
Abstract
Background
The Centers for Disease Control and Prevention recommends universal retesting within 3 months after treatment of Trichomonas vaginalis infection given high rates of persistent infection or reinfection, or if this is not possible, within 12 months following treatment. Data is lacking on how often this is actually done.
Methods
We analyzed the demographic and clinical characteristics, rate of return for the recommended retesting, concordance between wet prep and nucleic acid amplification testing, and percent positivity for T. vaginalis on repeat vaginal specimens at a local public health department in Durham, North Carolina, United States.
Results
Of 193 females treated for trichomoniasis between March 1, 2021 – May 31, 2022, 83% were Black or African American and 44% between the ages of 20 and 29 years. Of these individuals, 32% had retesting performed within 3 months and 50% within 365 days after treatment. Females between the ages of 20 and 29 years were more likely to return for retesting than those between the ages of 30 and 39 years. Of those who returned for retesting, 10% were positive on repeat testing.
Conclusion
In this study, 50% of females diagnosed with trichomoniasis completed retesting within 365 days. Improved scheduling of clients at the time of trichomoniasis treatment and improved identification in our electronic health record of individuals diagnosed with trichomoniasis within the prior year would likely improve retesting rates. Given the high prevalence of trichomoniasis, expanded screening of asymptomatic females in settings where this is feasible may be warranted.
Keywords
Introduction
Trichomoniasis infection, caused by the protozoan Trichomonas vaginalis, is the most common non-viral sexually transmitted infection (STI), with a global incidence of 276 million cases annually, 1 including an estimated 6.8 million cases in the United States (U.S.). 2 Although trichomoniasis infection is not a reportable disease in the U.S. and there are no recommendations for general screening of T. vaginalis, population and clinic-based studies estimate a prevalence of 2.5% in females and 0.5% in males. Trichomoniasis infection is a common cause of vaginal discharge in women and can cause urethritis in men, although infection is often asymptomatic. 3
Although correlation does not imply causation, infection from T. vaginalis has been shown to be associated with a number of adverse health outcomes in women, including pelvic inflammatory disease (PID),4,5 infertility, 6 increased human immunodeficiency virus (HIV) acquisition,7,8 and increased rates of HIV transmission to uninfected partners.9,10 In addition, in pregnant individuals, trichomoniasis is associated with increased rates of preterm delivery11,12 and delivery of low birth-weight babies.11,13,14 In men, T. vaginalis infection is often asymptomatic, although untreated infection can persist for months, and symptoms can include urethral discharge, urethritis, and a burning sensation following sexual intercourse. 15
The Centers for Disease Control and Prevention (CDC) recommends diagnostic testing for T. vaginalis in women with vaginal discharge and consideration for annual screening in persons receiving care in high prevalence settings such as Sexually Transmitted Infection (STI) Clinics and correctional facilities. 16 Screening can be considered in asymptomatic women at high risk for infection, such as those with multiple partners or who engage in transactional sex. 16 Given the high rate of reinfection in women treated for trichomoniasis, the CDC recommends universal retesting within 3 months after treatment, or if this is not possible, within 12 months following treatment, regardless of whether sex partners are treated. Data on how often individuals return for retesting outside of clinical trials is lacking.
We investigated the demographic characteristics of individuals diagnosed with trichomoniasis at the Durham County Department of Public Health (DCoDPH), located in the southern United States (U.S.). In addition, we analyzed how often wet mount microscopy missed T. vaginalis that was subsequently diagnosed by NAAT, rates of concomitant diagnosis of Chlamydia trachomatis (CT), Neisseria gonorrhoeae (GC), and syphilis infection, the rate of return for the recommended retesting, and frequency of positive tests for T. vaginalis at retesting.
Materials and methods
We reviewed the electronic health records (Epic, Verona, WI, U.S.) from March 1, 2021, to May 31, 2022, of individuals seen in our Sexual Health and Women’s Health Clinics at the DCoDPH in Durham, North Carolina, U.S., who were diagnosed with trichomoniasis. Of note, during the study period specimens were sent to our lab from a number of outside organizations for STI testing and demographic and clinical data was not available for these individuals.
During the study period trichomoniasis testing was done in all individuals with female genitalia with genitourinary symptoms (e.g. vaginal irritation, vaginal discharge, etc.). Clinical samples were obtained during a pelvic exam by either a nurse practitioner or physician. A diagnosis of trichomoniasis was made based on either the presence of motile trichomonads on wet mount (initial testing done for individuals with female genitalia who are seen with vaginal symptoms) or a positive transcription-mediated amplification test for T. vaginalis (APTIMA® Unisex Swab Collection Kit (Hologic, San Diego, CA, U.S.)). For individuals with female genitalia and vaginal symptoms who had a negative wet mount, reflex testing with the NAAT was automatically performed at the DCoPDH Laboratory. A list of individuals with a positive wet mount or NAAT test for T. vaginalis was given to the study investigators. For those individuals seen in the Sexual Health or the Women’s Health Clinics at the DCoDPH, further information was collected through review of their electronic health record (EHR).
Characteristics of individuals with treated T. vaginalis by retesting visit status.
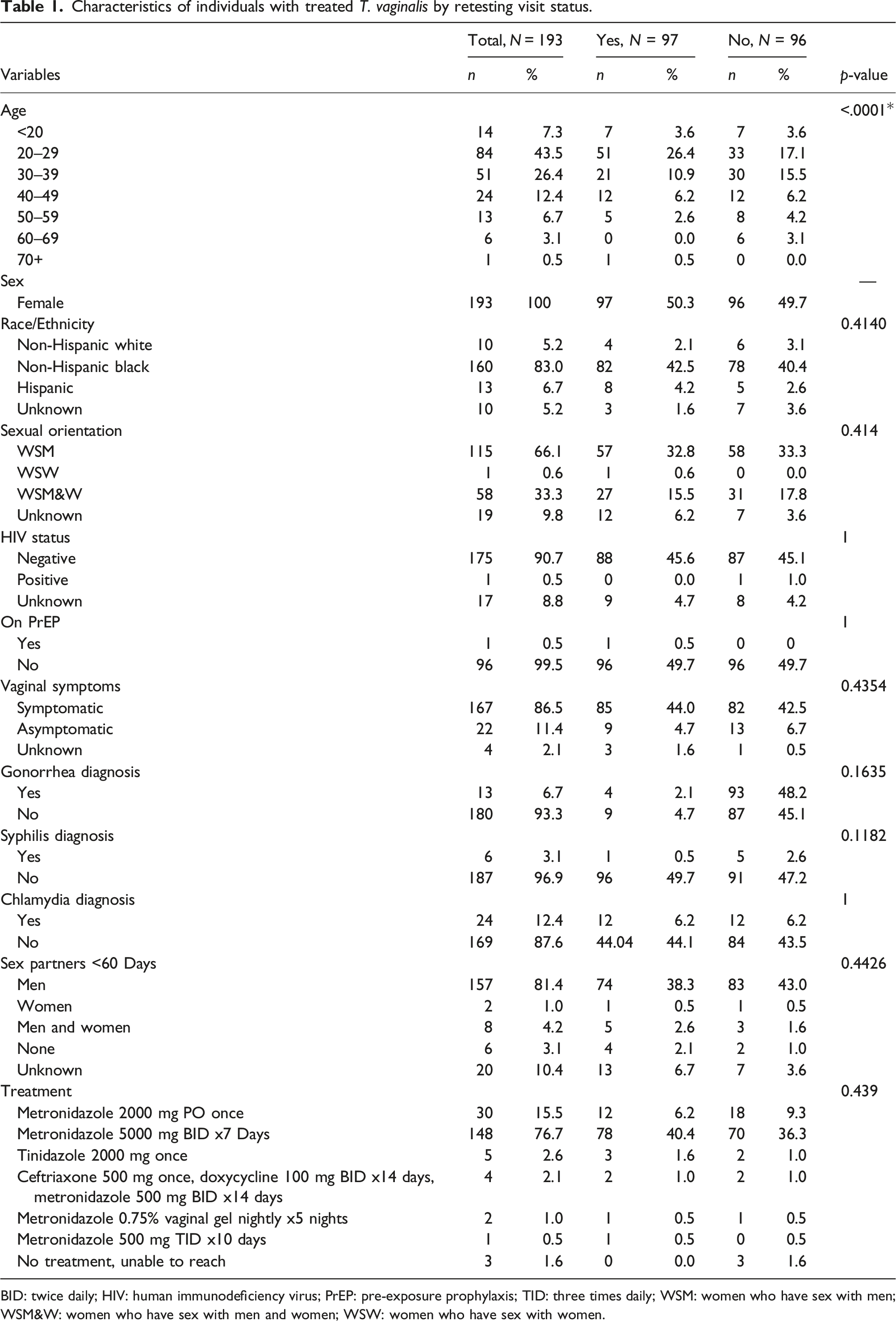
BID: twice daily; HIV: human immunodeficiency virus; PrEP: pre-exposure prophylaxis; TID: three times daily; WSM: women who have sex with men; WSM&W: women who have sex with men and women; WSW: women who have sex with women.
Retesting was routinely advised to individuals diagnosed with trichomoniasis during the study period and was deemed to have occurred if an individual returned to the Sexual Health or Women’s Health Clinics for reassessment and repeat testing for T. vaginalis by wet mount or NAAT within 365 days from treatment. If an individual returned for retesting, we assessed the duration in weeks from treatment date that the retesting was done (<4 weeks, 5–12 weeks, 13–26 weeks, or 27–52 weeks), and whether the repeat test was positive for T. vaginalis. If retesting was performed, we assessed the reason why, such as clients were seen back for routine STI screening, had persistent vaginal symptoms after treatment, had new vaginal symptoms, were scheduled for a retesting, or were seen for routine follow-up. If no retesting was done, we assessed the reason why, which included reasons such as the client was advised to follow-up only if symptoms persisted, advised to return in 3 months for retesting but were not scheduled, were seen within 12 months of treatment but repeat testing was not done, or was scheduled for retesting but cancelled or failed to show up for the appointment.
We performed Chi Square and Fishers Exact Test using SAS 9.4. Chi square test was used when categories had a sample size of greater than 5 (urethral/vaginal symptoms, a concomitant CT, GC, or syphilis diagnosis, days after treatment), while Fisher’s Exact test was used when categories had a sample size of less than or equal to 5. The Odds Ratio was calculated to identify the difference between the two categories and retesting visit status.
This project was exempted as non-research by the Durham County Department of Public Health Review Board.
Results
Of 224 EHRs reviewed that had a positive wet mount or NAAT test for T. vaginalis during the study period, 193 represented new cases and were included in our analysis. Of those that were unevaluable, 15 EHRs lacked any clinical data associated with the diagnosis of trichomoniasis because specimens were obtained outside of DCoDPH; 11 positive tests did not represent new cases; three positive tests were done as lab controls and did not reflect true cases; and two individuals had an invalid NAAT test (neither positive nor negative).
Of those individuals diagnosed with trichomoniasis, 67% were diagnosed by wet mount and 33% by NAAT. Since all individuals with a negative wet mount underwent reflex NAAT, the diagnosis of trichomoniasis was missed in 33% of cases on wet mount only and subsequently made through NAAT.
All persons diagnosed with trichomoniasis were individuals with female genitalia as the APTIMA® Unisex Swab Collection Kit is not approved for use in males and hasn’t been internally validated for use in males at the DCoDPH. Eighty-three percent identified as Black or African American and 44% were between the ages of 20 to 29 years (Table 1). The majority identified as either WSM (66%) or WSM&W (33%), were known to be HIV-negative (91%) and were not on PrEP (99%). The vast majority of persons diagnosed with trichomoniasis were symptomatic (87%), and 12% were diagnosed with concomitant chlamydia, 7% gonorrhea, and 3% with syphilis infection.
Characteristics of retesting visits.
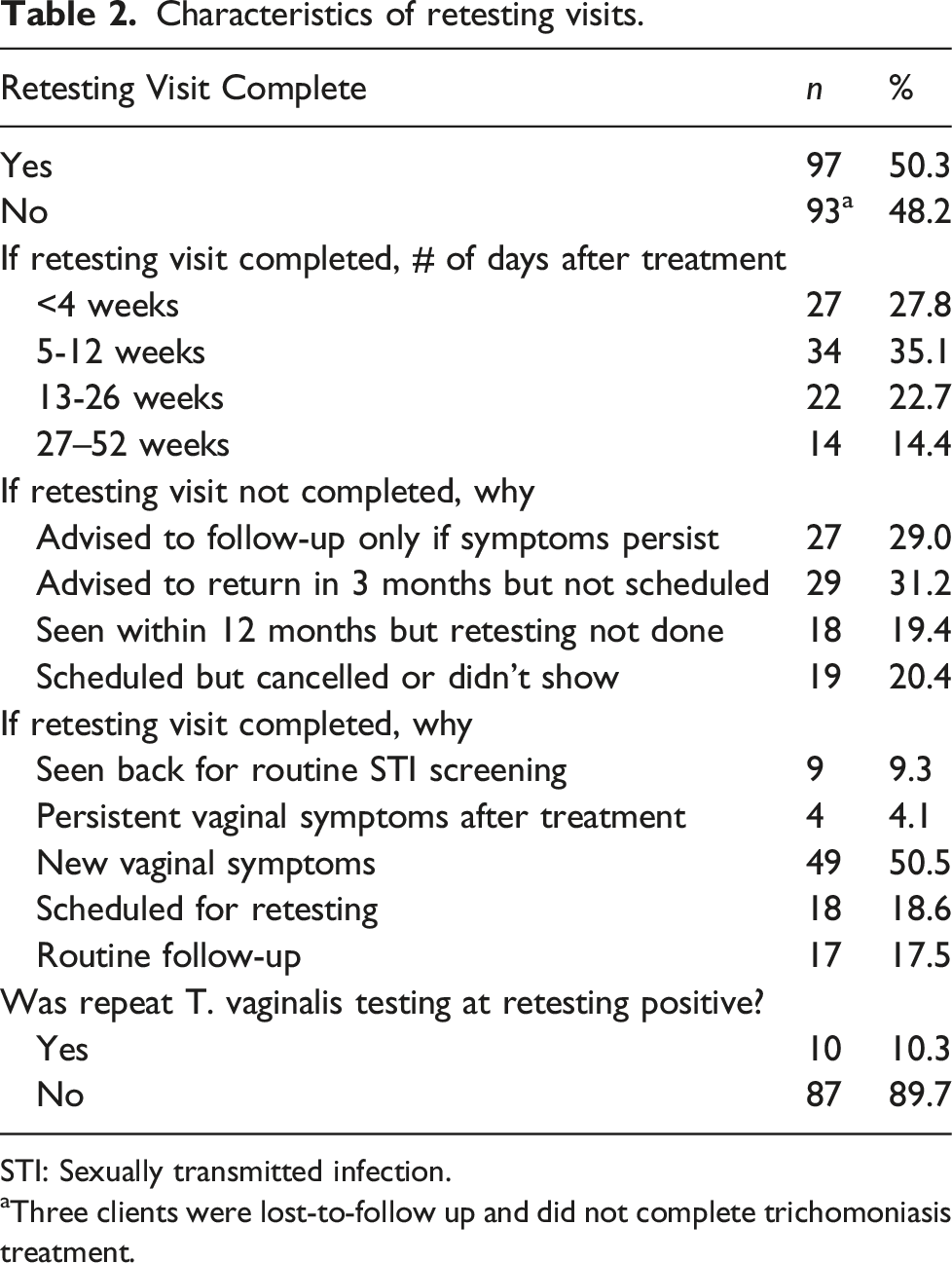
STI: Sexually transmitted infection.
aThree clients were lost-to-follow up and did not complete trichomoniasis treatment.
There was a significant association between age and completing retesting. Individuals between the ages of 20 to 29 years were more likely to have retesting performed compared to individuals between 30 and 39 years of age (26% vs 17%, p < .0001). There was no significant association between sex, race/ethnicity, sexual orientation, HIV status, PrEP status, presence of vaginal symptoms, concomitant STI diagnosis, or treatment regimen used and those who returned or did not return for retesting.
Discussion
In our setting, we found that 50% of females diagnosed with trichomoniasis completed re-testing for trichomoniasis within 365 days, with approximately half of those patients getting retested within 12 weeks of trichomoniasis diagnosis because of new vaginal symptoms. Only 19% had retesting done as scheduled. There is not much data in the literature regarding how often retesting is completed outside of clinical trial settings. In a study of pregnant women screened for STIs in Botswana, of 18 diagnosed with trichomoniasis, 14 (78%) returned for retesting. 17 In another study in the Democratic Republic of Congo, of 52 women diagnosed with trichomoniasis, 45 (87%) returned for retesting. 18 Although our policy is to recommend return for retesting at the time of treatment, we found that in 29% of cases individuals were advised to return only if symptoms persisted. In another 31% of cases, return for retesting within 3 months was advised but an appointment was not scheduled at the time of treatment. In 19% of cases, a client previously diagnosed with trichomoniasis was seen in one of our Clinics for reasons unrelated to trichomoniasis within 365 days of treatment, but no retesting was done. Given these findings, to increase retesting rates it would be best practice if clients were routinely scheduled for retesting at the time of treatment and a better system in the EHR for identifying clients who need retesting when they present to one of our Clinics is needed, even if for reasons unrelated to trichomoniasis. Lastly, 20% of individuals were scheduled for retesting but failed to follow-up for this.
We found that over 10% of females were positive for trichomoniasis on wet mount or NAAT at the time of retesting. This is lower than other retrospective studies, which have detected T. vaginalis on NAAT upon retesting in 24 to 44% of individuals.19,20 High rates of trichomoniasis after treatment are likely due to persistent infection or reinfection from untreated partners. We currently do not perform expedited partner therapy (EPT) in all of our Clinics at DCoDPH so male partners in this case are advised to seek trichomoniasis treatment at the DCoDPH or elsewhere. EPT may have a benefit in the treatment of partners of individuals diagnosed with trichomoniasis, although data for this is currently lacking.16,21,22 More data investigating EPT for the treatment of sex partners of individuals diagnosed with trichomoniasis is warranted.
In our study, wet mount identified T. vaginalis in 67% of individuals diagnosed with trichomoniasis, with NAAT identifying T. vaginalis in the remaining 33% of individuals who were negative by wet mount. Compared to NAAT, the sensitivity of wet mount has been reported between 26%–68%.23,24 At our institution wet mount missed one of 3 cases of trichomoniasis. NAAT is clearly more sensitive and thus preferable in settings able to offer it.
Given that up to 80% of cases of trichomoniasis are asymptomatic, 25 there appears to be a role for screening in asymptomatic individuals in settings where this is a viable option. Currently the DCoDPH only routinely performs testing for trichomoniasis in persons with vaginal symptoms, but we hope to offer screening to all women in the near future as well as testing in males. The current CDC guidelines recommend that annual screening may be considered in persons receiving care in high-prevalence settings such as STI Clinics and for asymptomatic women at high risk for infection such as multiple sex partners or a history of STIs. 16 Given the high prevalence of trichomoniasis – including asymptomatic infections – we agree that more aggressive screening in these high prevalence settings may be warranted.
Our study has several limitations. Firstly, for clients who tested positive for trichomoniasis at the time of retesting, we were unable to differentiate between treatment failure and reinfection. At times clients reported that their partners had not been treated for trichomoniasis and they continued to have sex with them, making reinfection likely, but this was not always the case. Secondly, our sample size was limited as this was a single center study. Thirdly, we relied on the veracity of information relayed to us by clients and the accuracy of reporting in the EHR, so there may be a potential for recall and reporting bias. Lastly, this was a single-center study so our findings may not be generalizable to other settings in other geographic locations, particularly those outside of the public health setting.
In conclusion, we found that 50% of females diagnosed with trichomoniasis completed retesting within 365 days. A significant number of clients were either not scheduled for retesting at the time of treatment or were not re-tested when seen back at the DCoDPH for reasons unrelated to their previous trichomoniasis infection. Efforts to schedule every client for retesting at the time of treatment and improved identification of individuals recently diagnosed with trichomoniasis in the DCoDPH EHR would likely improve retesting rates. In addition, over 10% of individuals were positive for T. vaginalis at retesting, supporting the rationale for retesting and aggressively identifying and treating sex partners. Further study should evaluate the role of EPT in partner management for trichomoniasis. This study supports the use of NAAT for trichomoniasis testing given the low specificity of wet mount. Lastly, consideration should be given to expanding screening of asymptomatic females for trichomoniasis in settings where this is feasible give the high prevalence of trichomoniasis, including in asymptomatic individuals.
Footnotes
Author’s note
A study of female clients in a Sexual Health Clinic in Durham County, North Carolina found that 50% returned for retesting within 365 days, with 10% positivity on re-testing.
Author contributions
JDJ conceived and designed the study. JDJ and LH were involved in data collection. JPZ analyzed the data. JDJ and JPZ wrote the initial draft. ER, CS, KH, LH, SC, and MM provided critical comments. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.