
Abstract
Background
Herpes simplex virus (HSV) is a common infection, affecting the majority of the population by age of 50. Recurrent symptomatic outbreaks, experienced by a minority, have significant psychological and psychosexual effects. The varicella zoster virus (VZV), resembling HSV, shows potential for a functional cure via vaccination. This study seeks to investigate if there is an association between low VZV antibody levels and recurrent HSV outbreaks.
Methods
A total of 110 patients with symptomatic and asymptomatic HSV were recruited during their sexual health screen. Serum samples were collected between Aug 2019 - July 2022; breaks in the study occurred due to COVID. The primary outcome measure was the serological status of HSV and VZV IgG titre level.
Results
The average age was 37.3 years (range 21–65 years). For people with asymptomatic genital HSV2 the average VZV IgG titre was 2373.9 IU/mL (n = 17); and 1219.0 IU/mL for the symptomatic group (n = 67); p ≤ 0.00001), with similar results for HSV1.
Conclusion
There is a strong association between average higher varicella-zoster virus (VZV) IgG level and being an asymptomatic carrier of herpes simplex sirus (HSV)1&2. A feasibility study to assess the use of the VZV vaccine as a treatment of HSV is planned.
Background
Herpes, caused by herpes simplex virus (HSV), is a common and widespread infection. The variation in prevalence of either HSV1 or HSV2 infection varies in countries with prevalences of HSV1 ranging from 84% in Bulgaria to 52% in Finland and for HSV2 ranging from 14% in Germany to 4% in England. 1 The worldwide prevalence of both types of HSV is 60%–90% at the age of 50.2,3 HSV is responsible for the majority of genital ulcer disease (GUD). HSV2 infects approximately 536 million people worldwide 4 and is associated with an increased susceptibility to other sexually transmitted infections (STIs), including HIV. Despite significant efforts, there has been limited progress in the effectiveness of genital herpes screening and prevention strategies over the past decade.5,6
Varicella zoster zirus (VZV) glycoprotein E (gE) shares structural similarities with its counterpart in HSV. 7 These similarities stem from their common evolutionary ancestry within the Herpesviridae family. Both gE proteins play crucial roles in viral pathogenesis and immune evasion,8,9 facilitating viral spread within the host.
Current research suggests that the VZV vaccine, which primarily targets VZV gE among other viral components, induces a robust and long-lasting host immune response. The vaccine prompts the production of specific antibodies and memory T-cells, contributing to durable immunity against VZV. This sustained immune protection has been observed to last for several decades after vaccination, effectively reducing the risk of VZV reactivation and disease, including herpes zoster (shingles). This remarkable longevity of vaccine-induced immunity raises intriguing possibilities for harnessing similar mechanisms to combat other herpes viruses, including HSV, and warrants further investigation.
Notably, research has uncovered an interesting phenomenon: an increase in antibody levels against HSV-deoxyThymidine Kinase (dTK) during VZV infections. 10 The virus-encoded thymidine kinase for both HSV and VZV is a target for future treatments. 11 This finding raises the prospect of developing a comprehensive treatment approach that could target a broad spectrum of human herpes viruses (HHV) within the alpha subfamily.
Our case-control study aims to elucidate the relationship between elevated VZV IgG levels and the asymptomatic carriage of both HSV1 and HSV2. By doing so, we hope to provide valuable insights into the potential of the VZV vaccine as a candidate for managing recurrent HSV infections.
Methods
Study setting
One hundred and ten adults at a sexual health centre in Reading, UK (August 2019 to July 2022) were enrolled during their genitourinary medical review. None of the patients had any previous VZV or Herpes zoster vaccination. HSV green top universal transport medium polymerase chain reaction (PCR) swabs were taken from recurrent HSV patients having an outbreak, and an extra clotted blood vial was taken to measure VZV IgG titers on the Diasorin Liasion platform & HSV IgG titers tested on the Hologic Panther platform.
Patient data included demographics, number of children, HSV infection status, number of outbreaks in the previous year, average length of outbreak, number of years since diagnosis and suppression therapy status. During COVID lockdown, the study was placed on hold to ensure reduction of spread of COVID-19. When this study was restarted, patients were required to adhere to standard COVID-19 rules for the hospital. To be allowed into the sexual health unit all patients were asymptomatic of COVID-19 during recruitment.
Symptomatic patients were defined as in our inclusion criteria: any adult (18 years of age or older) who is willing to give informed consent and has a diagnosis of HSV2 genital herpes in the last 2–30 years, either has continuous regular outbreaks (4 or more in any rolling year) or is on suppression therapy to prevent recurrence. Controls: any adult who was diagnosed with genital HSV2 infection between 2–30 years ago, is not on suppression therapy and has had no outbreaks in the previous year.
Ethics approval
The study was approved by The Royal Berkshire Hospital and the National Health Service Ethics board (IRAS Project ID: 260102), with participants providing written informed consent.
Results
The average age of the 110 participants was 37 years (range: 21–65 years), with similar age distributions in the HSV1 and HSV2 groups. Among the participants, 67 had HSV1, 84 had HSV2, and 39 had both infections. Twenty-five of the participants were on outbreak therapy (n = 15) or long term suppression therapy (n = 10) at the time blood was taken.
Out of the 110 participants, 18 had never been diagnosed with genital herpes and never had an outbreak; a few other patients were never formally diagnosed but did have previous outbreaks. All individuals who never had an outbreak and never diagnosed were recruited due to a history of prior contact with recurrent herpes partners and diagnosed by blood sample, 9 of them being HSV1 only, the others being HSV2 or had both infections. Twenty-three patients out of 110 had a positive genital swab at the time of recruitment. All others may have been diagnosed elsewhere or diagnosed on clinical examination alone, so diagnosed was confirmed by blood sample.
Each group (HSV1, HSV2 and any HSV together) were analysed separately. Supplementary Tables 1, 2, 3, and 4 provide additional demographic data and detailed results for HSV1, HSV2, and both infections combined. The main findings are summarized below.
For HSV1 (n = 67, 36 were male, 41 were symptomatic (25 females, 16 males)) the average VZV IgG titre was 2049.0 IU/mL for the asymptomatic group (n = 26) and 1078.5 IU/mL for the symptomatic group (n = 41; p = 0.001).
For HSV2 (n = 84, 44 were female, 67 were symptomatic (41 females 26 males)) the average VZV IgG titre was 2373.9 IU/mL for the asymptomatic group (n = 17) and 1219.0 IU/mL for the symptomatic group (n = 67); p ≤ 0.00001).
For any HSV infection (n = 110, if patient has HSV1&2 then only set of demographic data was analysed (duplicates removed)) the average VZV IgG titre was 2011.2 for the asymptomatic group (n = 32) and 1166.5 for the symptomatic group (n = 78; p ≤ 0.00001), see Figure 1 for graphical representation for all three sets of data. HSV1 there is a significant difference in VZV IgG titres between two independent means. Asymptomatic group of 26 participants (M = 2049) and a symptomatic group of 41 participants (M = 1078.5), (Two tale, p-value is 0.001). Sample size effect, Hedges’ g = 1.04 (>0.8) = large effect. HSV2 there is a significant difference in VZV IgG titres between these two independent means. Asymptomatic group of 17 participants (M = 2374) and a symptomatic group of 67 participants (M = 1219), (Two tale, p-value is < 0.00001). Sample size effect, Hedges' g = 1.6 (>0.8) = large effect. For HSV1 and HSV2 combined there is a significant difference in VZV IgG titres between these two independent means. Asymptomatic group of 32 participants (M = 2011) and a symptomatic group of 78 participants (M = 1166.5), (Two tale, p-value is < 0.00001). Sample size effect, Hedges' g = 1.12 (>0.8) = large effect. Black lines are 95% Confidence intervals placed on all the mean bars.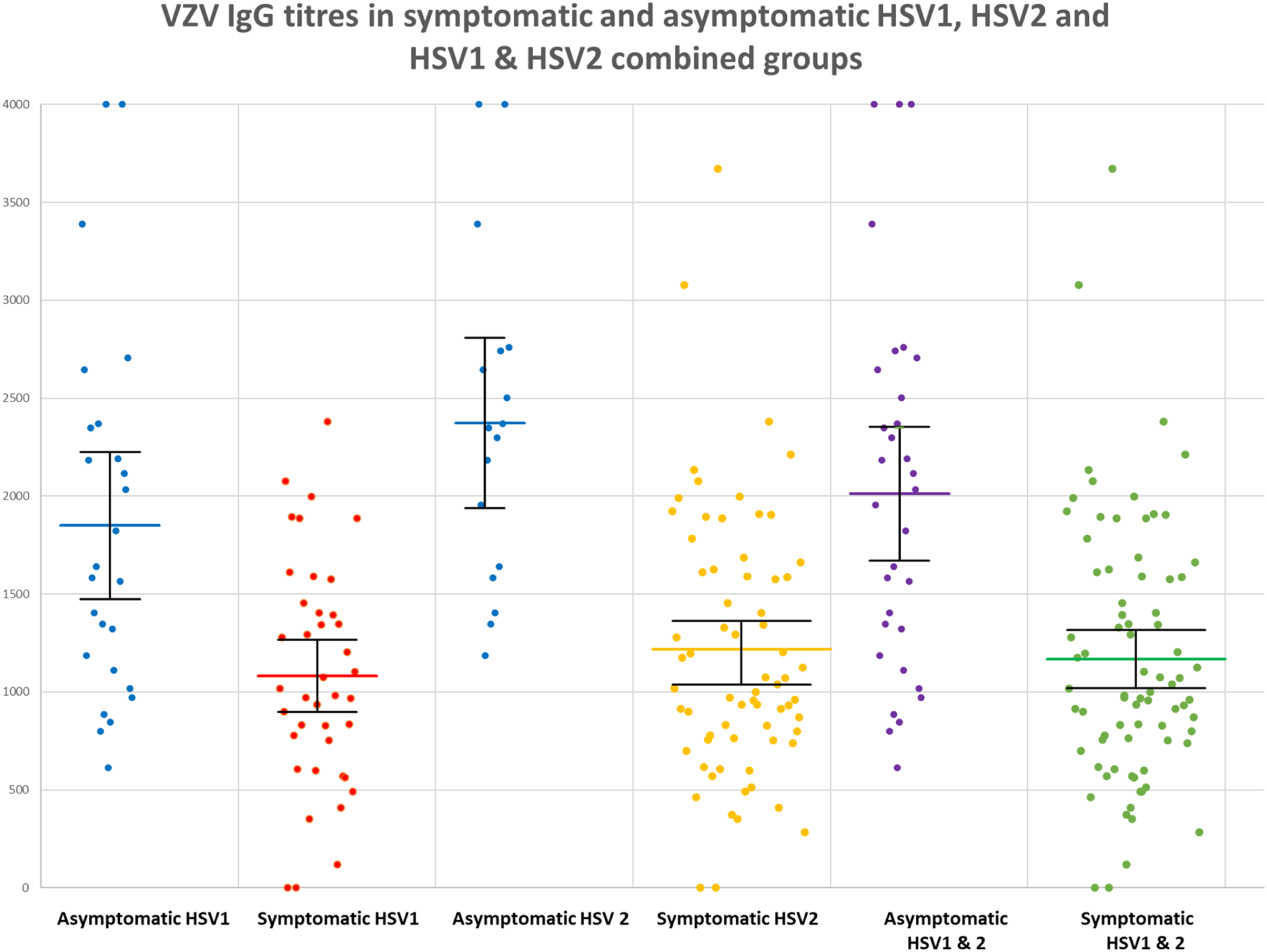
No association was found between age, ethnicity, number of children, number of outbreaks, length of outbreaks in the previous year or time since diagnoses and VZV IgG level, please see supplementary tables 1, 2, 3 & 4.
Discussion and conclusions
This pioneering study marks the first demonstration of a compelling association between VZV IgG levels and the symptomatic status of HSV. While other investigations have hinted at the potential of VZV vaccination in addressing HSV, our research underscores the relevance of VZV IgG levels as a pivotal factor in understanding and potentially managing recurrent HSV infections. Other studies have indicated the possibility of treating HSV with VZV vaccination.12–14
It is worth acknowledging certain limitations in our study. Many participants presented with genital HSV symptoms during recruitment, some of whom had asymptomatic partners, albeit the exact proportion of such cases remains unrecorded. This situation may introduce self-selection and recall biases. Additionally, a subset of patients were under various forms of suppression therapy, either for outbreaks or continuous management. However, considering that existing medical knowledge does not associate VZV IgG titers with HSV symptomatic status, we believe these biases have minimal impact on our findings. Notably, while acyclovir consumption directly affects the efficacy of the VZV vaccine, it does not significantly influence VZV IgG titers, ensuring the robustness of our results. Furthermore, the uniform processing of all VZV samples on the Diasorin Liasion and HSV blood samples on the Hologic Panther platform, with VZV reported in standard International Units (IU), minimizes the likelihood of substantial discrepancies across different diagnostic platforms in potential future studies.
In this study, HSV status confirmation primarily relied on serum samples, utilizing HSV IgG analysis, which may not be the most precise method. HSV status was only recorded as positive or negative, and the actual titre level should have been noted to see if there was an association with patients VZV IgG titre for assessing overall strength of the immune system. HSV titre level should be recorded in future studies. However, the sensitivity and specificity of most platforms surpass 90%, a level deemed acceptable for our study's purpose of detecting associations. One noteworthy omission in our study was the lack of recording HSV titers, representing an opportunity missed to explore the relationship between HSV IgG titers and VZV IgG titers, potentially yielding more comprehensive insights into the discovered association.
Prior research has shed light on the VZV vaccine's capacity to elevate IgG titers, increase the percentages of VZV-specific memory T-cells and memory B-cells, in transplant patients.1,15 This suggests that IgG titers may serve as indicators of T-cell function, extending beyond their role as mere antibodies. Additionally, the concept of trained immunity gains prominence, hinting at broader cell-mediated immune effects applicable to human herpes viruses and other viral infections.
While we acknowledge the potential role of age-related T-cell mediated immunity decline in initial HSV outbreaks among older individuals, our study lacked the necessary power to establish a concrete association between age and declining VZV IgG titers. Future investigations should carefully consider age-related VZV IgG decline as a potential confounding factor, particularly in studies assessing the efficacy of the VZV vaccine. Age restrictions, either focusing on younger or older populations, can mitigate this potential source of bias.
In the United States, VZV vaccination is predominantly administered during childhood, typically completed by age 6.1,16 Nevertheless, research indicates that the immunological response to VZV vaccination is weaker compared to natural infection, affording approximately 20 years of protection 17 rather than the typical 50 years. This disparity in vaccine uptake across different demographic groups, especially minority populations, in previous decades may have contributed to a higher burden of HSV infections, including in pregnancy and neonatal cases. 18 While our study did not detect significant associations between ethnicity, number of children, or age and HSV status, we attribute this to limited statistical power. Future, larger-scale studies will be better equipped to address these factors comprehensively.
Looking ahead, a feasibility study is planned to explore the potential use of the VZV vaccine as a treatment for HSV. This endeavour holds the promise of unravelling further insights and novel strategies in the ongoing battle against recurrent HSV infections.
Supplemental Material
Supplemental Material - Is the level of varicella-zoster virus IgG associated with symptomatic status of genital herpes simplex virus infection? A case-control study
Supplemental Material for Is the level of varicella-zoster virus IgG associated with symptomatic status of genital herpes simplex virus infection? A case-control study by Bret S. Palmer, Alan Tang, Stephen Winchester, Mark Atkins, Simon Barton and Peter Kelleher in International Journal of STD & AIDS.
Supplemental Material
Supplemental Material - Is the level of varicella-zoster virus IgG associated with symptomatic status of genital herpes simplex virus infection? A case-control study
Supplemental Material for Is the level of varicella-zoster virus IgG associated with symptomatic status of genital herpes simplex virus infection? A case-control study by Bret S. Palmer, Alan Tang, Stephen Winchester, Mark Atkins, Simon Barton and Peter Kelleher in International Journal of STD & AIDS.
Supplemental Material
Supplemental Material - Is the level of varicella-zoster virus IgG associated with symptomatic status of genital herpes simplex virus infection? A case-control study
Supplemental Material for Is the level of varicella-zoster virus IgG associated with symptomatic status of genital herpes simplex virus infection? A case-control study by Bret S. Palmer, Alan Tang, Stephen Winchester, Mark Atkins, Simon Barton and Peter Kelleher in International Journal of STD & AIDS.
Supplemental Material
Supplemental Material - Is the level of varicella-zoster virus IgG associated with symptomatic status of genital herpes simplex virus infection? A case-control study
Supplemental Material for Is the level of varicella-zoster virus IgG associated with symptomatic status of genital herpes simplex virus infection? A case-control study by Bret S. Palmer, Alan Tang, Stephen Winchester, Mark Atkins, Simon Barton and Peter Kelleher in International Journal of STD & AIDS.
Footnotes
Acknowledgements
We would also like to thank Dr Charlotte Lomer for her time in grammar and sense checking this work.
Authors’ contribution
Bret Palmer planned, conducted, reported the work described in this short communication on the academic guidance of Mark Atkins, Alan Tang, Simon Barton and Peter Kelleher. All processing of laboratory samples and forwarding results to Bret Palmer was done by Stephen Winchester. Bret Palmer analysed the data. Bret Palmer wrote the paper. All Authors contributed in the review and editing of the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The VZV case-controlled study was funded by the Florey Clinic Reading. The authors have received no financial contribution for this work.
Ethical statement
Provenance and peer review
Not commissioned; externally peer reviewed
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.