
Abstract
Co-infection with HIV and hepatitis B virus (HBV) has serious long-term consequences. We describe a case of an HIV-infected heterosexual black African man with a delayed diagnosis of HBV infection. Baseline HBV screening was performed using a sequential testing algorithm starting with a total core antibody (anti-HBc) test, which was negative. He had no evidence of immunity against HBV and subsequently received three unsuccessful courses of HBV vaccination. He had mild but persistent elevation of liver enzymes over a five-year period despite maintaining full suppression of HIV replication on efavirenz, lamivudine and zidovudine; the latter was changed to abacavir due to lipoatrophy. Further testing revealed e-antibody positive chronic HBV infection with undetectable anti-HBc reactivity. High-grade HBV viraemia associated with L180M and M240V drug-resistance mutations was confirmed. He was subsequently switched to a tenofovir-based regimen, which achieved HBV suppression. Adopting effective HBV screening strategies in HIV-infected patients is recommended.
INTRODUCTION
Hepatitis B virus (HBV) and HIV co-infection has a significant impact on disease progression as well as all-cause mortality. 1 The burden of HIV/HBV co-infection in the UK is estimated to be about 7%. 2 Serological diagnosis of HBV infection can be challenging in a minority of patients who test negative to surface antigen (HBsAg) and/or total core antibodies (anti-HBc). In occult HBV infection, defined as the presence of HBV deoxyribonucleic acid (DNA) in the liver (with or without detectable HBV DNA in blood) in individuals who test negative for HBsAg, a fifth of patients have negative anti-HBc serostatus. 3,4 Lack of anti-HBc reactivity despite detection of HBsAg in some patients with chronic HBV infection has been attributed to an underlying immunocompromised status or poor assay sensitivity. 5
CASE REPORT
Patient's hepatitis B vaccination courses and corresponding surrogate markers for HIV
The patient managed to achieve undetectable HIV viral load within six months of commencing antiretroviral therapy (ART) with efavirenz, lamivudine and zidovudine. The latter was switched to abacavir later in the course of his management because of lipoatrophy. His HIV viral load remained fully suppressed throughout his follow-up period; however, he was noted to have had mild but persistent elevation of his liver transaminases over several years (Figure 1).
Pattern of liver enzymes over a five-year period. AST = aspartate transaminase; ALT = alanine transaminase; ALP = alkaline phosphatase. Normal ranges for bilirubin, AST, ALT and ALP are 3–21 µmol/L, 10–35 U/L, 10–35 U/L and 30–150 U/L, respectively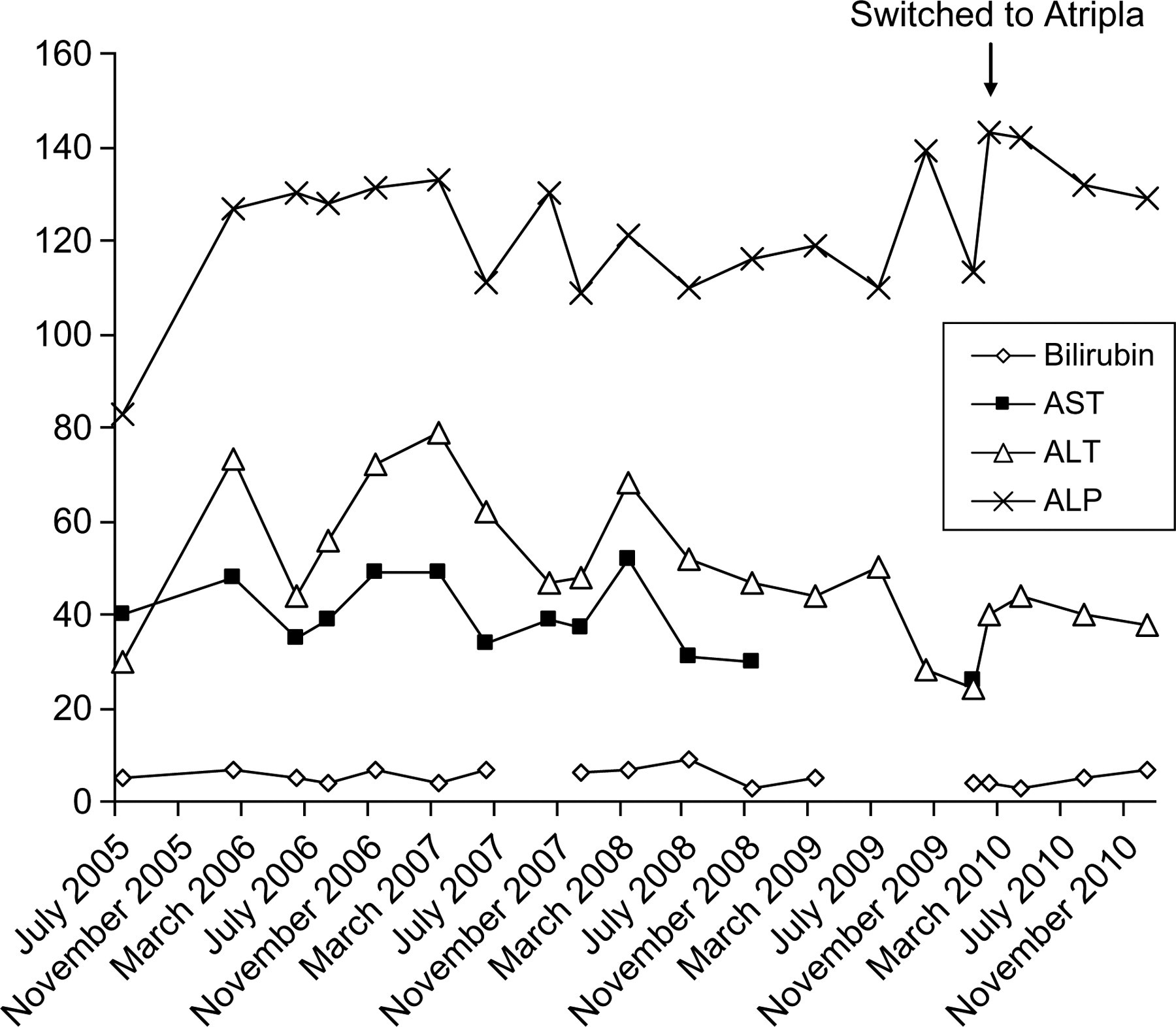
An abdominal ultrasound scan was unremarkable. Further tests for HBV in 2010 were consistent with e-antibody-positive chronic HBV infection with a viral load of 309,956,747 IU/mL (logarithmic value [log10] 8.49). Anti-HBc remained non-reactive despite achieving CD4 counts above 300 cells/µL. A genotype A HBV strain was identified with major drug resistance mutations in the form of L180M and M204V. Hepatitis D (delta) virus serology was negative and hepatitis C virus ribonucleic acid was not detected by polymerase chain reaction (PCR).
Our patient was switched to co-formulated tenofovir, emtricitabine and efavirenz in order to optimize his management. Six months later, his HBV DNA levels decreased to 814 IU/mL (log102.91) while HIV viral load remained fully suppressed. Our patient's wife, who was first diagnosed with HIV infection in 2005, tested negative for HBV using baseline screening with HBsAg and anti-HBc and has subsequently received a successful course of HBV vaccination.
DISCUSSION
We present a case of an HIV-infected patient whose concomitant HBV diagnosis was missed because of adoption of a sequential HBV testing algorithm starting with anti-HBc. Investigations of his liver enzyme abnormalities led to a diagnosis of occult chronic HBV with signature mutations conferring full and partial resistance to lamivudine and entecavir, respectively. This was a direct consequence of having received lamivudine monotherapy for his unrecognized HBV co-infection.
Our patient was first screened for HBV using a sequential testing algorithm starting with only anti-HBc. 6 Though this strategy may be appropriate for HBV screening in the general population, specific guidelines for screening HIV-infected patients currently recommend frontline HBV testing with both HBsAg and anti-HBc while also considering HBV DNA PCR in severely immunocompromised patients. 7 This case highlights that screening for HBV infection with anti-HBc alone can lead to a delay in diagnosis, as our patient has consistently failed to produce detectable levels of anti-HBc despite being exposed to HBV.
The M204V mutation induces 1000-fold reduction in the in vitro susceptibility of HBV to lamivudine in comparison to wild-type isolates. 8,12 In addition, L180M is a compensatory mutation whose presence indicates a high-level lamivudine resistance. Moreover, entecavir resistance requires prior lamivudine exposure as well as a stepwise development of two signature mutations (M204V and L180M) followed by a third additional mutation (S202I or M250V). 9,13 In our case, we opted for a tenofovir-based regimen as this has been shown to be highly effective in both lamivudine-naïve and lamivudine-experienced HIV/HBV co-infected individuals. 10,11
Effective HBV diagnostic strategies should be adopted in HIV-infected individuals in order to help optimize ART selection, avoid emergence of resistance and offer appropriate vaccination advice.
Footnotes
ACKNOWLEDGEMENT
Both CT and ZOEB contributed equally to this work. We thank Dr Martin Prince for his help with the management of this case.