
Abstract
Tyson’s glands are sebaceous glands located on each side of the frenulum that communicate with the preputial sac, and their inflammation can be an infrequent complication of urethritis. We describe a rare case that presented with urethral discharge and parafrenular swelling with mucopurulent discharge a week after an unprotected sexual encounter. The patient was empirically treated with 500 mg of ceftriaxone intramuscularly and 100 mg of doxycycline every 12 h for 14 days with symptomatic resolution. The urethral swab culture and the urine polymerase chain reaction (PCR) were negative for Neisseria gonorrhoeae and Chlamydia trachomatis, therefore, and given the response to treatment, nongonococcal tysonitis was diagnosed.
Keywords
Introduction
Periurethral or parafrenular abscesses are an infrequent complication of urethritis. We describe a rare case that presented as a distal swelling of the penile shaft secondary to the inflammation of the parafrenular glands. In the present article, we aim to shed some light on the anatomy of Tyson’s glands and their possible involvement in sexually transmitted infections.
Case report
A 37-year-old Caucasian homosexual cis-male attended our specialized centre to evaluate urethral discharge and distal penile swelling that started three days before. He reported an unprotected sexual encounter the previous week. No fever, malaise or other systemic symptoms were present. Physical examination revealed parafrenular swelling (Figure 1(a)) with mucopurulent discharge (Figure 1(b)). Microscopic examination of the glandular discharge showed abundant epithelial cells and white blood cells without evident diplococci. The patient was empirically treated with 500 mg of ceftriaxone intramuscularly and 100 mg of doxycycline every 12 h for 7 days. The latter was prolonged to 14 days, given persistent swelling (Figure 1(c)), with symptomatic resolution thereafter. The urethral swab culture and the urine polymerase chain reaction (PCR) were negative for Neisseria gonorrhoeae and Chlamydia trachomatis. A standard bacteriological swab undertaken to look for non-venereal infections presented negative results. The contacts reported by the patient could not be located and studied in our centre, so the partner notification data did not help us to shed more light on the diagnosis. Testing for M. genitalium was not undertaken due to a lack of availability at our centre. Given the clinical and microscopical findings and the response to treatment, nongonococcal tysonitis was diagnosed. Clinical presentation. Panels A & B: Initial clinical presentation. An evident inflammation (presenting as an apparent fluctuating nodule) in the right paraphrenic area was seen (panel A), along with mucopurulent secretion near the orifice of the Tyson's gland (panel B). Panel C: Significant clinical improvement after 7 days. Moderate but palpable inflammation was observed in the area of Tyson's gland, leading to recommend an additional week of treatment with doxycycline.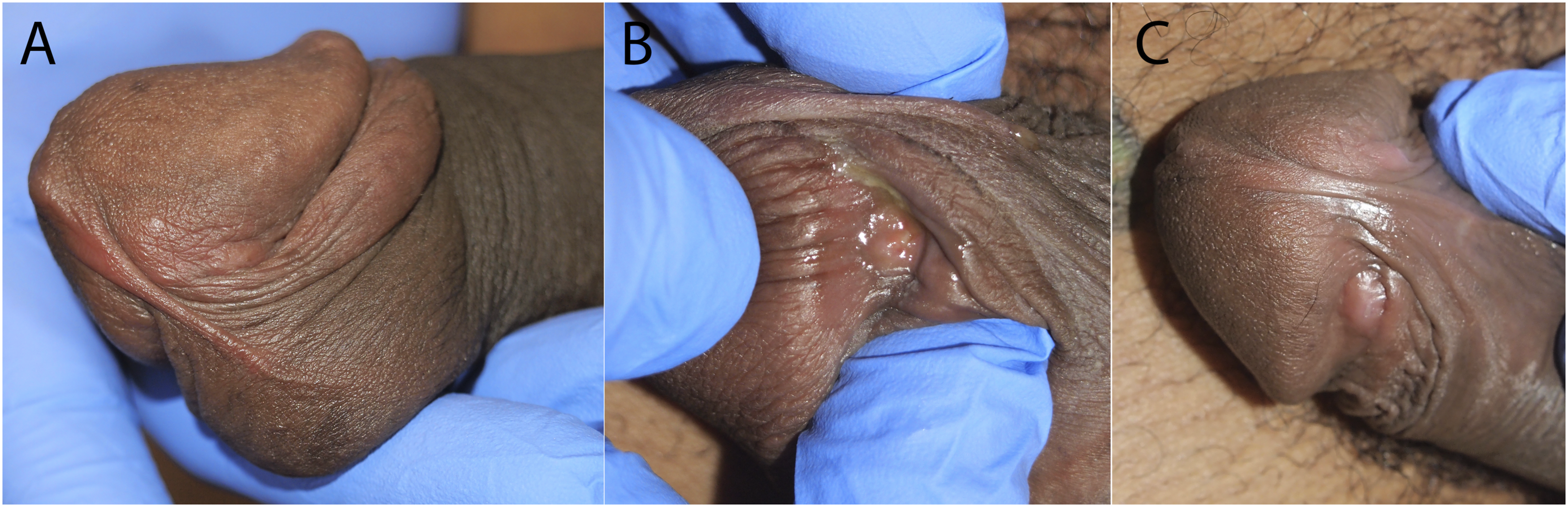
Discussion

The inflammation of Tyson’s glands is known as tysonitis and is an infrequent complication of urethritis due to the direct spread of the infection to parafrenular glands.1,2,5 Clinically it presents with unilateral or bilateral tender swelling on either side of the frenulum.2,6 The main cause of tysonitis is gonococcal infection but it can be caused by other bacteria such as Escherichia coli. 7 Due to its rarity and terminological differences about Tyson’s glands there were only nine cases of gonococcal tysonitis described in the literature before 2000. Since then, one case of non-venereal tysonitis was published in 2018. There was also a clinical study of 15 patients that were diagnosed with tysonitis between the years 2000 and 2020, all whom had been diagnosed with gonorrhea as well. 8 Of all these cases, 21 cases of gonococcal tysonitis were accompanied by urethritis, as our patient, although it can present in isolation.1,2,6,7,9–11 The treatment of this entity is with antibiotics, leaving the possibility of drainage for those cases that do not improve.1,2,6
To conclude, we present the case of a male with nongonococcal tysonitis after unprotected sexual intercourse. We believe that the presentation of this case is relevant for several reasons: first, its apparent low frequency in daily clinical practice; second, to recall the existence of these glands; third, to recognize that it would have been preferable to make the isolations from the discharge of the inflamed gland itself, since it was not possible to confirm a microbiological diagnosis with the available tests. However, the late response to treatment and the improvement after the second week of treatment with doxycycline raises the suspicion of nongonococcal tysonitis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.