.
Statistical analyses
Our analysis focused on the subset of participants who were not pregnant or immediately desiring pregnancy at baseline (N = 311 women). We conducted descriptive analyses to summarize participant characteristics, the frequency of different contraceptive types at each study visit, and contraceptive switching during study follow-up. If participants missed a study visit, they were assumed to have remained on their last reported contraceptive method and to have discontinued PrEP since PrEP was not available outside of the study clinic during the time when the study was conducted while contraception was otherwise available in the study vicinities. Observations were censored after PrEP was permanently discontinued by participant preference or study end. MEMS data were used to define effective PrEP adherence when ≥80% of expected MEMS openings were recorded since the prior study visit, indicating an average of ≥5 doses per week were taken.
We used multiple generalized estimating equations (GEE) to examine PrEP dispensation in relation to contraceptive use, as well as whether use of contraception influenced PrEP uptake and use. In the first set of models, we defined our exposure as PrEP dispensation since the prior visit, and we define our outcome in three ways: any effective contraceptive use (IUD, implants, surgical methods, oral pills, or injectable), long-acting effective contraceptive use (IUD, implants, and surgical methods), or non-long-acting methods (oral pills, injectable) because we hypothesized that those on long-acting contraceptive methods could have a different prevention mindset than those on non-long-acting methods. In our second set of models, we defined our exposure as effective PrEP use (at least 80% of expected bottle openings) and the outcomes remained the same as in the first analysis. In a third set of models, we used GEE to examine the reverse relationship, with effective contraceptive use as the exposure of interest and PrEP dispensation and adherence as the outcomes.
All GEE models were fit with a log link to estimate relative risks. We included age as a covariate in our models a priori, based on the known associations between age and PrEP dispensation and effective contraceptive use.21–23 We also assessed several additional covariates for confounding including education, income, marital status, partnership duration, time known to be in an HIV serodiscordant relationship, and number of children with study partner (all measured at enrollment), as well as time-dependent measures of sexual behavior (number of sex acts, proportion of unprotected sex acts, number of partners), timing of next desired pregnancy (within the next three years, more than three years from now, don’t know), STI symptoms, intimate partner violence, and ART use of the partner living with HIV. Of these covariates, any that resulted in a substantial change in the relative risk estimate (>10%) in univariate analysis were included in the multivariable models. We included the maximum set of covariates in all models to facilitate the comparison of point estimates.
Ethical statement
Study protocols were approved by ethical review boards at the University of Washington and collaborating institutions in Kenya and Uganda. All participants provided written informed consent in their preferred language.
Results
Participant characteristics
Of the 311 HIV-uninfected women in this analysis (93.1% of all those followed in the Partners Demonstration Project), the median age was 29.0 years (interquartile range [IQR] 24.0–35.0). Women using and not using effective contraception had a median of 2 children (IQR 1.0–3.0) and 1 child (IQR 0.0–2.0), respectively (Table 1). Notably, 178 (57.2%) women reported at least one condomless sex act with their partner in the month prior to enrollment. The mean follow-up time was 20.8 months while mean time using PrEP was 7.5 months. The total number of visits included in this analysis was 1895.
Participant characteristics at enrollment, by effective contraceptive use (N = 311 unless otherwise indicated).
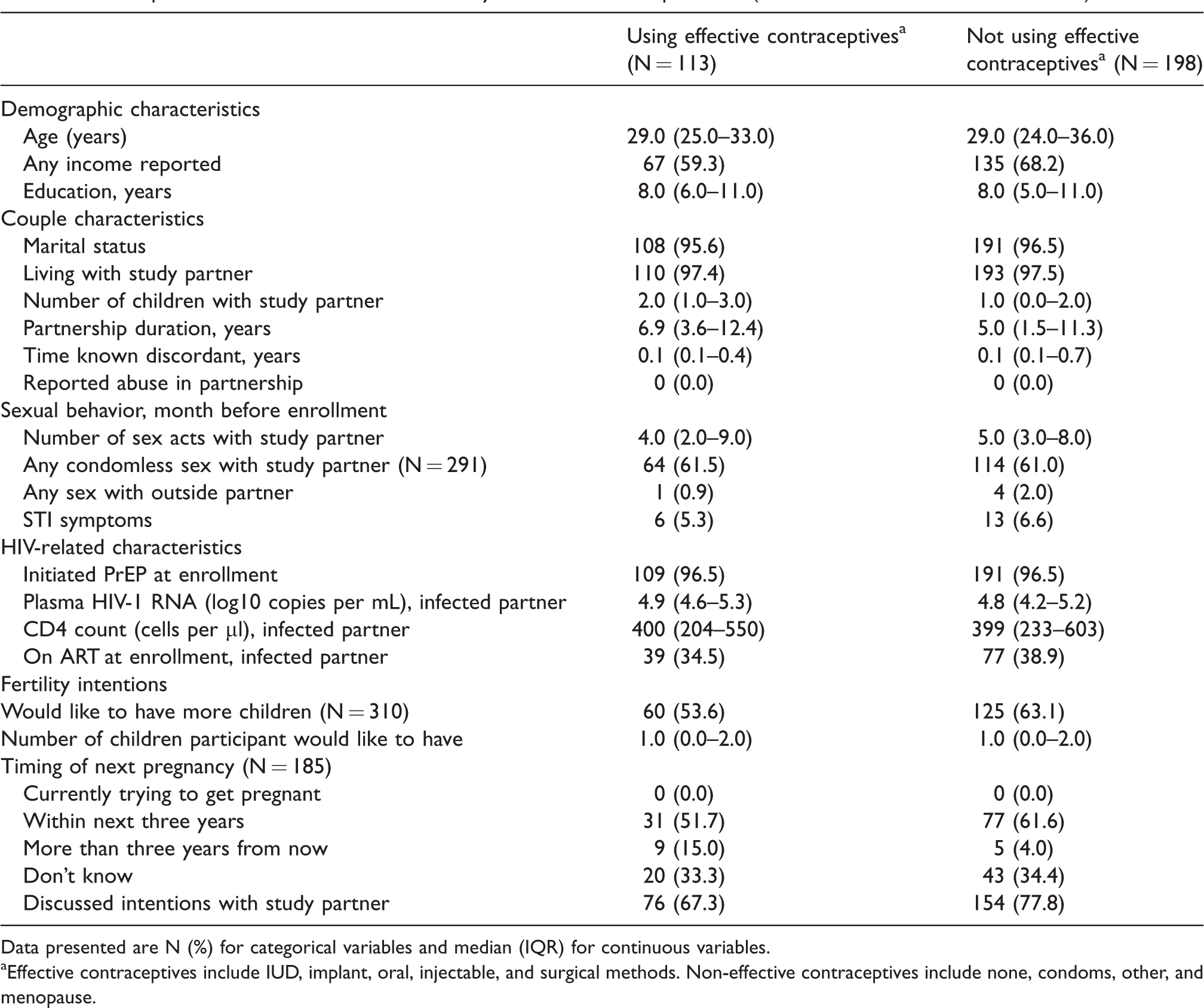
Data presented are N (%) for categorical variables and median (IQR) for continuous variables.
Effective contraceptives include IUD, implant, oral, injectable, and surgical methods. Non-effective contraceptives include none, condoms, other, and menopause.
PrEP use during study follow-up
All women initiated PrEP during the study and 92.9% of 311 (N = 289) HIV-uninfected women included in this analysis used PrEP until their partner living with HIV was using ART. Among all 311 HIV-uninfected women, 64.0% (N = 199) used PrEP for exactly 6 months following ART initiation by their partner. Among the 289 women who used PrEP until their partner was using ART, 25.6% (n = 74) continued PrEP use for >6 months following ART. This was due to primarily immediate fertility desires or current pregnancy (47.3% [35/74]), a desire for longer ART use by the partner living with HIV (39.2% [29/74]), or lack of documented viral suppression in partner living with HIV (13.5% [10/74]). MEMS data on PrEP pill bottle openings indicated that PrEP adherence was high among participants who had been dispensed PrEP at a prior study visit. Specifically, 72.2% of 1042 visits with available MEMS data had ≥80% of expected doses taken since the prior visit and 83.8% had ≥50% taken. These MEMS results aligned with pharmacologic measures of PrEP adherence. Tenofovir (TFV) was detected in 77.2% of samples among 122 participants randomly selected for TFV quantification at 422 visits following PrEP dispensation. Pharmacy pill counts yielded similar information and 87.1% and 95.4% of bottles had ≥80% and ≥50% of expected doses taken, respectively.
Contraceptive use during study follow-up
At baseline, 63.0% (n = 196) of women did not report using any effective contraceptive method, 15.1% (n = 47) were using injectables, 11.9% (n = 37) implants, 5.1% (n = 16) oral contraceptives, 2.6% (n = 8) surgical methods, and 2.3% (n = 7) IUD. The contraceptive method mix remained steady during the 24-month study follow-up (Figure 1). Approximately 14.8% of women (n = 46) used an effective contraceptive at all visits and almost half (45.7%; n = 142) never used an effective method. At enrollment, 27 women (8.7%) were not using effective contraception but initiated effective contraception use during follow-up and remained on effective contraception for the remainder of their follow-up period. 41 women (13.2%) were using an effective contraceptive method at enrollment but then discontinued the method at a subsequent follow-up visit and remained off an effective method permanently through study end (Figure 2). An additional 55 women (17.7%) reported switching on and off effective contraceptive methods throughout study follow-up (e.g., were not using an effective contraceptive method at enrollment, began using an effective method at one study visit, discontinued method use at their nine-month study visit, and resumed method use at their 12-month study visit). Participants who never used an effective method reported desiring children within the next three years at 19.0% of 1313 follow-up visits and reported wanting at least one more child during 56.8% of these visits. Participants who always used an effective method reported desiring children in the next three years at 13.7% of 395 follow-up visits and reported wanting at least one more child during 35.1% of these visits.

Contraceptive method mix among HIV-negative women in an open-label PrEP demonstration project.a
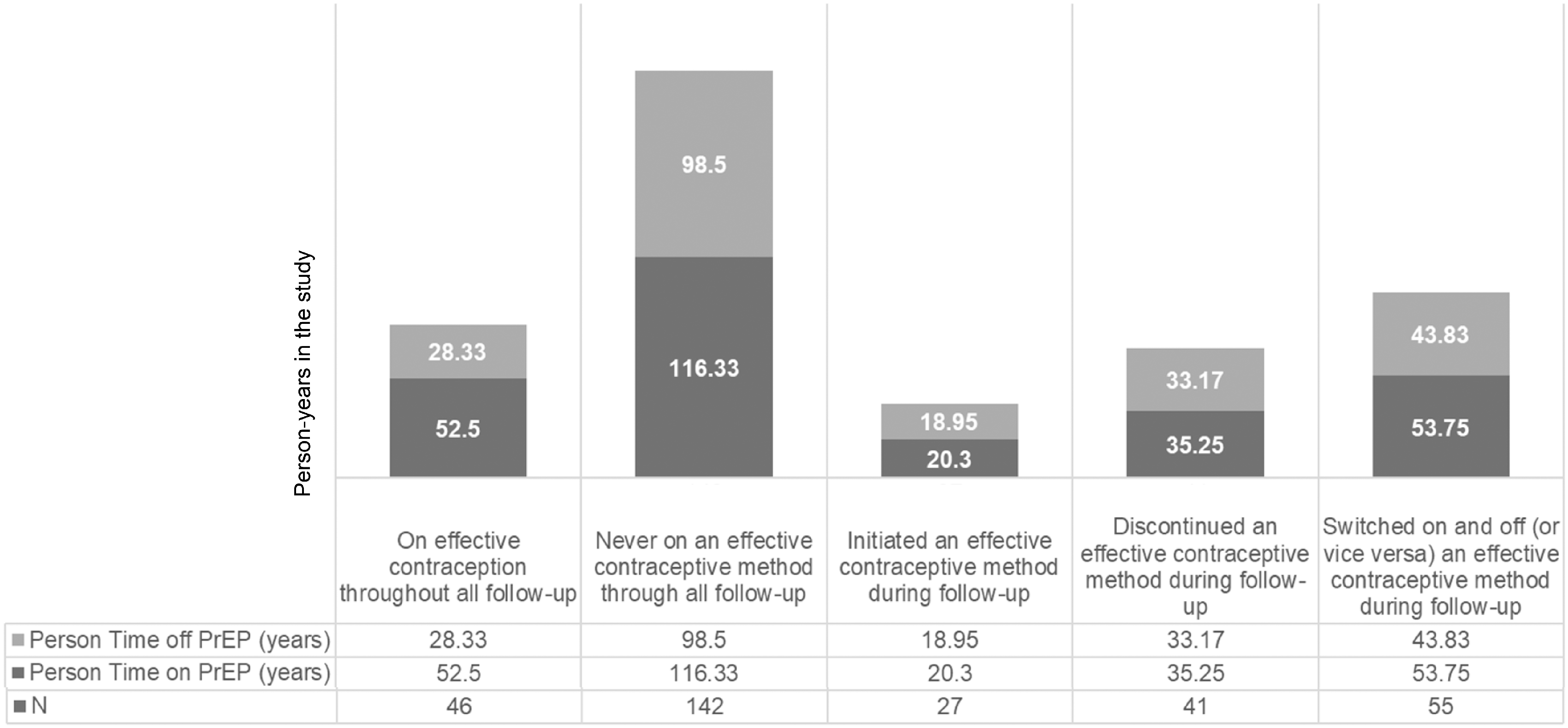
Contraceptive switching throughout study follow-up visits.a
The influence of PrEP on effective contraceptive use
Effective contraception was more frequently used during periods when PrEP was dispensed (38.9% of periods) relative to periods when PrEP was not dispensed (29.7% of periods, adjusted relative risk [aRR] 1.63, 95% CI 1.18–2.25). When disaggregating by type of effective contraceptive use, this association was driven by use of long-acting contraceptive methods (aRR 2.84, 95% CI 1.54–5.25) and there was no association between PrEP dispensation and use of injectable and oral contraceptives (Table 2). Effective contraception was used with similar frequency during periods when PrEP was used with high or low adherence (aRR 0.99, 95% CI 0.77–1.28, Table 2), and these results were consistent among women using long-acting and other effective methods.
Longitudinal analysis to examine the alignment between PrEP use (exposure) and effective contraceptive use (outcome).

Models adjusted for site, age at enrolment, timing of next pregnancy (within the next three years, more than three years from now, don’t know), ART use of the partner living with HIV, and number of times a condom was used with a study partner. There was <10% missingness for all analyses.
PrEP dispensation was defined as not having discontinued PrEP since the prior visit. Participants were considered to be off PrEP if they refused PrEP or missed a study visit when they would otherwise receive PrEP. Observations were censored after the protocol-defined PrEP stop (average length of follow-up in sample was 7.5 months).
Effective contraceptive methods include implant, IUD, injectable, oral, or surgical methods.
Long-acting methods include implants, IUD, and surgical methods.
Compared with the null outcome model, no effective contraceptive use (e.g., no contraceptive use reported, condoms only).
Non-long-acting methods includes injectables and oral contraceptives.
Effective PrEP use defined as >=80% of expected MEMS cap openings since the prior visit.
The influence of effective contraceptives on PrEP use
PrEP was more likely to be dispensed during visits with concurrent report of effective contraceptive use (76.2% of visits) compared to visits without use of effective contraception (68.1%, aRR = 1.19, 95% CI = 1.08–1.32, Table 3). After disaggregating by type of effective contraceptive use, this association was present only among women using long-acting methods (aRR = 1.34, 95% CI = 1.19–1.51, p-value <0.001, Table 3). PrEP adherence was similar when effective contraception was used as when it was not (73.3% versus 73.0%, aRR = 1.02, 95% CI = 0.73–1.41, Table 3), and we also did not detect a difference in PrEP adherence by effective contraceptive type.
Longitudinal analysis to examine the alignment between effective contraceptive use (exposure) and PrEP use (outcome).
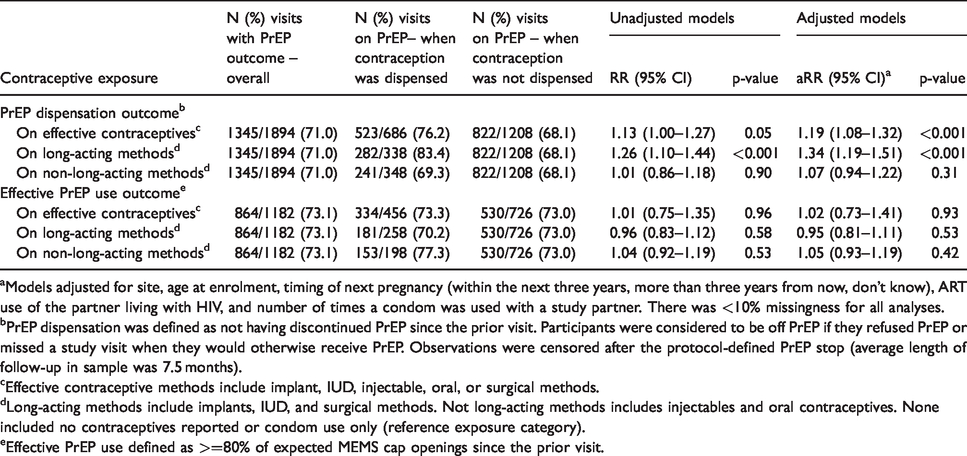
Models adjusted for site, age at enrolment, timing of next pregnancy (within the next three years, more than three years from now, don’t know), ART use of the partner living with HIV, and number of times a condom was used with a study partner. There was <10% missingness for all analyses.
PrEP dispensation was defined as not having discontinued PrEP since the prior visit. Participants were considered to be off PrEP if they refused PrEP or missed a study visit when they would otherwise receive PrEP. Observations were censored after the protocol-defined PrEP stop (average length of follow-up in sample was 7.5 months).
Effective contraceptive methods include implant, IUD, injectable, oral, or surgical methods.
Long-acting methods include implants, IUD, and surgical methods. Not long-acting methods includes injectables and oral contraceptives. None included no contraceptives reported or condom use only (reference exposure category).
Effective PrEP use defined as >=80% of expected MEMS cap openings since the prior visit.
Discussion
Women in our study were more likely to use oral PrEP when they were concurrently using long-acting contraceptives and any effective contraception was used more frequently when PrEP was being dispensed relative to periods off PrEP. This finding signals that healthcare delivery models that integrate provision of family planning and PrEP may successfully promote both preventive products, especially long-acting contraception. A recent study of integration of PrEP into FP clinics in Kenya reported a 21.7% uptake of PrEP among FP users. 15 We therefore need to learn more about these populations to assess full potential for integrated delivery. Additionally, our data suggest that some combined benefit exists for the use of the two products concurrently, and if they can be combined into one multi-purpose prevention technology (MPT), there is great potential to address unmet need for contraception and HIV prevention.
While PrEP dispensing aligned with contraceptive use, PrEP adherence did not appear to significantly influence effective contraceptive use among women in our study and contraception did not influence PrEP adherence. This finding suggests that PrEP and contraception can be used at the same time and neither may influence continuation of the other (i.e., once on PrEP its adherence is unlikely to be influenced by contraception and vice versa). One possible explanation for this finding is that the women in our study could have perceived themselves at risk of both HIV and pregnancy and were likely to use both PrEP and contraceptives independently. Promoting long-acting contraceptive use to a target population that is not looking to conceive in the short-term may contribute to fostering a preventive mindset that supports PrEP use too which will become even more pertinent when PrEP becomes available in long-acting formulations as opposed to daily pills.
In our cohort of women at high risk of HIV, 19 we found a high unmet need for contraception. Contraceptive discontinuation was common and only 14.8% remained on effective contraception throughout the 24-month study duration and an even smaller proportion of these women used longer acting methods despite reporting consistently that they desired pregnancy in 3 years or more. These data demonstrate high unmet need for contraception, as many other studies have shown.1–5 Additionally, some studies have reported that integration of FP into HIV treatment and care has not always led to increased use of contraception especially in regions where contraceptive use is low necessitating a need to address individual and community perspectives and barriers which could hinder uptake. 12
Study limitations
To our knowledge this is the first study to measure the relationship between the use of PrEP (both dispensation and adherence) and effective contraception prospectively among women at high risk of HIV infection. Our study focused on women at high risk of HIV acquisition in sero-discordant relationships and therefore our findings may not be generalizable to other women in transient relationships or with partners of unknown HIV status. Contraceptive use and fertility desires were measured by self-report every three months which could be subject to recall and social desirability biases. Additionally, there are marked measurement issues in ascertaining fertility desires and our tool may not have accurately captured this complex concept. Additionally, residual confounding by mismeasured sexual behavior data could influence our models of effective contraceptive use and PrEP use and potential misclassification of adherence if MEMS were misused (i.e. no pills ingested with an opening or multiple pill removed with a single opening). 24 , 25
Conclusion
For women at high risk of both unintended pregnancy and HIV, concurrent use of an effective contraception and daily oral pre-exposure prophylaxis (PrEP) are recommended strategies. Our results suggest that MPTs would be useful to women concurrently preventing pregnancy and HIV and that combining products would be desirable and may improve uptake and continued use of both PrEP and effective contraceptives. Future MPT acceptability studies are needed to explore the success/failure that women would have switching from the MPT to a PrEP-only product when women desire pregnancy. In summary, in this large prospective analysis of data from African women at high risk of HIV infection we found that PrEP and contraceptive use were effectively used concurrently. Programs focused on scaling up PrEP delivery can use the opportunity to integrate the provision of effective contraception when pregnancy is undesired and existing family planning programs can also be encouraged to integrate PrEP into their services.
Footnotes
Acknowledgements
The authors thank the couples who participated in the study and the teams at the four study sites and the University of Washington that supported data collection and management for this work. Partners Demonstration Project Team
Coordinating Center (University of Washington) and collaborating investigators (Harvard Medical School, Johns Hopkins University, Massachusetts General Hospital):
Jared Baeten (protocol chair), Connie Celum (protocol co-chair), Renee Heffron (project director), Deborah Donnell (statistician), Ruanne Barnabas, Jessica Haberer, Harald Haugen, Craig Hendrix, Lara Kidoguchi, Mark Marzinke, Susan Morrison, Jennifer Morton, Norma Ware, Monique Wyatt.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Partners Demonstration Project was funded by the National Institute of Mental Health of the US National Institutes of Health (grant R01 MH095507), the Bill & Melinda Gates Foundation (grant OPP1056051), and through the US Agency for International Development (cooperative agreement AID-OAA-A-12-00023). JV was supported by (F31 MH113420) and RH was supported by the Eunice K. Shriver National Institute for Child Health and Human Development (R00HD076679). Additional institutional support was provided by the UW/Fred Hutch Center for AIDS Research (grant P30A1027757). Dr. Patel was supported by the NIH National Institute of Allergy and Infectious Diseases (K23AI120855). Gilead Sciences donated the PrEP medication but had no role in data collection or analysis. The results and interpretation presented here do not necessarily reflect the views of the study funders.
Project sites
Kabwohe, Uganda (Kabwohe Clinical Research Centre): Stephen Asiimwe, Edna Tindimwebwa
Kampala, Uganda (Makerere University): Elly Katabira, Nulu Bulya
Kisumu, Kenya (Kenya Medical Research Institute): Elizabeth Bukusi, Josephine Odoyo
Thika, Kenya (Kenya Medical Research Institute, University of Washington): Nelly Rwamba Mugo, Kenneth Ngure
Data Management was provided by DF/Net Research, Inc. (Seattle, WA). PrEP medication was donated by Gilead Sciences.