
Abstract
Background
The two main objectives were to evaluate the COVID-19 point prevalence and the test performance of the WHO case definition to diagnose COVID-19 clinically in people with HIV in West Ukraine.
Methods
Multicenter cross-sectional study in Lviv, Ukraine, from October 2020-November 2021. COVID-19 unvaccinated people with HIV were included regardless of COVID-19 symptoms at routine clinical visits and had standardized medical, quality of life (EQ(5D)) and SARS-CoV-2 serology assessments. Reported symptoms indicating potential COVID-19 events at inclusion or between March 2020 and inclusion were classified by the WHO case definition as suspected, probable or confirmed. A clinical COVID-19 case was defined as being SARS-CoV-2 seropositive with at least a suspected COVID-19 according to the WHO case definition. The primary endpoints were the clinical COVID-19 prevalence and the test characteristics of the WHO case definition with SARS-CoV-2 serology as reference. (Clinicaltrials.gov:NCT04711954).
Results
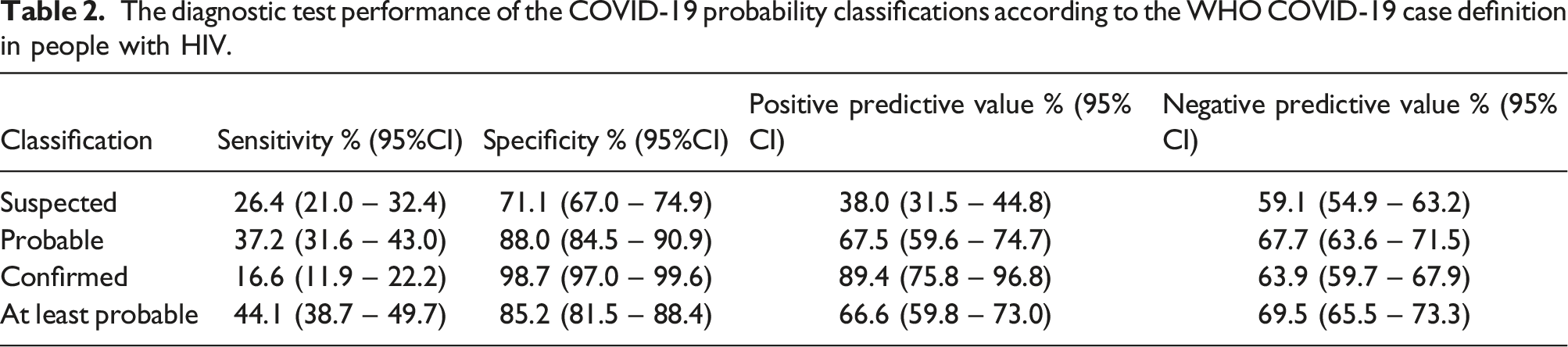
The 971 included people with HIV were median 40 years, 38.8% women, 44.8% had prior AIDS, and 55.6% had comorbidities. SARS-CoV-2 seroprevalence was 40.1% (95%CI:37.0–43.1) and 20.5% (95%CI:18.0–23.1) had clinical COVID-19 median 4 months (IQR:2–7) before inclusion. Clinical COVID-19 occurred less frequently in people with HIV with tuberculosis history, injecting drug use, CD4+ T-cells <200/mL and unemployment. The quality of life was not impacted after COVID-19. An at least probable COVID-19 classification by the WHO case definition had 44.1% sensitivity (95%CI:38.7–49.7), 85.2% specificity (95%CI:81.5–88.4), 66.6% positive predictive value (95%CI:59.8–73.0) and 69.5% negative predictive value (95%CI:65.5–73.3) to diagnose COVID-19.
Conclusions
COVID-19 unvaccinated people with HIV from Ukraine had a significant COVID-19 rate and using the WHO case definition had insufficient diagnostic accuracy to diagnose these cases. The lower burden in vulnerable people with HIV was unexpected but might reflect a shielding effect.
Introduction
People with HIV, particularly those immunocompromised, experience increased COVID-19 related mortality.1–3 It is therefore important to reliably identify COVID-19 in people with HIV. In resource limited settings, this is hampered by the limited availability of laboratory testing facilities. This creates challenges for clinicians caring for people with HIV to differentiate COVID-19 from pulmonary illnesses related to HIV and other respiratory viruses. Studies in HIV-endemic resource constrained settings showed a high COVID-19 prevalence.4,5 This supports the need to have adequate diagnostic tools available. Laboratory test independent algorithms to identify COVID-19 clinically were introduced by the World Health Organization (WHO) in 2020. 6 This WHO case definition has been widely implemented in resource limited HIV endemic settings. 7 Its diagnostic performance in people with HIV from HIV/COVID-19 co-endemic settings is however unclear.
HIV in Ukraine affects around 1% of the adult population and causes a high AIDS burden. The Ukraine HIV epidemic was centered in the east, with intravenous drug users as key population, but phylogenetically linked infections have increasingly occurred in central and west Ukraine since 2014. As a result of significant public COVID-19 vaccine hesitancy, a delayed initiation of COVID-19 vaccination from March 2021 onwards with a far more limited subsequent roll-out compared to the rest of Europe, the vast majority of people with HIV remained unvaccinated against COVID-19 prior to 2022. 8 Ukraine had limited public COVID-19 testing available leading to unreliable case load estimations and less stringent public countermeasures to stop COVID-19 from spreading, such as societal lockdowns. The two main aims of this study were to evaluate the COVID-19 point prevalence and to assess the diagnostic test characteristics of the WHO case definition for COVID-19 in a COVID-19 unvaccinated population of people with HIV from a low-middle income country without widespread available medical or societal COVID-19 countermeasures.
Methods
Design
We conducted a cross-sectional study including COVID-19 unvaccinated people with HIV ≥18 years in West-Ukraine between October 2020 and November 2021. Participants were recruited at the Lviv Regional Public Health Center, Pulmonary Health Center, and Astar Medical Center. These centers provide the HIV care in Lviv. People with HIV, regardless of COVID-19 symptoms, were consecutively approached for participation at routine HIV monitoring visits. SARS-CoV-2 laboratory diagnostics (PCR/rapid antigen test/serology) were considered standard of care as screen tests then, but were unavailable in these centers in routine care. With only data from routine care used, the ethical committee that approved the protocol waived the need for a written consent. All participants were informed on the use of their data and could opt out. The study was registered at https://clinicaltrials.gov NCT04711954.
Procedures
We used a case record form (CASTOR®) adapted from the Dutch ATHENA cohort and extracted data from the electronic patient files of the Ukrainian national HIV registry. People with HIV completed a questionnaire with their physician on current or prior COVID-19 symptoms since March 2020, risk exposures, reported SARS-CoV-2 test outcomes from other test clinics, medical history, socio-economic status (SES), and quality of life (equation (5D) questionnaire). After COVID-19 vaccinations became available, the vaccination status was added to the routine medical assessment by physicians. No longitudinal follow-up was done after inclusion. The assessment generated the data for the WHO case definition to classify the probability of a COVID-19 event as suspected, probable, or confirmed. We developed the protocol using the 2020 definition (supplementary files). 6 We used the updated 2022 definition for analysis except for the rapid diagnostic tests (unavailable) and kept any disclosed anosmia/ageusia as indicative of a probable case. Based on the medical information provided by the participant, the study physician made a presumptive clinical diagnosis of any potential current COVID-19 episode or COVID-19 episode that occurred prior to the inclusion.
A suspected COVID-19 case fit any of the following clinical criteria: (1) acute onset fever and cough, (2) acute onset of any three or more symptoms consistent with a viral disease (as defined by the WHO case definition). We assumed the required epidemiological criteria for a classification as suspected was always met given the pandemic status and absent lockdown measures. COVID-19 was also suspected with any severe acute respiratory illness requiring hospitalization. A probable COVID-19 case had a probable or confirmed COVID-19 case contact (or COVID-19 cluster link) and either fit the clinical criteria, had imaging suspected for COVID-19, reported anosmia/ageusia, or died from unexplained respiratory distress. Confirmed COVID-19 cases were people with HIV who disclosed a laboratory test confirming COVID-19. All other participants were classified as COVID-19 unsuspected.
Leftover serum taken at the routine HIV monitoring visit was stored and used to assess SARS-CoV-2 serology (Wantai SARS-CoV-2 antibody ELISA (Wantai Biological Pharmacy Enterprise Company, Beijing, China; provided as part of the study) retrospectively in batches to detect total immunoglobulin against the SARS-CoV-2 receptor binding domain according to the manufacturer’s protocol. There was no real-time serological confirmation of presumptive clinical COVID-19 diagnosis.
Outcomes
The primary endpoint was the clinical COVID-19 prevalence. A clinical COVID-19 case was defined as being SARS-CoV-2 seropositive with at least suspected COVID-19 according to the WHO case definition. We assessed the SARS-CoV-2 seroprevalence and clinical COVID-19 frequency. Medical and SES risk-factors for COVID-19 and quality of life following COVID-19 were assessed. The co-primary endpoint was the diagnostic test characteristics of the WHO case definition using the SARS-CoV-2 serology results as reference standard indicating prior SARS-CoV-2 infection in this COVID-19 unvaccinated population.
Statistical analysis
Means with standard deviation or 95% confidence intervals (95%CI) and medians with interquartile ranges were used. The clinical COVID-19 prevalence was defined by taking the number of clinical COVID-19 cases and the seroprevalence was defined by taking all SARS-CoV-2 seropositive people with HIV, and divide each by the total included number of people with HIV. Univariate and multivariable logistic regression was used to calculate odds ratios (OR) for clinical COVID-19 by sex, age (<30/30-50/>50 years), HIV transmission group, CD4+ T-cell count (<200/≥200 cells/mL), undetectable plasma HIV-RNA, history of tuberculosis, and comorbidities (none/≥1). We compared the SARS-CoV-2 seroprevalence and clinical COVID-19 frequency according to SES and quality of life domains with chisquare tests. The sensitivity, specificity, positive and negative predictive values were assessed of using the WHO case definition to diagnose COVID-19.
Results
Baseline characteristics
Baseline characteristics of the study population.
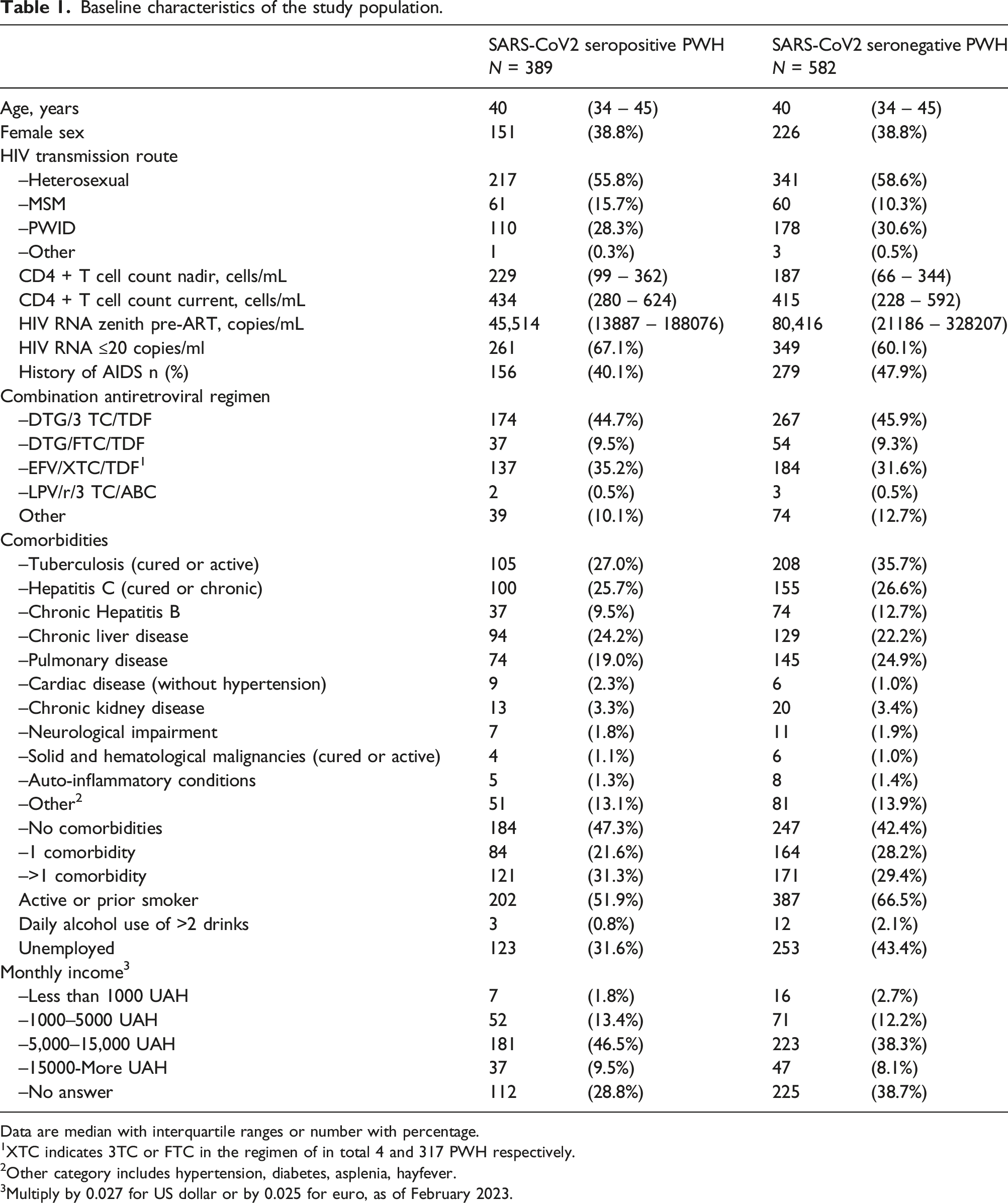
Data are median with interquartile ranges or number with percentage.
1XTC indicates 3TC or FTC in the regimen of in total 4 and 317 PWH respectively.
2Other category includes hypertension, diabetes, asplenia, hayfever.
3Multiply by 0.027 for US dollar or by 0.025 for euro, as of February 2023.
COVID-19 prevalence
A total of 199 SARS-CoV-2 seropositive people with HIV were classified according to the WHO case definition as having experienced suspected (29.6%), probable (52.3%) and confirmed (18.1%) COVID-19. The clinical COVID-19 prevalence was 20.5% (95%CI:18.0-23.1). The median time between the occurrence of at least a suspected COVID-19 and study inclusion with serology determined in these people with HIV was 4 months (IQR: 2-7). After adjustment, a history of tuberculosis (OR: 0.56, 95%CI:0.37-0.85) and injecting drug use (OR: 0.58, 95%CI:0.33-1.00 compared to being men having sex with men) remained associated with a lower risk of clinical COVID-19. Of the other variables, only a CD4+ T-cell count <200 cells/mL was associated with a lower risk of clinical COVID-19 in univariate (OR: 0.56, 95%CI:0.36-0.87) but not multivariate analysis (OR: 0.74, 95%CI:0.65-1.19). When restricting the analysis in a post-hoc defined multivariate model to anti-SARS-CoV-2 RBD seropositive people with HIV only, a history of tuberculosis remained associated with a lower risk of clinical COVID-19. Regarding SES, 595 participants were employed (61.3%) which was associated (p < .001 for both comparisons) with a higher SARS-CoV-2 seroprevalence (44.7% vs 34.3%) and more frequent clinical COVID-19 (24.9% vs 13.6%). Main occupational sectors were logistics (19.7%), management (11.9%), manufacturing (14.6%), medical/social care (11.9%), and 47.7% worked in other sectors. SARS-CoV-2 seropositivity and clinical COVID-19 rates did not differ significantly by occupational sector, social distancing at work, working with known SARS-CoV-2 infected colleagues, working from home, income level, or using public transportation. The equation (5D) scores on all domains (mobility, selfcare, usual activities, pain and discomfort, anxiety and depression, health score) were comparable between people with HIV with and without prior clinical COVID-19 and according to SARS-CoV-2 antibody serostatus.
WHO diagnostic algorithm
The diagnostic test performance of the COVID-19 probability classifications according to the WHO COVID-19 case definition in people with HIV.
Discussion
Almost 50% of COVID-19 unvaccinated people with HIV had COVID-19 by the end of 2021 in a resource limited setting of Lviv, Ukraine. This setting had limited public transmission countermeasures or laboratory surveillance of SARS-CoV-2 and had to rely on clinical algorithms to make presumptive COVID-19 diagnoses. The diagnostic test performance of the WHO case definition to identify or discard COVID-19 in this setting was however insufficient. The data indicated up to half asymptomatic SARS-CoV-2 infections and a lower odds of mentioning clinical signs or symptoms compatible with COVID-19 in more vulnerable people with HIV. The impact on the quality of life after mostly non-severe COVID-19 appeared limited.
The two main aims were to describe the COVID-19 epidemiology and evaluate the use of the WHO COVID-19 algorithm. The observed COVID-19 prevalence was in line with previous studies.2–4 We found that immunocompromised and people with HIV who inject drugs were less likely to have had clinical COVID-19. This might reflect shielding behavior in a setting with largely absent social distancing and lockdowns, unlike the settings in prior studies from South Africa and Western Europe. Another possibility is that SARS-CoV-2 transmission in people living with HIV became relatively enhanced amongst men having sex with men or those employed due to a higher rate of human interactions. These, and other sociobehavioural or cultural factors, might have played a role but were outside the study scope. Regarding the second aim, the WHO COVID-19 case definition had poor negative predictive value because of considerable asymptomatic SARS-CoV-2 infections. Atypically presenting SARS-CoV-2 infections not captured by the clinical algorithms could also have explained this. Nonetheless, this observation limits its use to exclude disease, relevant when aiming to prevent population transmission. Confirmatory testing is on the other hand also still required. Relying on this clinical algorithm alone to diagnose COVID-19 cannot steer clinical practice with sufficient certainty. This substantiates the WHO recommendation on its use. Our findings matched the performance of the WHO COVID-19 case definition in people without HIV. 9 Its use in practice was however heterogeneous, 7 especially in resource limited settings with absent confirmatory testing possibilities.
The limitations should be acknowledged. The COVID-19 prevalence in the Lviv region is unclear and could therefore not be used to put the observed prevalence in perspective. Emerging viral variants and population immunity have altered COVID-19 symptomatology which might limit generalization to the (post-)omicron era. SARS-CoV-2 antibody waning may have been possible but considered unlikely given the relatively short time between COVID-19 and sampling. Although the study overlapped partially with the start of COVID-19 vaccinations, the public roll-out including to people HIV was not prioritized and none of the participants disclosed receiving a COVID-19 vaccination. The influence of COVID-19 vaccination can therefore be considered negligible. PCR and rapid antigen tests would have strengthened the study but were unavailable. The retrospective nature introduced several biases including recall bias which makes firm conclusions impossible. We tried to mitigate this by having the same treating physicians who were trained uniformly to recognize signs and symptoms consistent with COVID-19 to guide participants through the questionnaire. Although not defined by the WHO, the clinical value of the WHO case definition arguably lies more in detecting acute SARS-CoV-2 infections. A study including people with HIV and recent SARS-CoV-2 infection would then add precision in evaluating its value. Furthermore, the algorithm was originally designed for public surveillance purposes. Case identification based on the symptomatology and epidemiological criteria is likely not different when the algorithm is used in clinical settings but this has not been formally assessed. The war escalation in 2022 prevented further analysis, including for example to assess possible selection bias of individuals who did not come to the centers for their care during the study period. Regarding strengths, this is the largest study in people with HIV to assess the WHO case definition, and the largest HIV/COVID-19 cohort from Ukraine. The study provides relevant data for clinical practice, which are otherwise scarce in Ukraine, and can help clinicians and policy makers to care for people with HIV with COVID-19 in low-middle income countries.
Conclusions
COVID-19 unvaccinated people with HIV from Ukraine were significantly affected by COVID-19 and the use of a clinical COVID-19 diagnostic algorithm had clear limitations to diagnose these cases. This highlights the need to supply HIV endemic low-middle income countries like Ukraine with resources for diagnostic testing during a pandemic.
Supplemental Material
Supplemental Material - COVID-19 epidemiology and performance of the WHO clinical algorithm to diagnose COVID-19 in people with HIV from Ukraine
Supplemental Material for COVID-19 epidemiology and performance of the WHO clinical algorithm to diagnose COVID-19 in people with HIV from Ukraine by Marta Vasylyev, Vira Buhiichyk, Nadiia Buhiichyck, Albert Groenendijk, Iryna Ben, Lesya Ostapiuk, Maryana Sluzhynska, Wouter F. W. Bierman, Jeroen J. A. van Kampen, Ferdinand W. N. M. Wit, Peter Reiss, Bart J. A. Rijnders, Oleksandra Sluzhynska, and Casper Rokx in International Journal of STD & AIDS
Footnotes
Acknowledgements
We thank all participants to this study and all colleagues in the Netherlands and Ukraine who helped making this study possible. The datasets used during the study are available on reasonable request to the first author and last author.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Unrestricted grant from ISS program by ViiV Healthcare (grant nr. 214,684) and the Erasmus MC Foundation aware.hiv Ukraine program (![]() ). The funder had no role in the design of the study, data collection, analysis, writing or the decision to submit for publication. The authors declare no other conflict of interest related to this submission. Results from a planned interim analysis at 500 participants have been presented at EACS conference London, 2021.
). The funder had no role in the design of the study, data collection, analysis, writing or the decision to submit for publication. The authors declare no other conflict of interest related to this submission. Results from a planned interim analysis at 500 participants have been presented at EACS conference London, 2021.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Erasmus MC Foundation (Aware HIV Ukraine - public fundraising); ViiV Healthcare; 214684.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.