
Abstract
The increasing use of non-tenofovir containing antiretroviral regimens calls for renewed attention to the prevention and management of hepatitis B virus (HBV) in people with HIV (PWH). We retrospectively assessed adherence to HBV guidelines, including complete HBV screening in PWH. In people with HIV/HBV co-infection, this included HBV therapy, screening for hepatitis delta virus (HDV) and on-therapy virologic response monitoring. HIV/HBV co-infection in PWH was defined as the presence of hepatitis B surface antigen (HBsAg) at the last measurement before study entry or detectable HBV-DNA for ≥6 months. After assessment, missing laboratory tests were performed to optimize HBV monitoring and screening for co-infections. Of all PWH under follow-up, 1484/1633 (90.9%) were adequately screened for HBV. After performing missing screening tests, 466 of 1618 PWH with complete screening results (28.8%) were non-immune for HBV infection. Fifty-one (3.2%) with HIV/HBV co-infection were identified. HBV treatment was adequate in 51/51 (100%). Screening for hepatitis A, C and delta virus antibodies and fibrosis was performed in 51/51 (100%), 49/51 (96.1%), 17/51 (35.3%) and 38/51 (74.5%). Annual HBV-DNA or HBsAg monitoring was done in 18/51 (35.3%) and hepatocellular carcinoma (HCC) surveillance in 2/9 (22.2%) of those indicated. Additional testing in those with missing data identified 4/34 (11.8%) persons with HDV antibodies and 3/30 (10%) with HBsAg seroclearance. Our study demonstrates the feasibility and added value of evaluating HBV care components and performing missing laboratory tests, identifying a large number of HBV vaccination candidates and HDV antibody screening, HBsAg monitoring and HCC surveillance as key areas for improvement.
Introduction
The advent of tenofovir-containing antiretroviral therapy (ART) has facilitated treatment of hepatitis B virus (HBV) co-infection in people with HIV (PWH), and has been associated with improved clinical outcomes. 1 Tenofovir also protects against the acquisition of HBV infection. 2 However, the increasing use of non-tenofovir containing ART such as dual or long-acting injectable therapy requires renewed attention to the prevention and management of HBV in PWH. 3 This includes recurrent evaluation of multiple care areas, such as HBV screening in PWH (including for those non-immune and eligible for vaccination). In PWH with HBV co-infection (HIV/HBV), additional screening for hepatitis A, C and delta virus (HAV/HCV/HDV) and hepatic fibrosis is advised. Furthermore, evaluation of anti-HBV treatment and on-therapy HBV-DNA or hepatitis B surface antigen (HBsAg) virological response monitoring and hepatocellular carcinoma (HCC) surveillance is recommended.3,4
The quality of guideline-adherent HBV care in people with HIV/HBV has previously been investigated by Lee et al. 5 Despite being essential HBV care components, 3 HBV screening in PWH and virologic response monitoring in people with HIV/HBV were not included in this study. 5 Moreover, no follow-up action was taken regarding the missing laboratory tests found during the study.
Therefore, the aim of our proof-of-concept quality improvement study was to first comprehensively evaluate all aforementioned care areas and then perform missing laboratory tests and inform caregivers of all results, with the goal of exploring the feasibility and added value of this approach for improving HBV care in PWH.
Methods
Study design, population and data collection
A retrospective cross-sectional assessment was conducted in adult PWH between March 2022 and March 2023 in the University Medical Center Utrecht, the Netherlands. PWH were eligible for inclusion if they had an outpatient visit during the study period. Those who objected against participation in research and audits were excluded. Demographic, clinical and laboratory data from the most recent outpatient visit were collected from electronic medical records. This project was undertaken as an audit and as such no ethical approval was required. Data were anonymized at the point of data collection with no patient identifiers retained.
Study definitions
The following definitions were used: • HBV co-infection as hepatitis B surface antigen (HBsAg) presence at the last measurement before study entry or detectable HBV-DNA ≥ 6 months; • complete HBV screening as assessment of serum HBsAg, HB core antibodies (anti-HBc) and HB surface antibodies (anti-HBs); • non-immune for HBV infection as HBsAg, anti-HBs and anti-HBc negative; • HBV/HIV therapy as tenofovir-based cART or entecavir combined with cART; • HAV, HCV and HDV screening as antibody laboratory testing; • fibrosis screening as transient elastography (TE) or liver biopsy; • HBV monitoring as HBV-DNA or, in case of undetectable HBV-DNA, quantitative HBsAg in the year prior to assessment; • HCC screening indication as people with HIV/HBV and advanced fibrosis or cirrhosis (defined as Metavir stage F3/F4 on liver biopsy or liver stiffness ≥ 8.1 kPa on TE);
6
• HCC surveillance as the performance of two hepatic ultrasounds ≤ 6.5 months apart in the year prior to assessment.3,4
Outcomes
In PWH, we assessed HBV screening results to identify those non-immune for HBV infection and thus eligible for vaccination, and those with HBV co-infection. In those non-immune for HBV infection, we specifically assessed whether they were on tenofovir (as tenofovir has been shown to have a protective effect against acquisition of HBV infection). 2
In people with HIV/HBV, we evaluated seven guideline-recommended HBV quality measures: (1) HBV therapy (2) HAV antibody screening and vaccination status (3) HCV antibody screening (4) HDV antibody screening (5) fibrosis screening (6) HBV-DNA or HBsAg monitoring (7) HCC surveillance in case of advanced fibrosis/cirrhosis.3,4
Missing laboratory tests
Following the above assessment, we investigated whether those with missing laboratory tests were under follow-up on March 1, 2023. In individuals still in care, the caregiver’s consent was obtained and missing co-infection screening and HBV monitoring tests were determined retrospectively in blood samples.
Statistical analysis
Continuous data were expressed as mean (standard deviation) or median (interquartile range) for parametric and nonparametric data. Categorical data were compared using Fisher’s exact test or χ2. Continuous variables were compared using the independent samples t test or Mann-Whitney U test. Two-sided p-values <0.05 were considered statistically significant. All analyses were conducted using SPSS version 27.0.
Results
HBV screening and laboratory tests in PWH
Characteristics of PWH and people with HIV/HBV at the time of the outpatient visit.

All categorical data are expressed as number (percentage of total population) and all continuous data are expressed as median (interquartile range) or mean (standard deviation (±)). Bold values indicates p < 0.05.
aMissing data: Time Since HIV diagnosis (2 PWH; 0.1%), time since ART initiation (6 PWH; 0.0%), Creatinine (97 PWH; 6.1%, 2 PWH/HBV; 3.9%), ALAT (22 PWH; 1.4%), current CD4+ count (54 PWH; 3.4%, 3 PWH/HBV; 5.9%), nadir CD4+ (167 PWH; 10.6%, 6 PWH/HBV; 11.8%), current VL <50 copies/mL (100 PWH 6.3%, 3 PWH HBV 5.9%), HBeAg (1 PWH/HBV; 2.0%).
bExcluding 15 elite controllers or long-term non-progressors not on cART and 20 PWH on cART consisting of multiple anchors (1.3%).
cUndetectable HBV-DNA was defined as <7 IU/mL.
Abbreviations: ALAT, Alanine transaminase; ART, antiretroviral therapy; cART, combination antiretroviral therapy; cop, copies; HBV, Hepatitis B Virus; HIV, Human Immunodeficiency Virus; INSTI, integrase strand transfer inhibitor; IVD, intravenous drug use; MSM, men who have sex with men; NNRTI, non-nucleoside reverse transcriptase inhibitor; no., number; PI, protease inhibitor; PWH, people with HIV; VL, viral load.
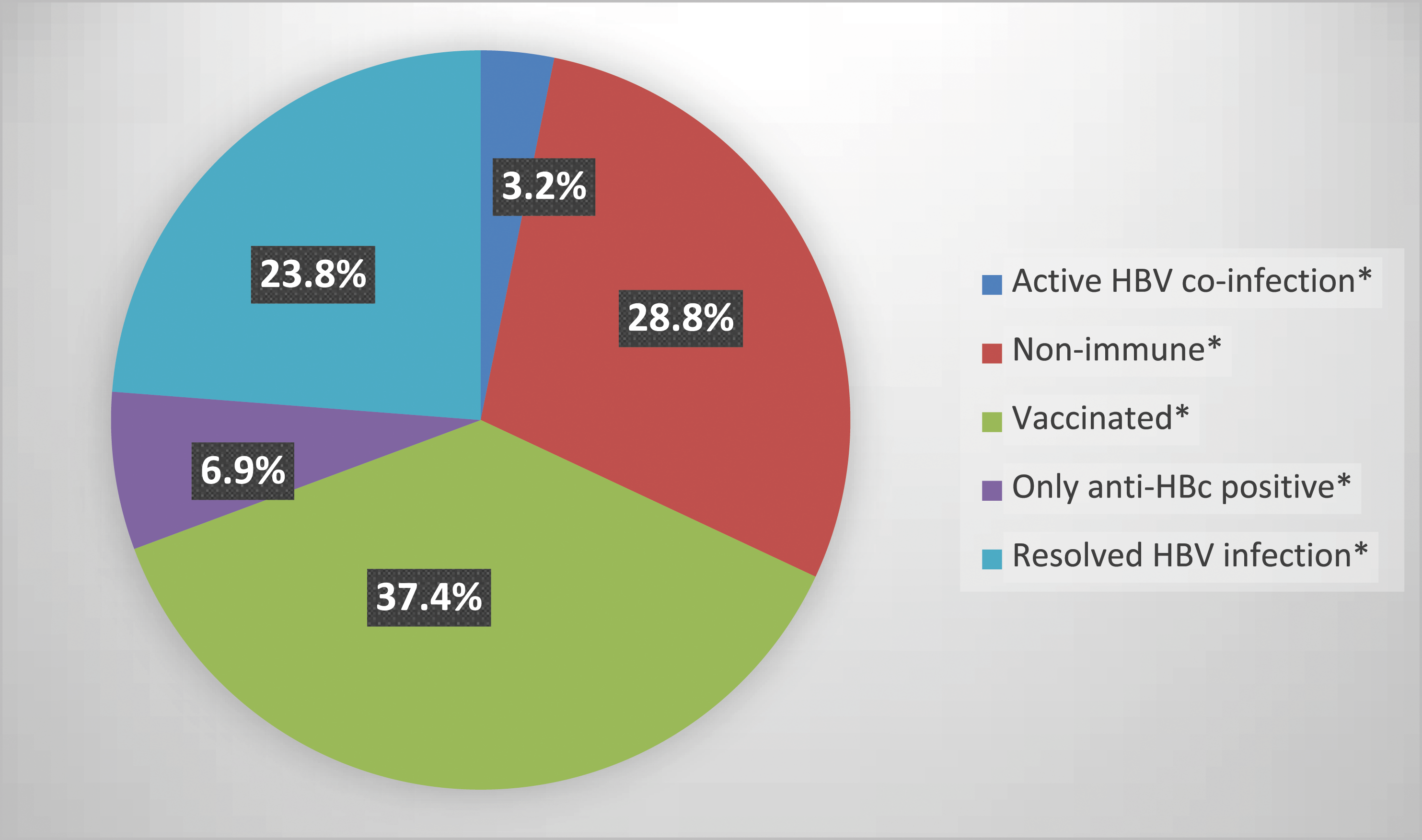
Pie chart showing distribution of HBV serology status in 1618 PWH. Abbreviations: anti-HBc, HB core antibodies; anti-HBs, HB surface antibodies; HBsAg, hepatitis B surface antigen; HBV, Hepatitis B Virus; PWH, people with HIV. *Active HBV co-infection: HBsAg pos, anti-HBs neg, anti-HBc pos; non-immune: HBsAg neg, anti-HBs neg, anti-HBc neg; vaccinated: HBsAg neg, anti-HBs pos, anti-HBc neg; only anti-HBc positive: HBsAg neg, anti-HBs neg, anti-HBc pos; resolved HBV infection: HBsAg neg, anti-HBs pos, anti-HBc neg.
Of the 910 (56.2%) men who have sex with men and therefore considered at high risk for HBV infection, 174 (10.8%) were non-immune and eligible for vaccination. Moreover, 27 (3.0%) of this group were not prescribed a tenofovir-based regimen, placing them at highest risk of HBV infection (given tenofovir’s protective effect against acquisition of HBV infection). Following this assessment, caregivers were informed of their patients’ serologic status and potential vaccination candidates.
Quality measures and laboratory tests in people with HIV/HBV
HBV treatment was adequate, as 51/51 (100%) were on tenofovir-based cART or entecavir combined with cART. Screening for HAV was conducted in 51/51 (100%), five of whom had no HAV antibodies making them eligible for vaccination. Screening for HCV and HDV was performed in 49/51 (96.1%) and 17/51 (33.3%). In 38/51 (74.5%) fibrosis had been screened by TE (31/51) or biopsy (7/51). Annual HBV-DNA or HBsAg monitoring was adequate in 18/51 (35.3%). Inadequate monitoring occurred in 33/51 (64.7%), the most recent HBV-DNA was undetectable in 30/33 individuals, rendering them eligible for HBsAg assessment. Lastly, 9/51 (17.6%) had an HCC indication due to significant fibrosis/cirrhosis. HCC surveillance was adequately conducted in 2/9 (22.2%).
After assessing these quality measures, we investigated whether those with HIV/HBV were in care on March 1, 2023. All were still in care and missing laboratory tests were performed, revealing 2/2 (100%) individuals without HCV antibodies, 4/34 (11.8%) with HDV antibodies but without HDV RNA and 3/30 (10%) with HBsAg seroclearance. None of those with HBsAg seroclearance had anti-HBsAg antibodies. Following this assessment, caregivers were informed of all results, particularly regarding inadequate quality measures and abnormal laboratory tests.
Discussion
In this cross-sectional study, we aimed to assess and improve guideline-adherent HBV care in PWH. Our study demonstrates the feasibility and added value of evaluating HBV care components and performing missing laboratory tests. Main findings include the large number of HBV vaccination candidates as well as HDV antibody screening, HBsAg monitoring and HCC surveillance being key areas for improvement in people with HIV/HBV.
A recent study by Lee et al. that examined guideline-adherent HBV care in people with HIV/HBV found that although HBV treatment and HCV screening were adequate, HAV screening and HCC surveillance were substandard. 5 Importantly, there was no mention of HBV screening and virologic response monitoring and missing laboratory tests were not performed retrospectively, so that any clinical implications remained unknown. We assessed all aforementioned care components and performing missing tests, thus revealing important key improvement areas.
HDV antibody screening had only been performed in 33% of individuals and missing tests revealed 4 (11.8%) with antibodies. In 2021, 5% of Dutch people with HIV/HBV tested for HDV had an active HDV infection, while only 12% of the total population had been tested, suggesting a large group of undetected active HDV infections. 7 Our numbers are consistent with this and underscore the need for increased awareness of HDV in caregivers, particularly in light of new treatment options. 8 HBV monitoring was identified as second improvement area: only 35% received guideline-adherent monitoring. After performing missing tests, we observed 10% HBsAg seroclearance. HBsAg seroclearance is relevant as it is associated with low risk of developing HCC and improved survival, and it allows caregivers to consider discontinuing anti-HBV treatment, limiting tenofovir-based toxicity and facilitating greater ART choice.3,9 Importantly, HBsAg seroclearance seems more prevalent in people with HIV/HBV than those with HBV mono-infection, presumably due to an immune reconstitution inflammatory syndrome type-effect with rapid expansion of CD4+ T-cells and anti-HBV immune response. 9 European HIV guidelines recommend annual HBsAg testing until loss of HBsAg and that in case of HBsAg loss with anti-HBsAg antibody acquisition, anti-HBV therapy may be stopped. 10 In 2021, <10% of Dutch people with HIV/HBV were tested for HBsAg seroclearance, underscoring the limited attention among caregivers and suggesting that a large group nationwide may also have HBsAg seroclearance. 7 Finally, the rate of guideline-adherent HCC surveillance was 22%. Although strikingly low, these numbers are in line with previous studies reporting rates of 7%–55%.5,11–13 It seems awareness of HCC surveillance is low among caregivers, and our study reinforces this notion and identifies this as an important area of improvement.
The next step in improving HBV care in PWH would be implementation of targeted healthcare interventions in areas found to be substandard in this study. For example, in the case of HDV, reflex testing could be used, where a positive HBsAg result immediately triggers HDV antibody screening in PWH. In Spain, the implementation of this has led to five times more HDV diagnoses, albeit in people with HBV mono-infection. 14 Given this result and our research findings, our center has chosen to implement this step and is currently evaluating its impact. In addition, interventions for HCC surveillance could include automated checklists for every newly diagnosed person with HIV/HBV to assess their HCC surveillance indication, as well as automated reminders or educational programs for both caregivers and those with HIV/HBV. 15
Our study has several strengths. To our knowledge, our study has the most comprehensive evaluation of HBV quality measures, unlike previous studies often focusing on a limited number of measures,5,11–13,16 and was thus able to identify multiple HBV care improvement areas. Additionally, our quality improvement study is the first to subsequently perform missing laboratory tests and, as a proof-of-concept, demonstrates that our approach is feasible and results in additional important clinical findings.
Our study is limited by the single-center design and small number of individuals with HIV/HBV, which may render our results not fully generalizable to other centers.
In conclusion, our study demonstrates the feasibility and added value of systematically evaluating HBV care components and performing missing laboratory tests. The key areas for improvement are the large number of HBV vaccination candidates and the substandard HDV antibody screening, HBsAg monitoring and HCC surveillance in people with HIV/HBV.
Footnotes
Author contributions
B.W. designed the study and wrote the study protocol. P.O., V.K. and A.G. collected and analyzed the data. P.O. drafted the manuscript in close collaboration with B.W. All authors contributed to the interpretation of the results, critically reviewed the manuscript and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.