
Abstract
Background: Sexually transmitted infections (STIs) can be transmitted from mother to neonate. We determined the frequency of mother-to-child transmission (MTCT) of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis to the newborn nasopharynx. Methods: This study was nested in a cohort study of etiologic testing versus syndromic management for STIs among pregnant women living with human immunodeficiency virus in South Africa. Mothers were tested for STIs using the GeneXpert platform within 60 days after delivery. Nasopharyngeal swabs were obtained from newborns of mothers with a positive STI test; these were then tested by Xpert® on the same day based on the maternal STI diagnosis. Results. We tested nasopharyngeal swabs from 85 STI-exposed newborns; 74 (87%) were tested within 2 weeks after birth (median five; range 2–12 days). MTCT frequency of any STI was 30/74 (41%); 43% (23/53) for C. trachomatis, 29% (2/7) for N. gonorrhoeae, and 24% (6/25) for T. vaginalis. Also, 4/11 (36%) swabs obtained between 14 and 60 days after delivery tested positive for STI. Conclusions: There was a high frequency of MTCT of STIs to the nasopharynx of newborns in our setting. The impact of nasopharyngeal colonization and the benefits of STI testing on newborn health remain to be determined.
Keywords
Introduction
There is a high burden of sexually transmitted infections (STIs) among pregnant women in sub-Saharan Africa, where syndromic management is the mainstay of STI control. Recent studies have reported a combined prevalence of Chlamydia trachomatis, Neisseria gonorrhoeae, or Trichomonas vaginalis infection of 32–48% in pregnant women in South Africa, 35% (including syphilis) in Zambia, 21% in Kenya, 18% in the Democratic Republic of Congo, and 14% in Botswana.1–7 These STIs have been associated with adverse pregnancy outcomes including preterm birth, low birth weight, stillbirth, and neonatal mortality.8–10 Also, untreated STIs have been reported to increase the risk of mother-to-child transmission (MTCT) of human immunodeficiency virus (HIV) in the absence of antiretroviral therapy. 11
Neonates are exposed to C. trachomatis, N. gonorrhoeae, and T. vaginalis around the time of delivery in the uterus and when passing through the birth canal. Newborn acquisition of these STIs may result in asymptomatic colonization of the conjunctiva, respiratory tract, or genitals; this may be self-limiting or progress to cause infection with disease.12–14 The most common clinical presentations of C. trachomatis and N. gonorrhoeae in newborns are conjunctivitis, lower respiratory tract infection and pneumonia, genital infection, and systemic gonococcal infection and/or meningitis. 14 T. vaginalis infection appears to have a similar clinical spectrum, but data are limited to case series. 15
Most studies of MTCT of C. trachomatis and N. gonorrhoeae were conducted in the 1980s and 1990s using microbial culture. Those diagnostic methods are less sensitive than the currently used nucleic acid amplification tests (NAATs) and may have resulted in an underestimation of the frequency of MTCT. A prospective cohort study by Schachter et al. 16 reported positive C. trachomatis cultures from the eye (23%), throat (15%), rectum (17%), and vagina (5%) among 131 exposed newborns in the United States in the 1980s. Among those exposed newborns, 18% developed C. trachomatis inclusion conjunctivitis and 16% developed pneumonia; all rectal and vaginal infections were subclinical. A 6-month prospective cohort study from Kenya in 1984 reported culture-confirmed conjunctivitis in 42% of 67 newborns exposed to N. gonorrhoeae and 31% among 201 newborns exposed to C. trachomatis; throat cultures were positive for 7% and 2% of exposed newborns, respectively. 17 Another study from 1980s in Kenya reported positive culture of C. trachomatis from the eyes, throat, or rectum in 37% (18/49) of exposed newborns. 18 In that study, some of the positive specimens were only obtained several months after delivery. Interestingly, while a range of frequencies of MTCT of C. trachomatis and N. gonorrhoeae have been reported, only single case reports have reported on MTCT of T. vaginalis. 15 Consequently, to our knowledge, the frequency of MTCT of T. vaginalis is unknown.
Understanding MTCT of STIs and their clinical impact is essential to inform public health interventions and policies aimed at improving newborn health, especially in countries where the prevalence of maternal STIs is high. This study aims to provide insight into the MTCT of C. trachomatis, N. gonorrhoeae, and T. vaginalis, by molecular testing of nasopharyngeal swabs obtained from STI-exposed newborns.
Methods
Study design and setting
This study was part of a larger non-randomized prospective cohort study focused on assessing the acceptability and feasibility of integrating point-of-care STI screening into antenatal care (ANC) services in three primary healthcare facilities in Tshwane District, South Africa. 2 HIV prevalence among pregnant women in this district was 29% in the most recent HIV sentinel survey. 19 Detailed methodology has been previously published. 2 In brief, pregnant women living with HIV were recruited while attending ANC for their pregnancy and managed for STIs either (a) syndromically (i.e., based on symptoms) or (b) based on point-of-care etiological testing for C. trachomatis, N. gonorrhoeae, and T. vaginalis with targeted treatment. Etiological testing was provided to those recruited at first ANC, while those recruited at later ANC visits were provided with syndromic management. Women were only tested at their enrollment visit; however, a 3-week posttreatment test-of-cure was provided. At the first postnatal visit after delivery, all women were tested for C. trachomatis, N. gonorrhoeae, and T. vaginalis using the GeneXpert® platform, regardless of the type of STI management received during antenatal care. Immediately upon test result availability, nasopharyngeal swabs were obtained from newborns of mothers with a positive postnatal STI test and also tested on the same day using the GeneXpert® platform for C. trachomatis, N. gonorrhoeae, and/or T. vaginalis based on the individual maternal STI result(s).
Written informed consent was obtained from all participants prior to study enrollment. The study was approved by the University of Pretoria, Faculty of Health Sciences, Pretoria, South Africa (Ref: 401/215) and the University of California, Los Angeles (Ref: 15-001351).
Procedures, microbiological testing, and antimicrobial treatment
Self-collected vulvovaginal swabs (Xpert® Vaginal/Endocervical Specimen Collection kits (Cepheid, Sunnyvale, CA)) from mothers and clinician-collected nasopharyngeal swabs (UTMTM (Copan Diagnostics, USA)) from newborns were tested using the Xpert® CT/NG and Xpert® TV assays on the GeneXpert® platform (Cepheid) on the same day at the participating facility. Targeted treatment was provided in the case of a positive test result in line with CDC guidelines 20 : azithromycin 1g oral stat dose for mothers with C. trachomatis and azithromycin 20 mg/kg once daily by mouth for 3 days for newborns (a maximum dose of 125 mg) based on local expert opinion. Neisseria gonorrhoeae was treated with stat doses of ceftriaxone 250 mg intramuscular injection and 1g azithromycin oral in the mothers; 50 mg/kg of ceftriaxone was used in asymptomatic newborns. Metronidazole was given as a 7-day course of 400 mg twice daily to mothers and 50 mg/kg once daily by mouth to newborns. All mothers and newborns with a positive STI test result were scheduled for a follow-up visit, including a test-of-cure with further management if indicated, 3 weeks posttreatment. Partner notification and treatment was provided to all women with a positive STI test at any of their ANC visits.
Statistical analysis
All data were entered into a REDCap database (Vanderbilt University, USA) and analyzed using IBM SPSS Statistics version 24 (IBM Corporation, New York, USA). Descriptive summary statistics are presented as counts with proportion (%) and median with interquartile range (IQR). Descriptive summary of the study population is provided. Frequency and 95% confidence intervals (CI) of MTCT for each STI were calculated by dividing the number of newborns with a positive test result for a specific STI by the number of newborns exposed to that STI; newborn exposure was defined by a positive maternal STI test postdelivery. Factors associated with MTCT of STIs were determined via univariate analysis using the chi-squared test or Fisher’s exact test for dichotomous variables (providing the odds ratio (OR) with 95% CI) and the Mann–Whitney U test for continuous variables to compare newborns with and without STI. Factors with a p-value <0.1 in univariate analysis were included in multiple logistic regression analysis. A p-value <0.05 was considered statistically significant.
Results
Characteristics of mothers with and without a diagnosis of sexually transmitted infection at their postnatal visit, Pretoria, South Africa, 2016–2017.
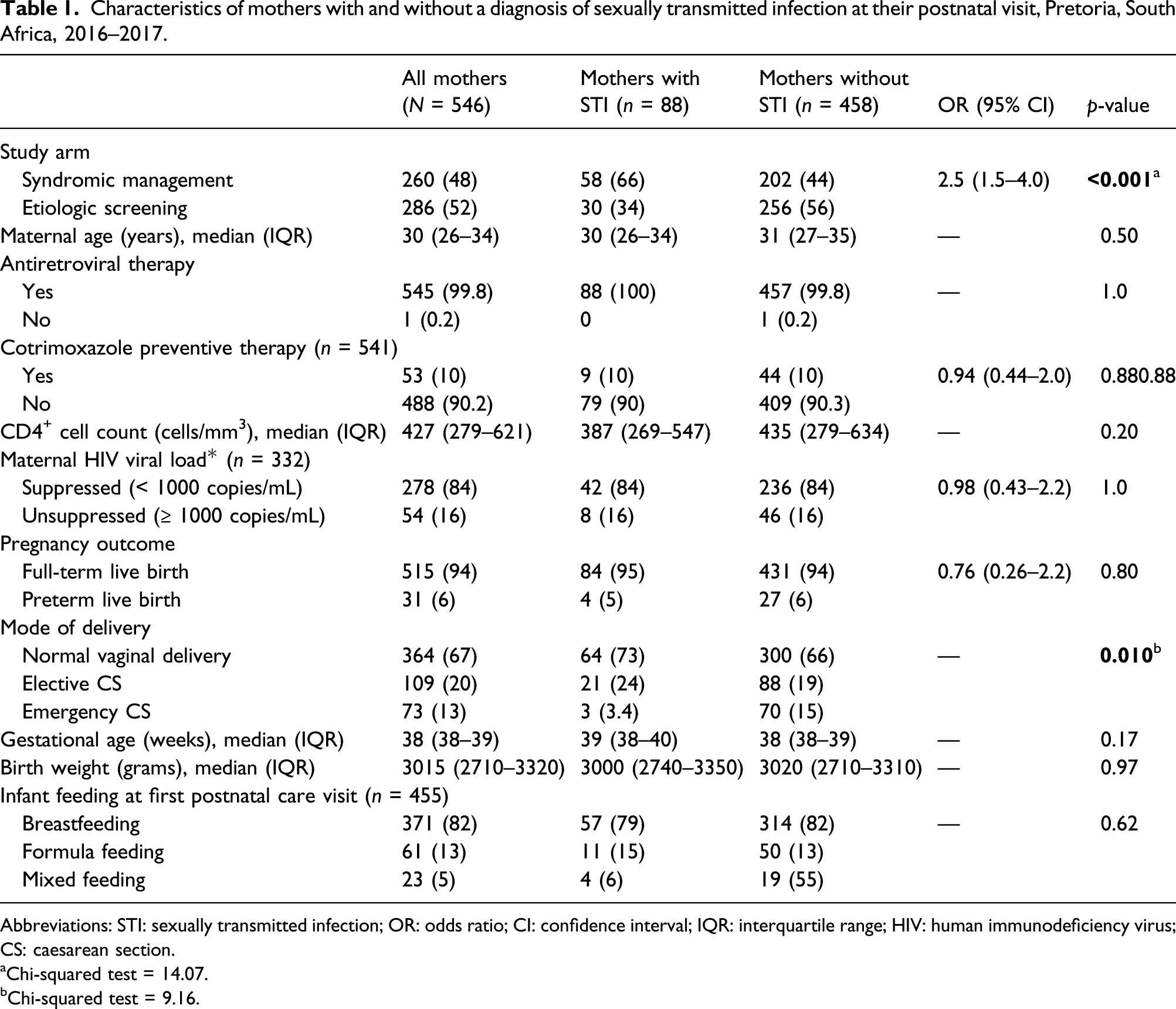
Abbreviations: STI: sexually transmitted infection; OR: odds ratio; CI: confidence interval; IQR: interquartile range; HIV: human immunodeficiency virus; CS: caesarean section.
aChi-squared test = 14.07.
bChi-squared test = 9.16.
STI results for mother–newborn pairs were available for 85/88 (97%) of mothers with a positive STI test result at their postnatal visit: Three newborns were not available for testing, including one that was stillborn. Most women with their newborn (74/85 (87%)) had a postnatal visit with STI test within 14 days of delivery (median 5 days; range 2–12 days); 11 (13%) visited between 14 and 60 days after delivery. Of those mother–infant pairs with a test within 14 days after delivery, 53 (72%) mothers had C. trachomatis, 7 (9.5%) N. gonorrhoeae, and 25 (34%) T. vaginalis infection. One newborn tested positive for HIV at birth.
Frequency of mother-to-child transmission of C. trachomatis, N. gonorrhoeae, and T. vaginalis in mother–newborn pairs in South Africa (n = 74).
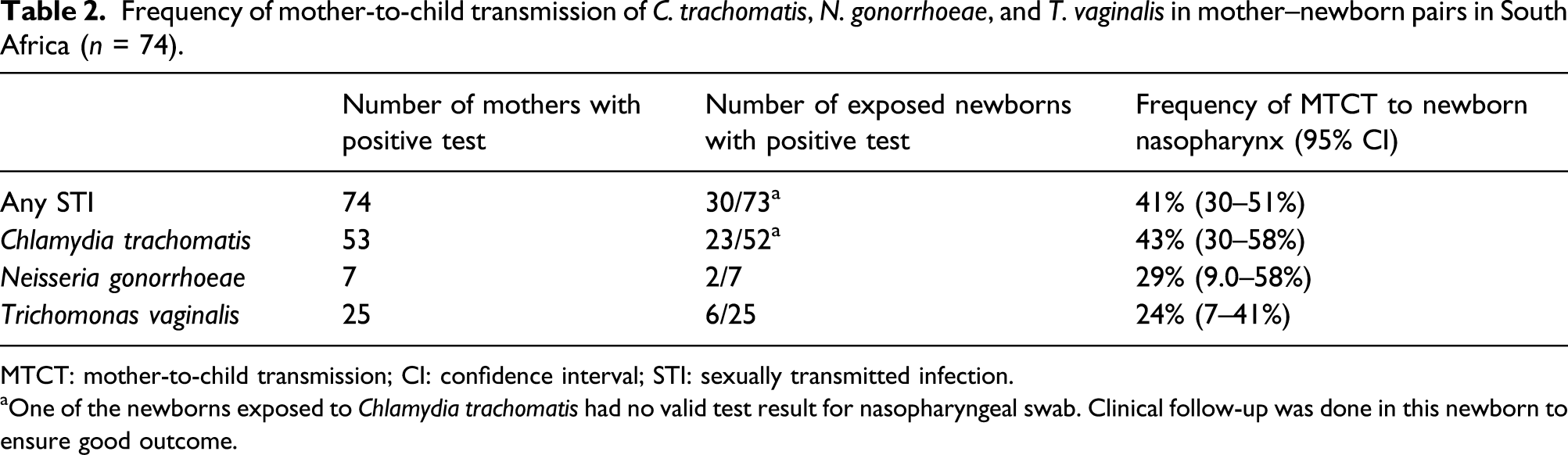
MTCT: mother-to-child transmission; CI: confidence interval; STI: sexually transmitted infection.
aOne of the newborns exposed to Chlamydia trachomatis had no valid test result for nasopharyngeal swab. Clinical follow-up was done in this newborn to ensure good outcome.
All newborns were reported to be in good health at time of the postnatal visit. One newborn had been treated for congenital pneumonia and another one for eye infection prior to their postnatal study visit; both had negative STI tests from their nasopharyngeal specimens. One newborn had been hospitalized for prematurity but is doing well now; T. vaginalis was detected in the nasopharyngeal swab of this newborn at 21 days postdelivery.
Treatment outcome data were available for 29/34 (85%) newborns with a positive nasopharyngeal STI test; five newborns were lost to follow-up (three with C. trachomatis and two with C. trachomatis and T. vaginalis). Test-of-cure was negative in 21/29 (72%) newborns including 13 newborns with C. trachomatis, two with N. gonorrhoeae, and six with T. vaginalis. All eight newborns with a positive C. trachomatis test-of-cure result had documented negative test results following repeated azithromycin treatment for C. trachomatis.
Factors associated with mother-to-child transmission of C. trachomatis in 53 infected pregnant women in Pretoria, South Africa, 2016–2017.
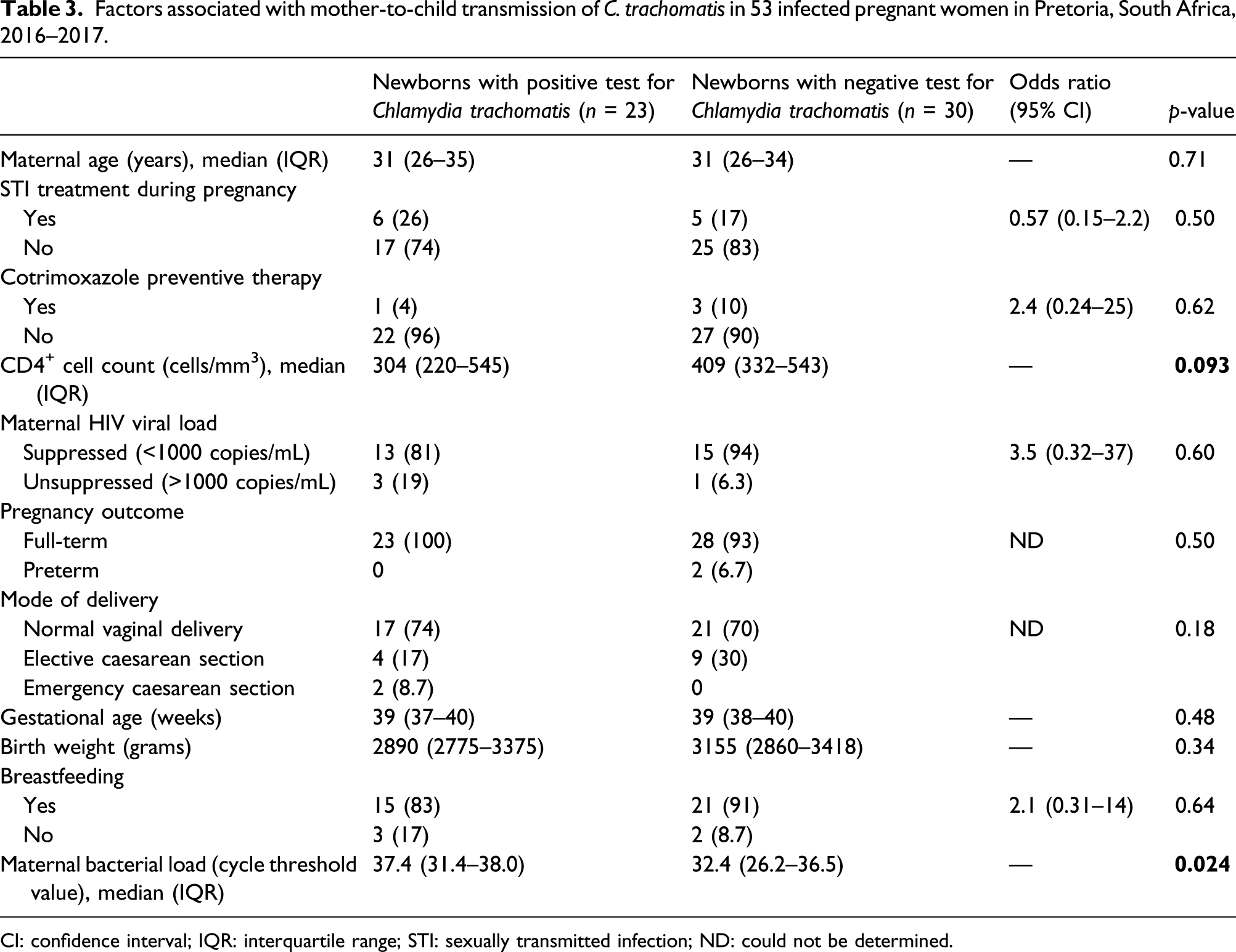
CI: confidence interval; IQR: interquartile range; STI: sexually transmitted infection; ND: could not be determined.
Discussion
This study demonstrates the frequency of MTCT of C. trachomatis, N. gonorrhoeae, and T. vaginalis to the nasopharynx of newborns of women living with HIV in high STI burden settings in sub-Saharan Africa. Of importance, this study is the first to report the frequency of T. vaginalis MTCT frequency; only case reports have been previously reported. 15 While STIs can be detected from the nasopharynx of newborns for a considerable period after delivery and can be either symptomatic or asymptomatic, these organisms respond well to targeted antimicrobial treatment.
Our finding that 43% of exposed newborns had detectable levels of C. trachomatis DNA in the nasopharynx is significantly higher than the 2–18% MTCT previously reported in studies from the United States and Kenya.12,16–18 However, those studies were all from the pre-NAAT era and used microbial culture methods. Sensitivity of molecular assays such as the Xpert® CT/NG assay used in our study is at least equivalent to culture for nasopharyngeal specimens. 21
Data from two national health registries in Finland suggest that the risk of C. trachomatis disease related to vertical transmission in newborns was only 1.8% in their population. 22 That study was based on microbiological diagnosis of symptomatic newborns and did not take subclinical and empirically treated infections into account. The study provides an underestimation of MTCT because most nasopharyngeal infections are asymptomatic. 12
To our knowledge, our study is the first to report on the frequency of MTCT of T. vaginalis. Our data suggest that transmission of T. vaginalis to the nasopharynx occurs in about one-quarter of exposed newborns, that is, in similar range of other STIs, making it potentially an important infection in newborns in sub-Saharan Africa where the prevalence of T. vaginalis in women is generally high.1–7 The clinical relevance of such transmission events requires further investigation.
The clinical spectrum of nasopharyngeal STIs in newborns is diverse. These may present as asymptomatic colonization, a mild respiratory tract infection or severe pneumonia.14,15 Three longitudinal studies from the 1980s suggest that pneumonia develops in 10–20% of all newborns exposed to C. trachomatis and in 25% of those with a positive nasopharyngeal culture.12,15,23 Most newborns in our study were asymptomatic and perceptively healthy. Only one newborn in our study had been treated for pneumonia; no infants with conjunctivitis were identified. However, this may be an underestimation of true occurrence since only those newborns that were doing well would likely have accessed postnatal care at primary healthcare-level facilities. Given that colonization and detection of nonviable DNA may be more readily detected by NAAT-based tests, the progression of nasopharyngeal STIs to respiratory tract disease may occur less frequently than a positive microbial culture.
Lower maternal C. trachomatis DNA load and, in univariate analysis, lower CD4+ cell count were associated with MTCT of C. trachomatis in our cohort of pregnant women living with HIV. We do not have a clear explanation for this observation. Most DNA in genital specimens from women without HIV infection originates from nonviable bacterial cells. 24 We hypothesize that alterations in the immune response related to HIV infection caused changes in the ratio of viable and nonviable bacterial cells in the genital tract, especially in women with low CD4+ cell count, resulting in a lower overall DNA load but higher number of viable, infective cells. Alternatively, this observation may also be the effect of chance related to sampling variation and lack of standardized testing of bacterial DNA load. 25
This study has several limitations. First, for reasons of convenience, we only tested nasopharyngeal specimens and did not include conjunctival specimens. South Africa’s national guidelines recommend provision of chloramphenicol eye ointment for conjunctival prophylaxis; however, the clinical effectiveness of that approach is undocumented. Second, we only used the routine postnatal visit for follow-up. MTCT rates were calculated for mothers who visited within 2 weeks of delivery and reportedly without resuming sexual activity. This may have led to an underestimation of the true MTCT rate because mother–newborn pairs where the child became ill may not have returned for postnatal care and been tested within the 2 weeks’ time period. The observation of positive STI test results in newborns that were more than 2 weeks old has been reported before and requires further research for its clinical significance. Additional standardized follow-up with more extensive clinical data collection would have promoted the inclusion of ill newborns presenting to the health system during the newborn period. Third, we did not confirm the N. gonorrhoeae positive results from newborn nasopharyngeal swabs with a second molecular test; false-positive results due to cross-reaction with pharyngeal Neisseria species cannot be ruled out. Last, only women living with HIV infection were enrolled in this study; the effect of HIV on MTCT of STIs is unknown.
Chlamydia trachomatis, N. gonorrhoeae, and T. vaginalis are common in pregnant women in sub-Saharan Africa as is the frequency of transmission to newborns. The impact of those STIs on newborn health in resource-constraint settings remains to be determined. Although progression of nasopharyngeal colonization to respiratory tract infection and pneumonia may only occur in a minority of newborns, STI colonization might predispose to other respiratory tract infections and chronic respiratory disease later in life. 26 Understanding the short- and long-term health consequences of STI exposure and colonization requires further research in our setting, especially in the context of high maternal HIV prevalence.
Etiologic screening of women for STIs during pregnancy has been shown acceptable, feasible, and reproducible in several resource-limited countries. 27 In our study, women who were managed syndromically for STIs during pregnancy were more than twice as likely to have an STI detected at their postnatal visit than those that received etiologic screening. This highlights the importance of implementing etiologic STI screening during pregnancy as its potential benefits will extend to newborn health.
Supplemental Material
sj-pdf-1-std-10.1177_0956462421990218 – Supplemental Material for Mother-to-child transmission of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis in HIV-infected pregnant women in South Africa
Supplemental Material, sj-pdf-1-std-10.1177_0956462421990218 for Mother-to-child transmission of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis in HIV-infected pregnant women in South Africa by Remco PH Peters, Ute D Feucht, Lindsey de Vos, Phuti Ngwepe, James A McIntyre, Jeffrey D Klausner and Andrew Medina-Marino in International Journal of STD & AIDS
Footnotes
Acknowledgements
The authors would like to acknowledge the Tshwane District Department of Health and clinic managers who gave permission to conduct the study at the respective sites and the facility staff who accommodated our study teams.
Declaration of conflicts of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded via The Eunice Kennedy Shriver Institute of Child Health and Human Development, National Institutes of Health, award R21HD084274 to AMM and JDK, and the President’s Emergency Plan for AIDS Relief through the United States Agency for International Development under the Cooperative Agreement AID 674-A-12–00,017 to the Foundation for Professional Development. Remco PH Peters, Jeffrey D Klausner, and Andrew Medina-Marino were supported through the National Institute for Allergy and Infectious Diseases (award number R01AI149339).
Ethical statement
This study was approved by the University of Pretoria, Faculty of Health Sciences, Pretoria, South Africa (Ref: 401/215) and the University of California, Los Angeles (Ref: 15-001351).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.