
Abstract
Background
Propagation and microbiological detection of N. gonorrhoeae can be challenging due to the fastidious nature of the bacterium outside the human host environment. Different sample transport options were evaluated in order to address this issue.
Methods
Symptomatic and high-risk patients consented to take part. Standard practice in clinics involve using a guanine and cytosine selective (GC) plate for transport and incubation. Other devices were assessed in two different studies. MWE’s Sigma VCM™-a transport device for use between clinic and laboratory-was used in one study (n = 166). In the other, (n = 102), Biomed’s Intray™ plates were used, which can be used for both initial transport and incubation at the destination laboratory.
Results
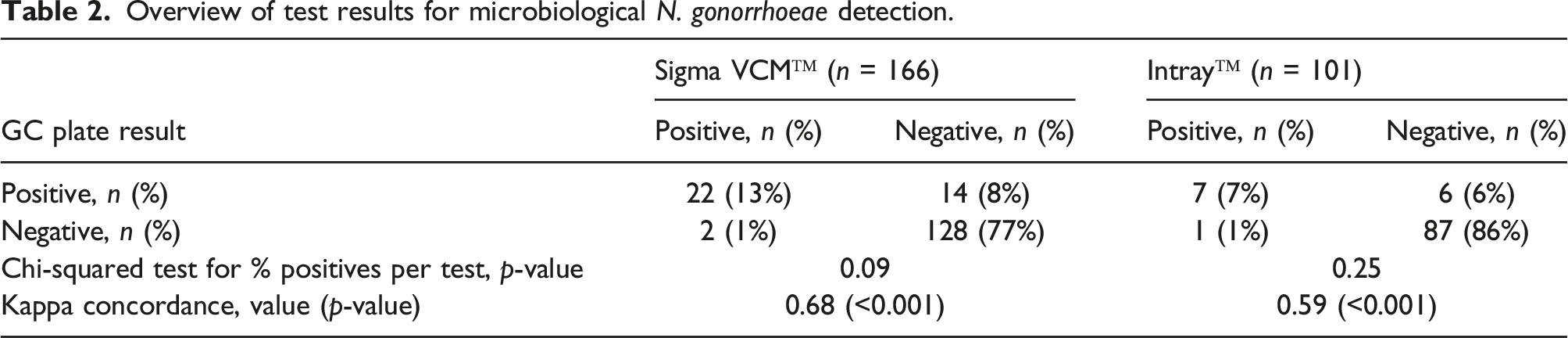
In the Sigma VCM™ study, positive results were obtained for 14% (Sigma VCM™), 21% (GC plates); the distribution of outcomes did not significantly differ between the two microbiological sampling methods (p-value 0.09, Chi-squared test). Concerning the InTray™ sub-study, N. gonorrhoeae was detected in 9% (InTray™), 13% (GC plating) of cases respectively, with again no significant difference between the microbiological sampling methods (p-value 0.25). Regression analysis identified a significant association between N. gonorrhoeae detection and male patients, absence of dysuria and previous gonorrhoea infection.
Conclusion
No significant difference in rate of microbiological detection of N. gonorrhoeae could be detected between different transport devices in a sexual health clinic setting. Performance appraisal of transport devices for bacterial sexually transmitted infection can inform practitioners’ options regarding said devices.
Background
Of approximately 500,000 diagnoses of sexually transmitted infections (STIs) in England per annum, over 40,000 are gonorrhoea cases. 1 The bacterium N. gonorrhoeae causes an infection of the lower genital tract, and undetected or inadequately treated gonorrhoea can cause serious reproductive health consequences such as epididymitis and prostatitis in men and pelvic inflammatory disease, infertility and ectopic pregnancy in women.1–5 Additionally, the emergence of drug resistant gonococcal strains have increased rapidly in recent years, thereby reducing treatment options and causing a threat to public health. 4 Routine diagnostic testing is widely recommended to slow the spread of resistant gonorrhoea.2,6 The incidence of gonorrhoea may be underestimated in some European countries due to suboptimal access to laboratory facilities for microbiological testing and associated antibiotic resistance profiling and/or confirmation of nucleic acid amplification testing (NAAT)-positive samples. 6
Diagnosis of gonorrhoea is confirmed by the detection of N. gonorrhoeae at an infected site. The methods used to diagnose gonorrhoea are influenced by the clinical setting, storage and transport system to the laboratory, which in developed countries typically involves a combination of microbiological incubation culture and NAAT. NAATs are recommended for both symptomatic and asymptomatic infections in men and women and achieve sensitivity of >90%.2,3 A microbiological diagnostic evaluation has the additional benefit of antimicrobial susceptibility testing allowing for early detection of antibiotic resistance.
N. gonorrhoeae bacteria are technically difficult to preserve and recover from clinical specimens. 7 Recovery rates of N. gonorrhoeae also differ per anatomical site; it is particularly challenging to diagnose gonorrhoea from extragenital site samples. 8 For developing countries, the technical and cost challenges around microbiological diagnosis for N. gonorrhoeae may contribute to the use of a syndromic approach to gonorrhoea management rather than using a microbiological approach. 9 In order to achieve effective laboratory diagnosis - bearing in mind the organism’s fastidious nature - it is desirable to optimise collection and transport of samples.10,11 Across two separate evaluation sub-studies, the overall aim was to assess the effectiveness of the novel InTray™ GC system (Biomed Diagnostics) and Sigma VCM™ transport medium (Medical Wire Equipment) compared to the current standard method of plating onto standard agar plates in order to detect N. gonorrhoeae in microbial samples from sexual health clinics.
Methods
Patients and study design
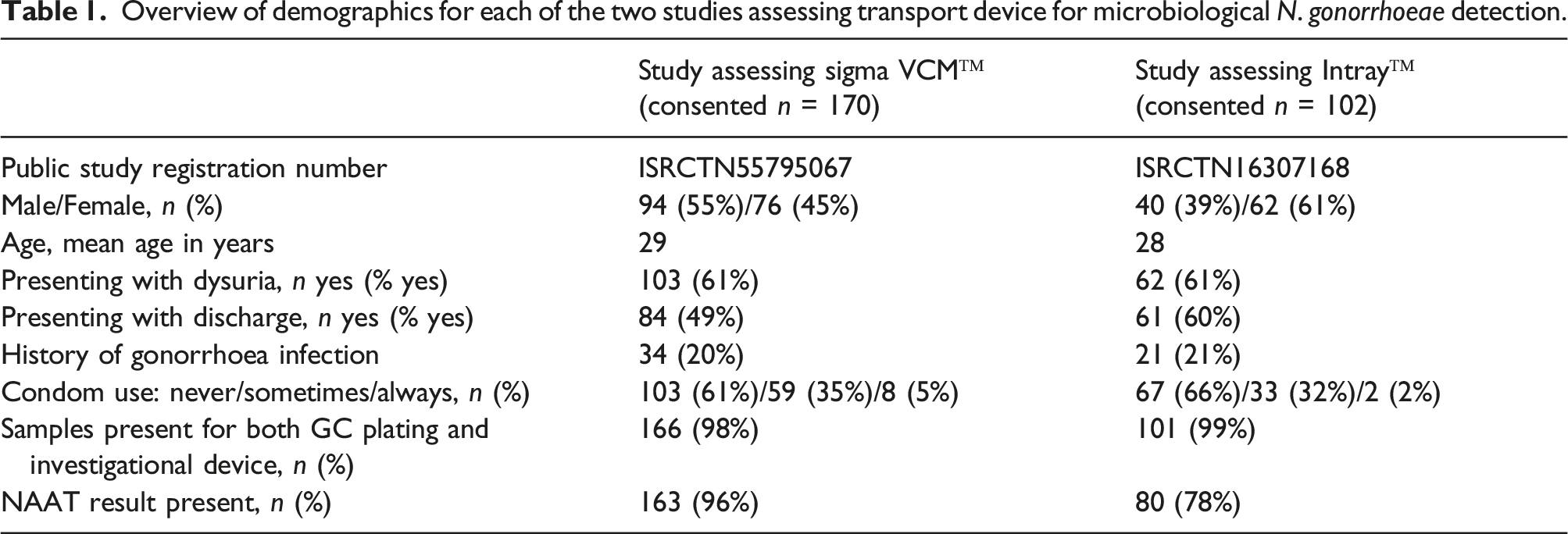
Two separate, consecutive, prospective evaluative studies were conducted at two clinic locations within one National Health Service (NHS) Trust in England between 2018 and 2021. The performance of MWE’s Sigma VCM™ was initially assessed (registered under clinical trial registry number ISRCTN55795067), followed by a subsequent study appraising the Biomed Intray™ product (trial registry reference ISRCTN16307168). This two-stage approach was taken to avoid excessive tissue sampling (swabbing) on the same patient. The methodology, such as patient eligibility, in addition to processing and analysis of standard clinical samples (GC plate and NAAT sample), was identical for each sub-study and is described below. Eligibility included: patient aged 18 years or older, capacity to provide written, informed consent and [a] presentation to a sexual health clinic with symptom(s) that could be indicative of gonorrhoea infection (i.e. presence of urethral or vaginal discharge and/or dysuria) or [b] recent medical history and risk factors that, in the opinion of the treating clinician, warranted investigation for gonorrhoea infection. Full written informed consent was obtained from all study subjects by sexual health nursing staff in a clinic setting. The same staff also collated the study related outcome measures and demographic information, most of this being routinely collated clinical data.
Medical devices and diagnostics
Microbiological testing was the diagnostic test appraised in this study, meaning the growth of bacteria on a selective medium agar plate; 12 the GC plate for standard practice was Oxoid Lysed GC Selective agar with VCAT supplement (Thermo Fisher Scientific). Sigma VCM™ samples transferred onto such plates in the laboratory, whereas Intray™ plate samples did not have to be transferred. However, as part of standard practice in the laboratory, an oxidase test, a Gram stain for positive colonies and confirmatory biochemical API® Neisseria and Haemophilus test were also performed. Once received by the central laboratory, all GC plates were incubated at 37°C and 5% CO2 for a further 48 h, with separate NAAT testing taking place in parallel in the same laboratory. A separate swab was taken for NAAT testing, using AMPLICOR CT/NG Specimen Preparation Kit (Roche Diagnostics) and then EuroClone® dual testing kit for both N. gonorrhoeae and Chlamydia trachomatis on Roche Diagnostics COBAS® system.
As mentioned, patient recruitment took place at two clinic locations. Due to a difference in distance to the central laboratory, there was a subsequent difference in processing and transport of samples. At clinic location A (“direct incubation” method), the GC plates were incubated directly at 37°C until they were collected and transferred in individual, sealed bags (containing CO2 generators) to the central laboratory. At clinic location B (“indirect incubation” method), the streaked GC plates were kept at room temperature in a CO2-rich environment in a gas jar followed by collection and transfer to the central laboratory.
Medical Wire Equipment (Corsham, United Kingdom) markets Sigma VCM™ (MW911S) which meets the Clinical and Laboratory Standards Institute requirements for Quality Control of Microbiological Transport Systems concerning the recovery of N. gonorrhoeae. This is a small vial containing 1.0 mL liquid Amies Transport Medium and contains a cellular foam bud for sampling. At both clinic locations (A and B), the Sigma VCM™ samples were kept at ambient temperature until arrival at the central laboratory where the foam bud was streaked onto a standard GC plate and incubated as per normal procedure.
BioMed Diagnostics (White City, United States) offers InTray™, a microbiology sample collection, transport, and culture in vitro device designed for simultaneous detection and observation of N. gonorrhoeae. The InTray™ system consists of an outer, re-sealable label with a clear window covering the media, which creates an airtight seal over the 2″ diameter surface. An incorporated CO2 tablet can be activated to create a ∼7% CO2 environment. Similar to the GC plates, InTray™ samples were incubated directly at clinic location A, and at clinical location B they were left at room temperature until arrival at the central laboratory.
Outcome measures and analysis
The primary outcome was to determine the respective microbiological detection rates of N. gonorrhoea for Sigma VCM™ and InTray™ compared to current plating practise (GC medium). The secondary outcome was to compare NAAT molecular diagnostics. Sample size calculation was based on a hypothetical 20% absolute difference in positive cases between opposite transport devices, equating to an effect size of 0.4, which translates to a minimum of 48 study subjects when a 80% power and a p-value of 0.05 is defined as a significant difference using Chi-squared test as the inferential statistical test. For samples where a NAAT result was available in addition to microbiological results for standard and investigational transport device, Kappa concordance levels were determined. Since they were not paired, Kappa concordance could not be appraised for Sigma VCM™ versus InTray™. Binary logistic regression was conducted using NAAT and GC plate results as respective dependents, since more samples were available for these methods compared to the two new transport devices tested. Variables included in the model concerned data collated per standard clinical practice (see Table 3). Data was first collated with Microsoft Excel, before analysis with IBM SPSS v24 statistics software.
Results
Overview of demographics for each of the two studies assessing transport device for microbiological N. gonorrhoeae detection.
Overview of test results for microbiological N. gonorrhoeae detection.
Comparison of microbiological versus molecular N. gonorrhoeae diagnostics.
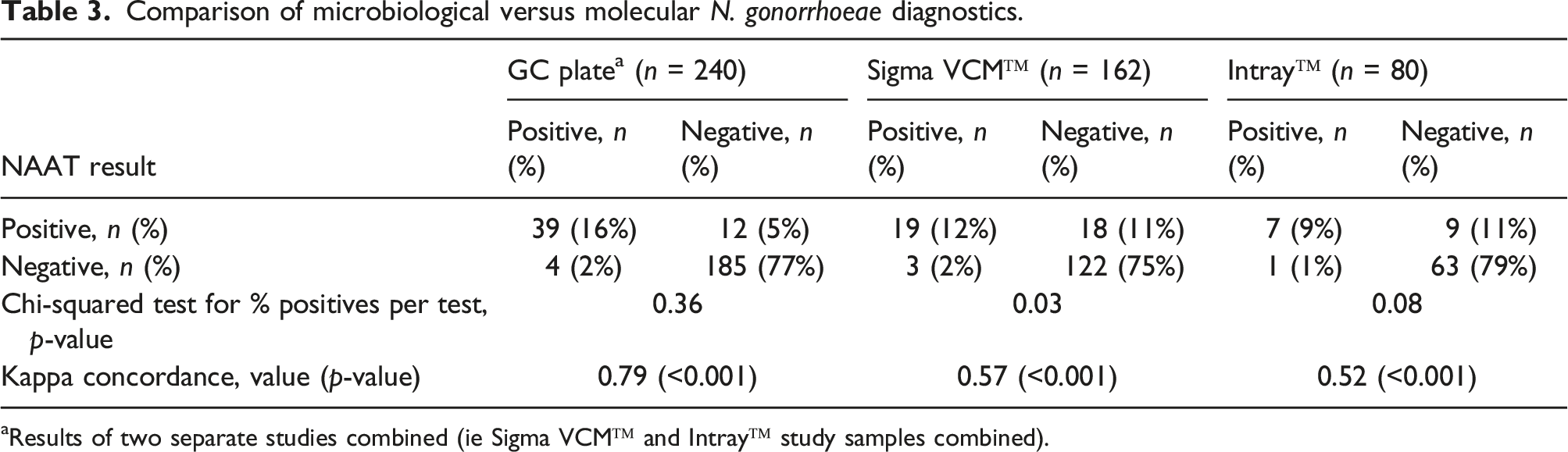
aResults of two separate studies combined (ie Sigma VCM™ and Intray™ study samples combined).
Discussion
Binary logistic regression analysis of variables associated with positive N. gonorrhoeae result.
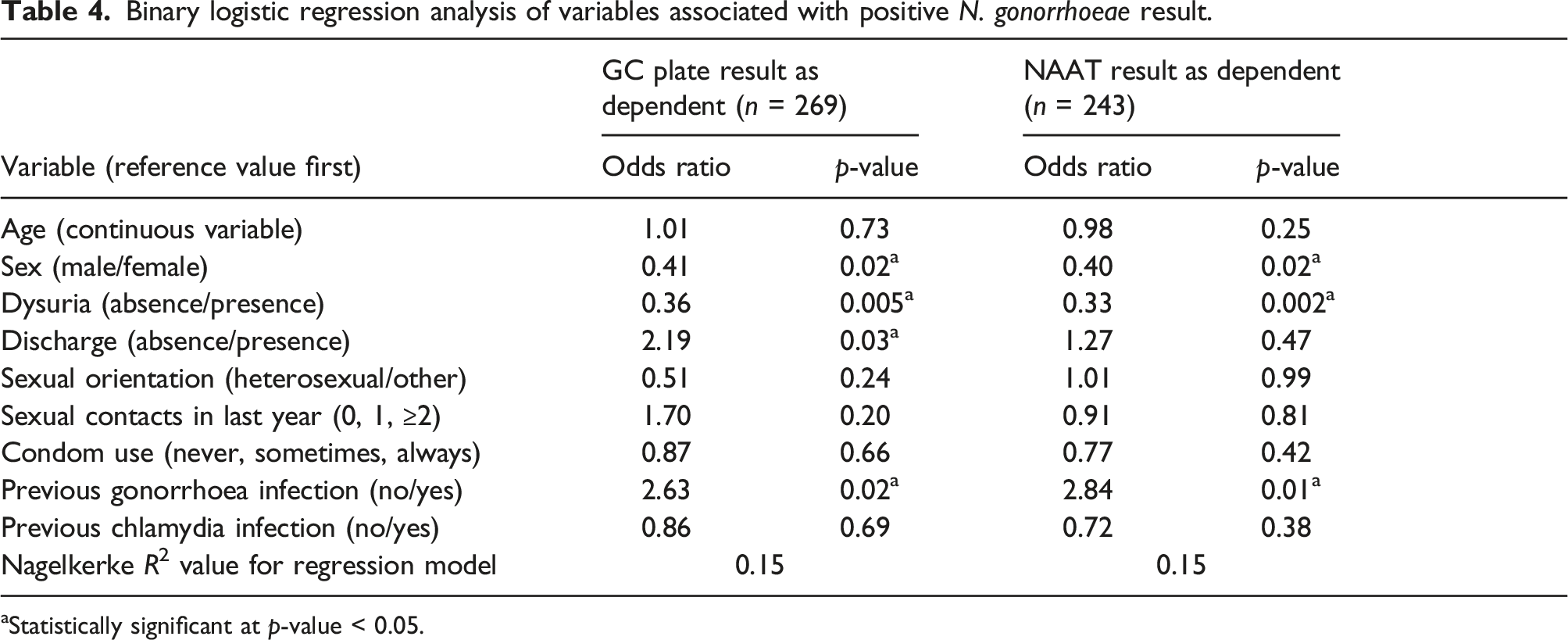
aStatistically significant at p-value < 0.05.
This present “real-world” study differs from some other studies where the performance of different transport devices has been appraised through measurement of recovery rates, i.e. laboratory-based controlled application of N. gonorrhoeae onto either a medium plate or solution to then determine degree of bacterial growth after certain pause and subsequent incubation at 37°C.7,10,11 In our study, the InTray™ device had the lowest concordance levels with both GC plating and NAAT results, but in a controlled experiment with different N. gonorrhoeae strains, recovery rates with use of InTray™ showed less than 10% reduction in average log10 Colony Forming Units (CFUs) per millilitre in a controlled experiment. 14 Two clinic-based studies on patient samples, both comparing InTray™ with modified Thayer-Martin agar plates, found a concordance of >0.85 but InTray™ being negative more often when the Thayer-Martin agar plate samples were positive.15,16 To our knowledge, this is the first time results on relative performance of Sigma VCM™ to standard direct GC plating has been reported; based on outcome distribution and concordance with both standard GC plates and PCR, it does not outperform the others.
The overall performance of NAAT testing for N. gonorrhoeae is more sensitive than microbiological culture methods. 17 However, the results obtained in this present study indicate that NAAT cannot be used as a true gold standard to measure sensitivity and specificity performance because the NAAT result for eight patient samples was negative, yet the microbiology result was positive (a repeat NAAT result was not available in these instances). Previous studies have shown that discordance between culture and NAAT is more often seen in samples from female and asymptomatic patients.18,19 Nonetheless, there have been occasions where the result(s) of either NAAT testing alone or a combined two-of-three positive tests (including mixture of culture results and NAAT results) have been used as a benchmark when appraising medical devices and tests for N. gonorrhoeae.16,17,20 In addition to measuring concordance levels, our regression analysis shows an almost identical profile of what variables are associated with a positive N. gonorrhoeae GC plate result and NAAT result respectively. When further comparing GC culture and NAAT, the standout variable is the presence of discharge, which is significantly associated with GC culture only. This may possibly be due to the presence of a higher bacterial load, required to detect N. gonorrhoeae microbiologically, since this link has previously been demonstrated by others. 21
A methodological advantage of this study (i.e. both sub-studies) is that it was conducted prospectively, and samples were obtained from patients presenting with symptoms of/high-risk history for gonorrhoea infection. One limitation of the study is that patients were enrolled at two locations where processing of the GC plates differs; at one location plates are incubated instantly prior to transport to the central laboratory whereas at the other location they are kept at ambient temperature prior to transport. This may be an issue since N. gonorrheae is sensitive to differing conditions.13,22 The synchronised processing approach for GC plates and Intray™ and specific handling required for the Sigma VCM™ tubes-which cannot be incubated at 37°C and necessitate swabbing of the sample from tube to a GC plate-counter this drawback. Ultimately, it is this multi-location issue that prompted the appraisal of different transport devices. Despite a pragmatic approach to enrich for N. gonorrhoeae positive patients, the overall rate of positive tests was lower than anticipated and this affects the ability to draw conclusions on performance of the Intray™ cohort in particular. It is beyond doubt that, in this sample of patients, GC plating is non-inferior to the more cumbersome and expensive method of using the Sigma VCM™ tubes and more expensive Intray™ plate. Provided that there is awareness of potentially poorer recovery rates, particularly Sigma VCM™ has the advantage that the sample is stored in a locked tube and can potentially be transported over longer distances; this may be suitable in developing countries with fewer microbiology laboratory facilities to enable antibiotic resistance testing. The challenge remains to find ways to improve microbiological N. gonorrhoeae recovery rates, and overall to establish a true, likely molecular technology-based, gold standard test. As part of meeting this challenge it is beneficial for both controlled and clinic-based assessments to be performed to get a clear picture of a device’s (relative) performance. A microbiological device for N. gonorrhoeae transport and recovery will have to be practical and affordable to enable usage in different clinic settings.
Supplemental Material
Supplemental Material - Devices for the transport and microbiological detection of Neisseria gonorrhoeae in sexual health clinic samples: a prospective comparative study
Supplemental Material for Devices for the transport and microbiological detection of Neisseria gonorrhoeae in sexual health clinic samples: a prospective comparative study by Leon Jonker and Matt Phillips in International Journal of STD & AIDS
Footnotes
Acknowledgements
We are grateful to the patients at the participating sexual health clinics, and the sexual health department’s clinical staff for contributing significantly to study subject recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Medical Wire Equipment and Biomed Diagnostics; each provided a non-restricted research grant through free-of-charge provision of medical devices, grant titles ‘STRINGS study’ and ‘GONDOLA study’ respectively.
Contributorship
LJ, conceptualisation, investigation, methodology, formal analysis, writing-original draft; MP, conceptualisation, funding acquisition, chief investigator, study oversight, data collation, writing-reviewing and editing.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation (Health Research Authority, UK) and with the Helsinki Declaration of 1975, as revised in 2008. Ethics approval was obtained via Health Research Authority (references 243037 and 279980) and Research Ethics Committee (references 18/LO/1936 and 20/YH/0223). Participants consented to participating in the study in line with Declaration of Helsinki on Good Clinical Practice.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.