
Abstract
Background
The COVID-19 pandemic disproportionately affected people of Black ethnicities, however, there are limited data on the post-acute sequelae of COVID-19 infection in these populations, and none in those with HIV.
Methods
We conducted a cross-sectional study in people of Black ethnicities with HIV in the UK. Participants were assessed for functional impairment, frailty, respiratory symptoms, anxiety and depression; they were also asked to rate aspects of their physical and mental health on a scale from 1 (poor) to 10 (excellent), both at enrolment and prior to the pandemic. We report associations with COVID-19 history and recovery status.
Results
We enrolled 183 participants between June 2021 and October 2022, 131 (72%) of whom reported COVID-19. A history of COVID-19 was associated with a reduced ability to carry out usual activities (OR 2.54 [1.03–6.21], p = 0.04), an increase in pain, tiredness and breathlessness, and overall decline in physical health. Of those with a history of COVID-19, 111 (85%) reported to have fully recovered. Those who had not fully recovered reported poorer functional status (p < 0.001) and had higher generalised anxiety scores (p = 0.02). Objective measures of physical function were similar in those who reported no COVID-19, COVID-19 with full recovery, and COVID-19 with incomplete recovery.
Conclusions
In this cohort of Black people with HIV, participants with a history of COVID-19 reported a reduced ability to carry out activities of daily living and various other health issues. Although most people reported full recovery from COVID-19, self-reported limitations in functional status and anxiety were common sequelae.
Keywords
Introduction
The post-acute sequelae of COVID-19 include physical, neurocognitive, and mental health impairments such as respiratory symptoms, pain, fatigue, sleep disturbance, depression and anxiety.1,2 Collectively, these multisystem sequelae are also known as long-COVID. 3 Large cohort studies have reported up to 1 in 5 adults develop long-COVID,4–6 predominantly following an initial SARS-CoV-2 infection (as compared to reinfection). 7 Long-COVID constitutes a significant public health burden, thought to affect at least 65 million individuals around the world8,9 and around 3% of the UK population. 10
Research into the pathogenesis and treatment of long-COVID is ongoing 11 including large clinical research studies such as the National Institutes of Health and Care Research “Researching COVID to Enhance Recovery (RECOVER)” program 12 in the general UK population. Pre-existing comorbidities have been linked to an increased risk of long-COVID including obesity,13–15 cardiovascular disease,4,14 kidney disease, 14 chronic lung disease, 15 diabetes, 16 depression and anxiety15,16 and dementia. 14 In addition to comorbidities, inflammatory markers, such as C-Reactive Protein (CRP), have also been shown to be persistently elevated in those with long-COVID and persist for up to 7 months post- acute infection. 17
The COVID-19 pandemic is known to have disproportionately affected people of Black ethnicities, with higher rates of COVID-19 acquisition, morbidity and mortality.18–20 Several studies have explored ethnic disparities in long-COVID.21–25 Results are mixed, with some studies demonstrating an increased prevalence of symptoms amongst people of Black ethnicity,21,23–26 and others failing to show an association.15,22 Research on long-COVID in these populations is needed to better understand the consequences of the pandemic in those who were most affected by it. 27
People living with HIV with poor immunovirological control are at increased risk of adverse COVID-19 outcomes.28–33 A global meta-analysis of 17 studies revealed that an estimated 52% of people living with HIV who reported a SARS-CoV-2 illness developed at least one long-COVID symptom. 34 Whilst previous studies have evaluated the impact of ethnicity or HIV status on long-COVID, to our knowledge, there are no studies which have explored the long-term sequelae of COVID-19 in people of Black ethnicities living with HIV. In the present study, we report on the long-term sequelae of COVID-19 in this population.
Methods
During routine HIV clinic visits between June 2021 and October 2022, people of Black ethnicities who had previously participated in the Genetic Determinants of Kidney Disease in People of African Ancestry with HIV (GEN-AFRICA) study (NCT05685810) were invited to take part in the COVID-AFRICA parent study (IRAS 294887), and a subset of these in the cross-sectional COVID-19 sequelae study. Enrolment into the COVID-19 sequelae was open to individuals irrespective of their COVID-19 history, however, we aimed for at least half of participants to have experienced COVID-19, and this data was gathered at the COVID-AFRICA parent study visit..
The study was approved by a National Health Service Research Ethics Committee (21/PR/0529) and the Health Research Authority (IRAS 295943). All participants provided written informed consent and received £10 cash for their time and effort.
Participants completed questionnaires evaluating their physical and mental health, functional status and well-being. They were asked to rate their current physical health, sleep, tiredness, pain, mobility, ability to independently self-care and carry out usual activities, memory, concentration and wellbeing on a 10-point scale ranging from 1 (poor) to 10 (excellent); they were additionally asked to rate these same factors just before the pandemic, to report current respiratory symptoms (cough, breathlessness, phlegm), and to complete assessments of their mental health (Patient Health Questionnaire-9 35 and Generalised Anxiety Disorder-7 score 36 ). Participants who had experienced COVID-19 were asked whether they had fully recovered or not.
We assessed physical status using the Clinical Frailty Score, 37 functional status, 38 and by measuring heart rate, respiratory rate, and oxygen saturations (breathing room air) at rest and after the one-minute sit-to-stand test, 39 and the 4-m gait speed. 40 Blood samples were obtained to measure CRP.
Statistical analyses
We described the characteristics of the study population, overall and stratified by COVID-19 (recovery) status, with comparisons using Pearson’s χ2 test (or exact tests where expected numbers were small) for categorical variables and Kruskal-Wallis test or analysis of variance for continuous variables, as appropriate.
We determined the proportions of participants who rated aspects of their physical and mental health lower at the time of enrolment, as compared to pre-pandemic. A ≥1 point decline was considered to be ‘any’ decline and a ≥2 point decline was considered to be a moderate-severe decline. Odds ratios (adjusted for age and sex) of the association of COVID-19 status with each outcome were calculated using logistic regression analysis.
We also compared physical status, respiratory symptoms and mental health, overall and stratified by COVID-19 and recovery status, using Pearson’s χ2 test/exact tests and Kruskal-Wallis tests, as above.
All analyses were performed using STATA v17 (StataCorp, College Station, TX). p values < 0.05 were considered significant.
Results
Demographic and clinical characteristics of the study participants stratified by COVID-19 status.
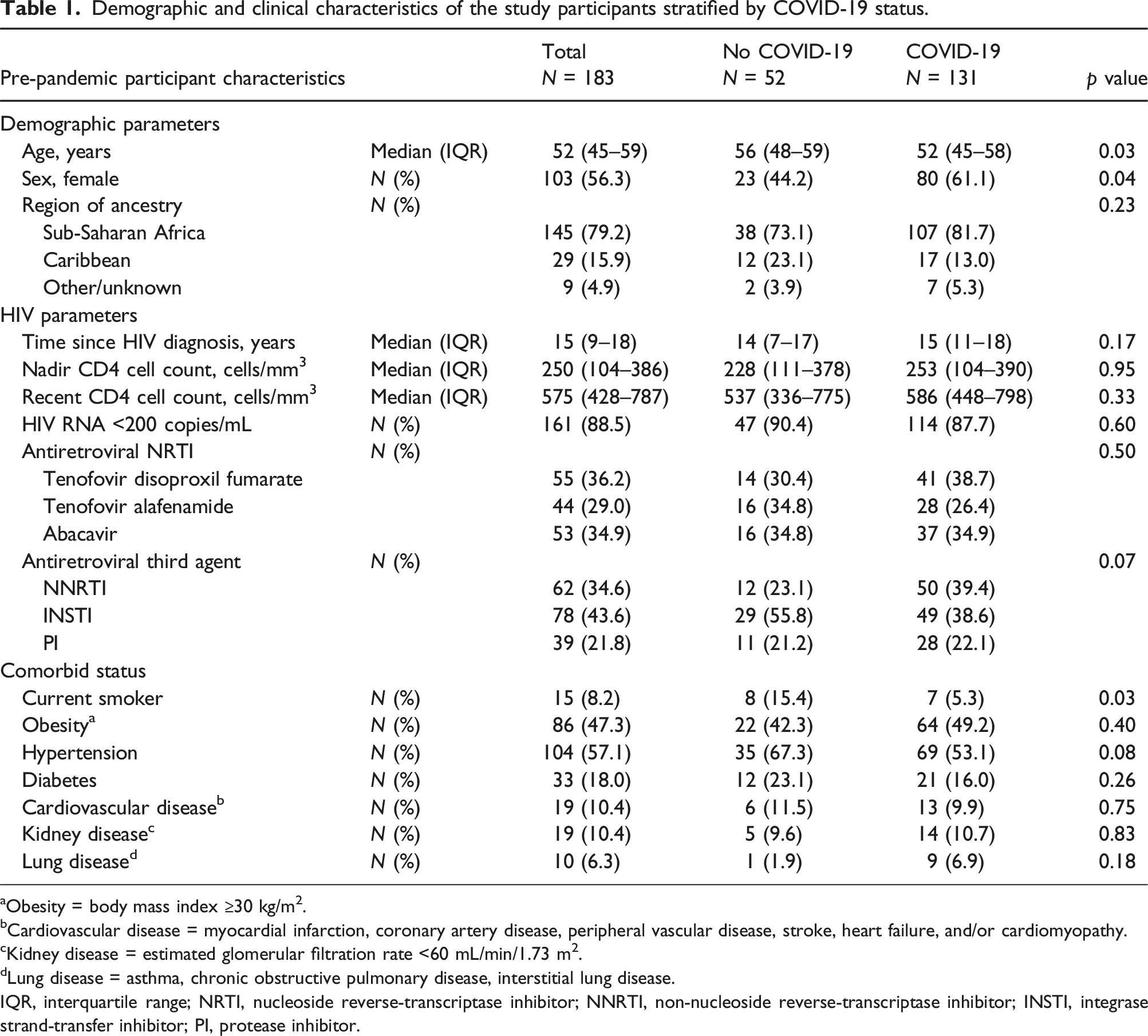
aObesity = body mass index ≥30 kg/m2.
bCardiovascular disease = myocardial infarction, coronary artery disease, peripheral vascular disease, stroke, heart failure, and/or cardiomyopathy.
cKidney disease = estimated glomerular filtration rate <60 mL/min/1.73 m2.
dLung disease = asthma, chronic obstructive pulmonary disease, interstitial lung disease.
IQR, interquartile range; NRTI, nucleoside reverse-transcriptase inhibitor; NNRTI, non-nucleoside reverse-transcriptase inhibitor; INSTI, integrase strand-transfer inhibitor; PI, protease inhibitor.
Changes in physical and mental health assessments, stratified by COVID-19 status and adjusted for age and sex a .
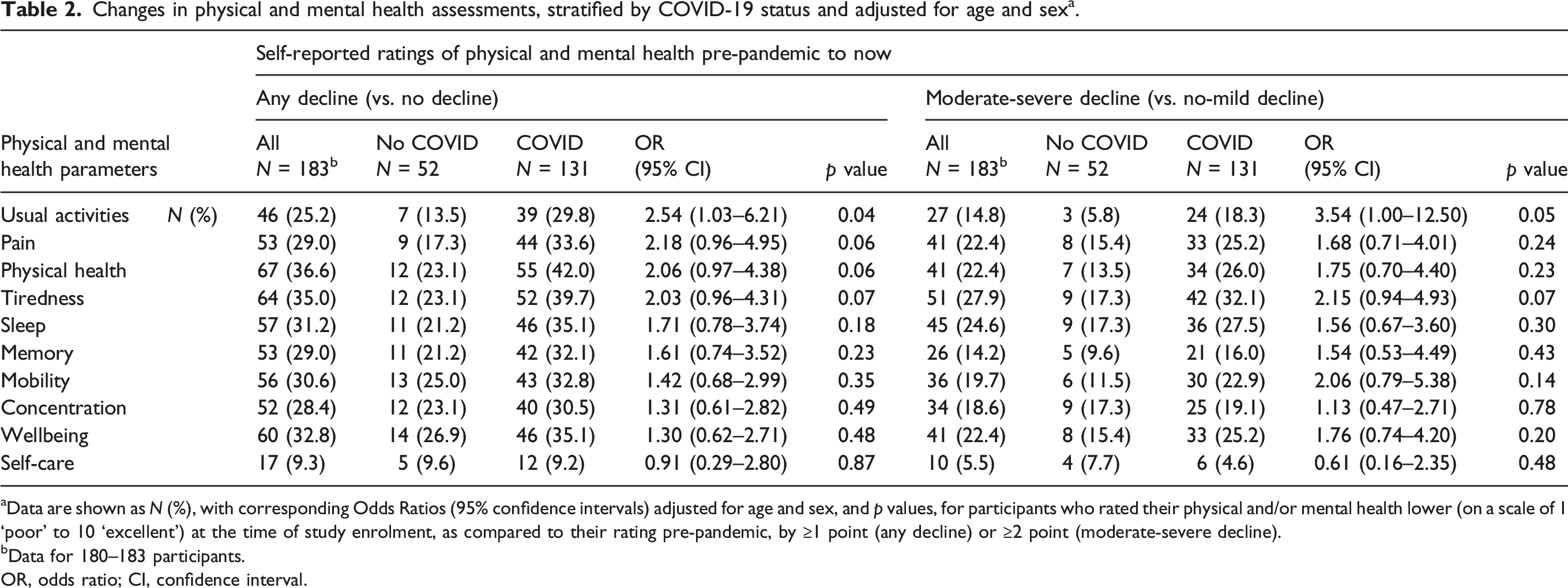
aData are shown as N (%), with corresponding Odds Ratios (95% confidence intervals) adjusted for age and sex, and p values, for participants who rated their physical and/or mental health lower (on a scale of 1 ‘poor’ to 10 ‘excellent’) at the time of study enrolment, as compared to their rating pre-pandemic, by ≥1 point (any decline) or ≥2 point (moderate-severe decline).
bData for 180–183 participants.
OR, odds ratio; CI, confidence interval.
Physical status, respiratory symptoms and mental health, stratified by COVID-19 status.
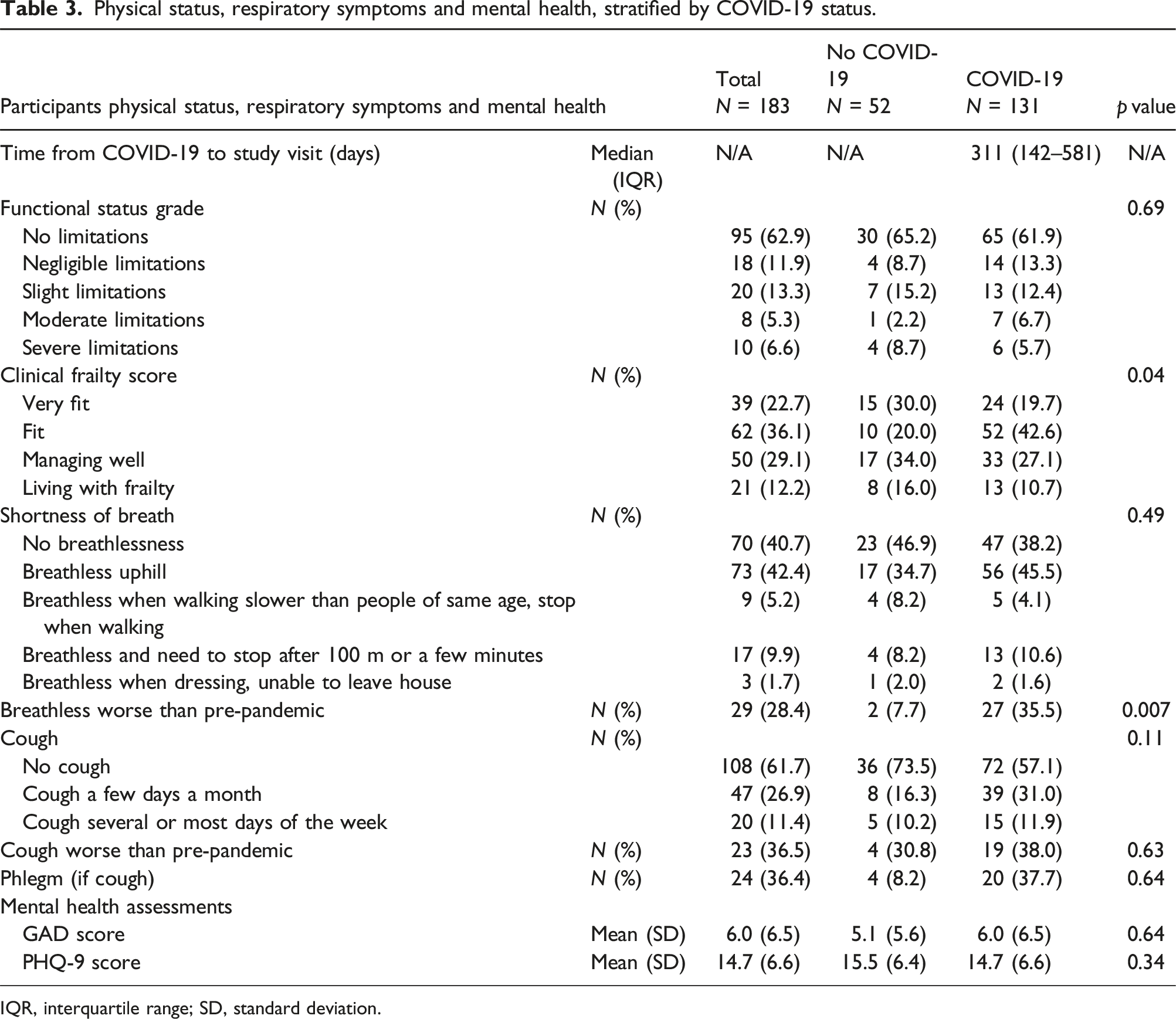
IQR, interquartile range; SD, standard deviation.
We also compared the characteristics and assessments for those who had, and those who had not, fully recovered from COVID-19. These two groups had similar demographic and clinical characteristics including age, nadir and current CD4 cell counts and proportions with suppressed HIV RNA (Table S1). Those who reported not to have fully recovered from COVID-19 had developed COVID-19 more recently (median 145 vs 354 days, p = 0.005) and were more likely to report that they were living with slight or moderate limitations in their functional status and frailty; they also had significantly higher anxiety scores, and this result was statistically significant (Table S2). An analysis restricted to participants who had experienced and fully recovered from COVID-19 in the preceding 12 months showed broadly similar results (Table S3).
Finally, there were no significant differences in effort tolerance, gait speed, respiratory rates, heart rates, and oxygen saturations (at rest or at the end of the one-minute sit-to-stand test), or in CRP levels among those not recovered from COVID-19, those who had recovered, and those without COVID-19 (Table S4).
Discussion
Our study evaluated sequelae of COVID-19 in a cohort of people of Black ethnicities living with HIV in UK. Even though 85% of participants reported full recovery from COVID-19 and most had well-controlled HIV, a history of COVID-19 was associated with a reduced ability to carry out activities of daily living, increased pain, tiredness and breathlessness, and overall decline in physical health. Our results suggest there may be a substantial burden of long-COVID in people of Black ethnicities with HIV.
Studies in the general population have similarly reported an association between COVID-19 and a reduced ability to carry out daily activities, 10 an increase in pain10,41 and a worsening of tiredness or fatigue.1,24,41,42 These studies43–45 also reported impairments of sleep, memory, mobility, wellbeing and concentration in participants who had COVID-19, but (as in our study) these associations did not achieve statistical significance. By contrast, the ability to self-care in our participants was unaffected by COVID-19, and the shorter time between the COVID-19 illness and the assessments in those not having fully recovered is in line with reports of a decline in the prevalence of long-COVID over time. 46
Approximately one third of participants with a history of COVID-19 reported breathlessness that was worse compared to prior to the pandemic. However, current levels of shortness of breath, and physical cardiorespiratory assessments at rest and post-exercise, were similar for those with and without COVID-19. Previous research of severe acute respiratory syndrome showed pulmonary changes on computed tomography reported up to 7 years after infection. 47 Other studies in the general population have also found breathlessness scales were above pre-COVID baselines in those with long-COVID1,10 with some studies focused on ethnic minorities, suggesting people of Black ethnicities with long-COVID may be more likely to experience dyspnoea as compared to other ethnic groups.24,25 Unfortunately, our study does not have objective, pre-pandemic assessment of cardio-respiratory function for comparison or radiological studies to evaluate for persistent lung parenchymal abnormalities.
Our results showing that incomplete recovery from COVID-19 was characterized by general functional impairments and (generally mild) frailty are consistent with previous reports.48,49 Our results are also in keeping with previous studies from the general population which show an increased rate of generalised anxiety disorder amongst those with long-COVID.1,48 One case-control study identified signs of neuroinflammation using CT-PET in individuals post COVID-19 and found those with motor slowing and persistent neuropsychiatric symptoms had higher translocator protein distribution volume (an index of gliosis and inflammatory change). 50 A metanalysis among people living with HIV reported the most common long-COVID symptoms to be neurological rather than respiratory. 34
Qualitative studies have previously explored the lived experiences of the COVID-19 pandemic, 51 including long-COVID,52,53 amongst Black populations with HIV and highlighted the worsening health and social inequalities due to the pandemic. Data show people of mixed ethnicity and those born outside the UK are less likely to be referred to long-COVID services, despite being more prone to experiencing symptoms.16,54 This highlights the need to ensure equitable access to long-COVID services, and targeted strategies to improve long-COVID outcomes amongst disadvantaged communities who may experience help-seeking barriers.53,55
The strengths of our study include the ethnic diversity of the Black study participants and the inclusion of all COVID-19 cases, regardless of severity. Our study is limited by its cross-sectional design, lack of follow-up visits and lack of young participants. It was designed and conducted before a consensus long-COVID definition, long-COVID subtypes and a validated symptom burden questionnaire were developed.42,56–58 Many of our outcomes were self-reported and subjective. Awareness of COVID-19 status may have impacted willingness to participate, influenced reported mental and physical health ratings, and the use of retrospective recall in the case of pre-pandemic health is duly acknowledged as a limitation. We sought to overcome this potential source of bias through the use of suitable response sets in the questionnaire (e.g., “ Did you feel affected by tiredness BEFORE the pandemic?”), as per recommendations for health-related COVID–19 research. 59
The changes in symptomology with different SARS-CoV-2 variants, following vaccination, and as the pandemic progressed are well documented anecdotally and in studies. 60 It is important to note our study was performed in 2021/22, when a significant number of people were admitted to hospital with severe lung infection secondary to SARS-CoV-2 (10% in this cohort). As a result, the long-COVID symptoms documented in our study may differ from symptom profiles reported in more recent years. 60 The modest sample size, resulting in limited power to detect statistical differences for some of the comparisons, along with no power analyses and the multiple outcomes examined, led us to focus on effect sizes (and consistency of these) rather than statistical significance per se.
In summary, in this study of people of Black ethnicities living with HIV in the UK, a history of COVID-19 was associated with a decline in physical and mental wellbeing. About 15% of those with COVID reported incomplete recovery and these individuals reported functional limitations, a degree of frailty, breathlessness and anxiety. Given our limitations, future studies with large sample sizes are needed to explore the pathophysiological mechanisms of long-COVID; such studies should include representation of ethnic minorities including those living with HIV to ensure equitable post-COVID healthcare for the most severely affected populations.
Supplemental Material
Supplemental Material - Post-acute sequelae of COVID-19 in people of Black ethnicities living with HIV in the United Kingdom
Supplemental Material - Post-acute sequelae of COVID-19 in people of Black ethnicities living with HIV in the United Kingdom by Zoe Ottaway, Lucy Campbell, Julie Fox, Fiona M. Burns, Lisa Hamzah, Sarah Schoeman, David Price, Amanda Clarke, Sarah L. Pett, Denis Onyango, Caroline Sabin, Robert F. Miller, Frank A. Post and on behalf of the COVID-AFRICA study group.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The COVID-AFRICA study was funded through a grant from Gilead Sciences (IN-UK-983-6053).
Ethical statement
Data Availability Statement
The database contains personal and sensitive information and is therefore not publicly available. Access to the study data and/or samples is governed by the National Health Service data access policy and those of King’s College Hospital NHS Foundation Trust, the study sponsor. The Gen-AFRICA and COVID-AFRICA studies are open to collaborations, and all requests from researchers who meet the criteria for access to fully anonymized patient level data will be considered. Concepts can be submitted for review to the principal investigator (Prof. Frank Post; email:
Supplemental Material
Supplemental material for this article is available online.
Appendix
COVID-AFRICA group: Study sites and staff
University Hospitals Sussex NHS Foundation Trust, University Hospitals Sussex NHS Foundation Trust, Brighton (Amanda Clarke [PI], Marion Campbell, Alyson Knott, Lisa Barbour, Vittorio Trevitt).
Chelsea and Westminster NHS, Chelsea and Westminster NHS Foundation Trust, London (Rachael Jones [PI], Alex Schoolmeesters, Shoreh Ghazali).
Guys and St Thomas’s NHS Foundation Trust, London (Julie Fox [PI], Anele Waters, Mariusz Racz, Louise Terry, Kathy Arbis).
King’s College Hospital NHS Foundation TrustLondon (Frank Post et al., King’s College Hospital NHS Foundation Trust, London (Frank Post [CI], Zoe Ottaway, Beatriz Santana-Suarez, Leigh McQueen, Lucy Campbell, Bee Barbini, Emily Wandolo, Rachel Hung, Luella Hanbury, Sarah Barber, Chris Taylor, Mary Poulton, Holly Middleditch, Itty Samuel, Candice McDonald, Vladimir Kolodin, Laura Cechin, Larissa Mulka, Amy John, Sally Hawkins, Madelaine Angus, Tim Appleby, Katherine Bainbridge, Hayley Cheetham, Julie Barker, Kate Childs, Rousell Roberts, Nivenjit Kaur, Lisa Shorrock, Kate El Bouzidi, Nisha Patel, Amelia Oliveira, Ayoma Ratnappuli, Kate Flanagan, Daniel Trotman, Nisha Mody, Michael Brady, Killian Quinn, Elizabeth Hamlyn, Gurjinder Sandhu, Verity Sullivan, Naomi Fitzgerald).
Leeds Teaching Hospitals NHS Trust, Leeds (Sarah Schoeman [PI], Gary Lamont, Natasha Calder-Smith, Tadas Mazeika, Kiran Chana).
North Manchester General Hospital, Manchester (Andrew Ustianowski [PI], Gabriella Lindergard, Jan Flaherty, Valerie George, Denise Kadiu, Alice Hendy, Kevin Kuriakose).
Mortimer Market Centre, Mortimer Market Centre; Central and North West London NHS Foundation Trust, London (Sarah Pett [PI], Mah Jabeen Qamar, Jose Paredes Sosa, Konstantina Tetorou, Michelle Beynon, Adesola Yinka-Ogunleye, Gosala Gopalakrishnan, Irfaan Maan, Claire Mullender).
Newcastle Hospitals NHS Foundation Trust et al., Newcastle Hospitals NHS Foundation Trust, Newcastle (David Ashley Price [PI], Bijal Patel, Ian McVittie).
Queen Elizabeth Hospital and Lewis, Queen Elizabeth Hospital, Woolwich; Lewisham and Greenwich NHS Trust, London (Stephen Kegg [PI], Chloe Saad, Rosa Harrington, Kirsty Cunningham, Mandy Lewis).
Royal Free London NHS Foundation TrustLondon (Fiona Burns et al., Royal Free London NHS Foundation Trust, London (Fiona Burns [PI], Jonathan Edwards, Tom Fernandez, Katie Spears).
St George’s University Hospital NHS Foundation Trust, London (Lisa Hamzah [PI], Catherine Cosgrove, Hannah Laurence, Ameen Rahman, Katie Toler).
University Hospital Lewisham, University Hospital Lewisham; Lewisham and Greenwich NHS Trust, London (Melanie Rosenvinge [PI], Claudia Adade, Shelley Campbell).
Africa Advocacy Foundation (Denis Onyango).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.