
Abstract
Background
Hepatitis B virus (HBV) disproportionately affects people at risk of HIV. Encounters for HIV post-exposure prophylaxis (PEP) create opportunities for HBV screening and prevention. We quantified HBV prevalence, susceptibility, and active/passive immunization use among patients seeking HIV PEP.
Methods
We conducted a retrospective chart review of patients requesting PEP at an academic hospital between 2001-2021 in Toronto, Canada. Patients were classified as HBV immune or susceptible based on laboratory tests. Among HBV-susceptible individuals, we quantified how often HBV vaccine and/or hepatitis B immune globulin (HBIG) were administered.
Results
We identified 2018 PEP episodes, 75.3% being for sexual exposures. Mean age was 33.6 years. Among 1593 (78.9%) participants with available HBV testing data, six (0.4%) tested HBsAg-positive. Of 2018 episodes, 56.8% were among HBV-immune and 19.8% among HBV-susceptible participants; 23.1% were among participants of unknown status. Of susceptible participants, 55 (13.8%) received HBIG and 143 (35.8%) received HBV vaccinations.
Conclusions
HBV prevalence was low but roughly one-fifth of patients seeking HIV PEP were HBV-susceptible. HBIG use was inconsistent with current guidelines, and a minority of HBV-susceptible individuals were vaccinated. More systematic HBV testing, increased HBV vaccination and more rational use of HBIG are needed in those seeking HIV PEP.
Introduction
Hepatitis B virus (HBV) poses a significant public health threat and is the leading cause of chronic liver disease worldwide. 1 HBV is a sexually transmitted and blood-borne virus transmitted through percutaneous and mucosal exposure to blood and body fluids such as vaginal secretions and semen.1–3 Shared mechanisms of transmission between HBV and HIV lead to overlapping populations at-risk for both infections, including people with multiple sexual partners; gay, bisexual and other men who have sex with men (GBM); and health care personnel prone to blood and body fluid exposures.3–6 Consequently, HBV infection is more common in populations most likely to seek HIV post-exposure prophylaxis (PEP). For instance, a 2016 Toronto-based cohort study found that 49.4% and 19.1% of GBM living with and without HIV, respectively, had previously tested HBV-positive. 7 Considering that exposures leading individuals to seek HIV PEP may also increase their risk of HBV infection, PEP-related healthcare encounters present an opportunity to simultaneously implement HBV screening and prevention strategies. Notably, many HIV PEP drugs have anti-HBV activity, including tenofovir disoproxil fumarate (TDF), tenofovir alafenamide (TAF), emtricitabine (FTC) and lamivudine (3TC), although these agents are seldom used as primary HBV prevention strategies.8,9
Current HBV prevention interventions include active immunization with HBV vaccine and passive immunization with hepatitis B immune globulin (HBIG). The Engerix-B recombinant HBV vaccine offers 99% seroprotection in healthy adults and 83–99% in GBM and others at risk of HBV (e.g. people in correctional facilities).10,11 HBV vaccination is recommended for all adults and children to decrease their risk of HBV infection. 11 In Canada, the HBV vaccine schedule varies between provinces, with doses given according to the 0-, 6- and 12-month, or 0-, 1- and 6-month schedule either starting at birth or in adolescence. 11 Any non-HBV-immune individuals should additionally begin the HBV vaccine series after a high-risk exposure. 11 Despite this, population-level HBV immunity remains incomplete. The 2023 Adult National Immunization Coverage Survey found that only 69.2% of Canadian adults had received at least one dose of HBV vaccine. 12 Among patients presenting to an HIV prevention clinic in Toronto, Canada, 22.2% were non-immune to HBV. 13 In a cohort of HIV pre-exposure prophylaxis (PrEP) users in Ontario, 15.2% of PrEP-experienced participants were non-HBV immune. 14 Further, among 855 sex workers in Vancouver, Canada, only 68.3% reported ever being HBV vaccinated. 15
Passive immunization using HBIG can be used as HBV PEP within 48 hours after an exposure. A randomized controlled trial of healthcare workers with accidental exposure to HBV-positive blood found that, among 56 participants given two doses of HBIG and 28 given both one dose of HBIG and one dose of the HBV vaccine, none became acutely HBV-positive. 16 In addition to being recommended for infants born to HBV-positive mothers, current Canadian guidelines also recommend HBIG if a person: 1) is an HBV vaccine nonresponder, 2) has only received one dose of the HBV vaccine, 3) is unvaccinated or 4) has anti-HBs antibody titre levels below 10, and sustains a percutaneous or mucosal exposure to HBV-containing blood/body fluids; this includes the sexual contacts of individuals with or at high risk of HBV infection. 11 Given the overlapping risks for HIV and HBV among many key populations, and the inclusion of people with multiple sexual partners in the definition of persons at high risk of HBV, this guidance suggests that many people seeking HIV PEP may warrant HBIG if not known to be HBV-immune, yet its use in this context is uncommon.
We explored the need for and uptake of HBV prevention interventions in a cohort of individuals seeking HIV PEP in Ontario. Our primary objective was to quantify HBV susceptibility among HIV PEP requesters. Secondary objectives were a) to assess adherence to current HBV prevention recommendations by estimating the frequency of HBV vaccination and HBIG administration among susceptible individuals, and b) to assess the prevalence of baseline HBV infection in the cohort.
Methods
Study overview
We conducted a retrospective chart review of patients seeking HIV PEP at St. Michael’s Hospital (SMH), an academic tertiary care hospital in Toronto, from January 1st, 2001, to December 31st, 2021, (inclusive). SMH is a major provider of HIV PEP services in Toronto, a large and diverse urban centre. 17
Participants
Our study included all individuals who received at least one dose of HIV PEP or requested PEP at SMH’s emergency department (ED) during the study period. Neonates prescribed PEP to prevent vertical HIV transmission were excluded. We obtained preliminary lists of individuals presenting to the ED with a triage complaint or diagnostic code related to HIV PEP. Eligible patients were then identified from among these lists using manual chart review.
Data collection
Trained study personnel extracted data from patient charts into a Research Electronic Data Capture (REDCap, Version 14.0.33) database, including demographic and clinical characteristics, exposure type, STBBI testing, vaccinations, PEP prescription details, clinical outcomes, and referrals to other services.
Data were extracted for as long as they were available in relation to a given PEP episode. After patients underwent preliminary assessment in the ED, they were typically referred for further assessment in the infectious diseases clinic within 1–7 days, and then instructed to undergo follow-up laboratory testing for up to 6 months (2001-2013) or 3 months (2013-2021) post-exposure in accordance with contemporaneous HIV PEP guidelines.18,19 However, adherence to recommended follow-up schedules has historically been poor, consistent with published experience from other PEP programs in the industrialized world.17,20,21
Laboratory data
We extracted all available laboratory results for hepatitis B surface antigen (HBsAg), hepatitis B surface antibody (HBsAb), and hepatitis B core antibody (HBcAb) during each participant’s period of PEP follow-up (3–6 months) from hospital charts. Serology was performed at SMH using chemiluminescent immunoassays on/after September 15th, 2014, or microparticle enzyme immunoassay if before September 15th, 2014. We further extracted HBV DNA viral loads, performed by in vitro nucleic acid amplification test at the Public Health Ontario Laboratory, when available in participant charts. We defined HBV susceptibility as an HBsAb titre ≤10IU/mL, in the context of a non-reactive HBcAb test when available. Active HBV infections were defined as either a reactive HBsAg test, a reactive HBcAb test plus a detectable HBV DNA level, a positive anti-HBc IgM, or based on self-reported chronic HBV if no HBV-related laboratory data were available. 3 Patients with HBsAb titre >10IU/mL were considered immune. 3
Data analysis
All statistical analysis was conducted using R version 4.4.1. We performed descriptive analyses of sociodemographic variables to characterize our cohort, using PEP episodes as the unit of analysis. For all subsequent analyses, we used the PEP episode as the unit of analysis, since patients could present for HIV PEP more than once and each presentation represents a separate opportunity for intervention. We further reported the number of participants who knew their partner’s HBV status. Among those receiving HIV PEP, we calculated the number of participants who received an HBV-active regimen.
We then reported the proportion of participants meeting the above definitions of HBV susceptibility and HBV infection, stratified by exposure type (sexual vs parenteral vs other/unknown), as well as the proportion of HBV-susceptible individuals who received the HBV vaccine and/or HBIG, stratified by HBV immune status.
Ethical approval
Approval was obtained from the Research Ethics Board (REB) of Unity Health Toronto prior to commencing study-related activities.
Results
Summary of PEP episodes.
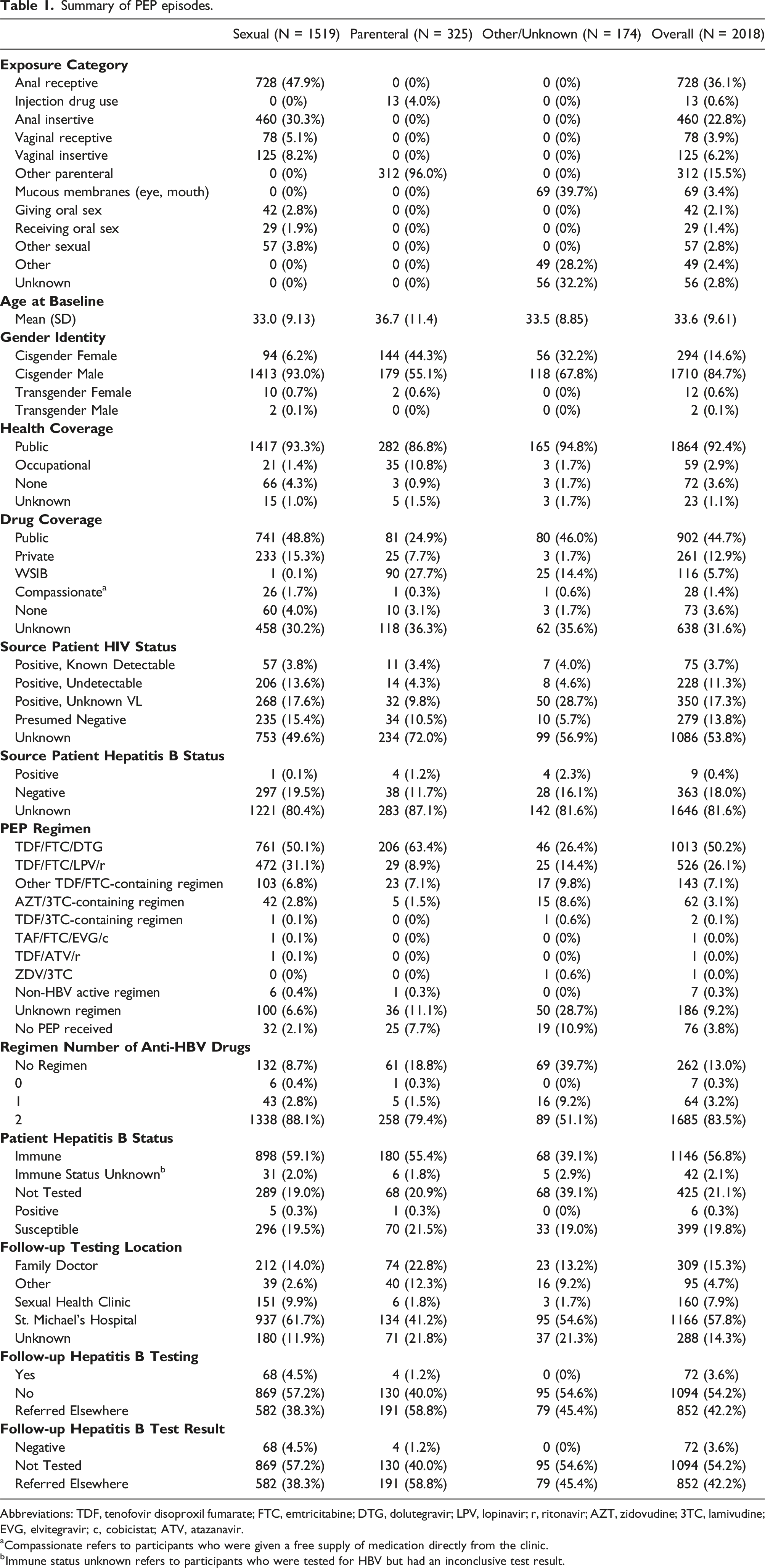
Abbreviations: TDF, tenofovir disoproxil fumarate; FTC, emtricitabine; DTG, dolutegravir; LPV, lopinavir; r, ritonavir; AZT, zidovudine; 3TC, lamivudine; EVG, elvitegravir; c, cobicistat; ATV, atazanavir.
aCompassionate refers to participants who were given a free supply of medication directly from the clinic.
bImmune status unknown refers to participants who were tested for HBV but had an inconclusive test result.
Of 1593 (78.9%) episodes with available HBV testing data, six (0.4%) had HBV infection at the time of presentation to the ED, demonstrated through a reactive HBsAg test (n = 6) and HBV DNA (n = 1).22,23 Five of these individuals presented due to a sexual exposure and one presented due to a parenteral exposure. All were known to be chronically HBV-positive prior to their PEP episode. Data on HBV immune status were unavailable in 467 (23.1%) episodes. Of all PEP episodes, 399 (19.8%) were in persons found to be susceptible to HBV; this proportion was similar for those presenting with sexual versus parenteral exposures (19.5% vs 21.5%).
Summary of hepatitis B interventions by immune status.

Note: Among nine participants with HBV-positive contacts, one received HBIG and the remaining eight did not receive an HBV vaccine or HBIG.
The proportion of participants who reported knowing the HBV status of the source person was low, at 19.6% among those reporting sexual exposures and 12.9% reporting parenteral exposures. Only nine exposures involved a known HBV-positive source. Among the nine corresponding exposed individuals, six were immune to HBV, one was susceptible and two had unknown immune status; none of these patients received the HBV vaccine or HBIG.
Follow-up was planned at SMH for 1166 episodes, at the participant’s family physician for 309 episodes, and at a sexual health clinic for 160 episodes; 383 had an unknown or other follow-up location. Of the participants instructed to return to SMH for follow-up testing, 72 (6.2%) were tested for HBV infection within 3–6 months of their initial PEP visit; none had acquired HBV infection, 11 (15.3%) tested HBV susceptible and 17 (23.6%) had an unknown HBV immune status.
Discussion
In this retrospective chart review quantifying HBV susceptibility among patients presenting to an urban academic hospital in Canada seeking HIV PEP, we found that 19.8% participants were susceptible to HBV, 56.8% were immune to HBV and 0.3% were HBV-positive at the time of presentation. Of 399 HBV-susceptible participants, 8 (2.0%) received HBIG alone, 96 (24.1%) received a dose of the HBV vaccine and 47 (11.8%) received both HBIG and the HBV vaccine, but 248 (62.2%) received no HBV-specific prevention measures. Further, nine exposures involved known HBV-positive contacts, including three where the exposed person was either HBV susceptible or HBV serostatus-unknown, yet HBIG and HBV vaccine were not administered. These findings suggest missed opportunities to conduct HBV screening and vaccination among people at elevated HBV risk and reveal inconsistencies in HBIG administration.
A sizeable proportion (23.1%) of participants in our cohort were lacking HBV serology data at baseline, underscoring the need for increased education to HIV PEP providers about the importance of HBV testing, as recommended by evidence-based PEP guidelines. 18 The relatively high level of HBV susceptibility among participants seeking HIV PEP in our analysis further demonstrates how such testing may identify opportunities for primary HBV prevention in the form of vaccination.
Our finding of 19.8% HBV susceptibility further indicates a greater need for HBV vaccine uptake among key populations at-risk for this oncogenic, chronic viral infection (e.g. GBM, sex workers and people who inject drugs).13,15,24 While a universal HBV vaccine program has been implemented in Canada since the 1990s, the nature of the HBV vaccine formulation and dosing, along with variability in vaccine schedules, contribute to suboptimal rates of HBV immunity. Notably, the HBV vaccine must be administered in two to three doses, but many patients do not return for subsequent healthcare visits and fail to complete the full vaccine series. 25 Since groups at high risk of HBV often experience systemic discrimination within the healthcare system and face barriers to healthcare access, engaging with key communities to improve vaccine accessibility is essential to overcoming this challenge. It is also noteworthy that 5–10% of immunocompetent adults will not mount an adequate immune response following HBV vaccination. 25 Newer HBV vaccines with improved immunogenicity profiles are emerging, notably, the tri-antigenic hepatitis B vaccine approved for Canadian use in 2022; a study of this new vaccine demonstrated 91.4% immunogenicity, compared to 76.5% for older HBV vaccines.11,26 While uptake of new vaccines will contribute to improved HBV immunity in the future, performing post-immunization serology in groups at high-risk of acquiring HBV may further address the issue of vaccine non-response. 11 This advice provides further justification for conducting HBV screening among those presenting for HIV PEP.
Engaging primary healthcare providers in HBV awareness and prevention strategies may also help increase HBV immunity rates and improve vaccine uptake, likely through routinization of sexual health and STBBI discussions using destigmatizing approaches.27,28 Physicians performing HIV PEP follow-up visits should additionally ensure they test patients for HBV, ideally at baseline and 3-month visits. 29 The low rate of clinical follow-up observed in our cohort, while similar to that observed in other PEP programs, emphasizes that there is much room for improvement in this facet of PEP care.17,20,21 Attention to HBV testing and prevention interventions in the context of HIV PEP is further important as PEP users often transition to tenofovir-based HIV PrEP, at which time it is essential to know patients’ HBV status before starting PrEP to minimize the risk of triggering hepatitis flares when therapy is interrupted. 18
While most participants in our cohort were unsure of their partner or source person’s HBV status, nine encounters involved a known HBV-positive source, including three among HBV-susceptible or immune status-unknown patients. None of these three individuals received HBIG or the HBV vaccine, despite guideline recommendations for both in such a scenario. 11 Inconsistent administration of HBIG and the HBV vaccine as HBV PEP was also evident among HBV-susceptible participants exposed to partners of unknown HBV status in our cohort—a scenario in which both interventions are recommended if the partner is from a high-prevalence population or has multiple sexual partners. 11
This inconsistency raises questions about the true need for HBIG in the latter situation, given the clinical burden and cost associated with administering this blood product. A crude calculation suggests that even after a high-risk exposure (e.g. condomless receptive anal sex, for which the risk of HBV transmission from a positive partner is 0.97%) 30 to someone from a higher-burden population (e.g. GBM in whom estimated HBV prevalence in North America is 1.79%),31,32 the risk of HBV acquisition would be low at roughly 0.00017 per encounter. If HBIG lowers the risk of HBV acquisition by 57.1%,33–35 the risk in HBIG recipients would be roughly 0.000074 per sex act and the absolute risk reduction 0.000099. These estimates suggest that among GBM in North America who have condomless receptive anal sex with a partner of unknown HBV status, roughly 10,086 individuals would need to receive HBIG to prevent a single HBV infection (“number needed to prevent”). This high number raises questions about the practicality and cost-effectiveness of HBIG when the partner’s HBV status is unknown.
Fortunately, there is reason to believe the HIV PEP medications received by patients in our setting may protect against HBV infection. 36 One study found significantly fewer HBV infections among participants using daily oral TDF/FTC as HIV PrEP after they were followed for 3 months (1/240 PrEP users, vs 21/246 PrEP nonusers, p = .018). 8 Another study found that use of HBV-active antiretroviral therapy (ART) among HIV-positive participants was negatively associated with HBV infection (hazard ratio = 0.4, 95% CI = 0.2–0.6); these results were mirrored in an African study, which found incident HBV infections decreased from 2.3/100 person-years among those not taking HIV ART, to 0.49/100 person-years among those on ART.36,37 While the magnitude of potential HBV prevention benefit from a 28-day course of HIV PEP is unknown, these data suggest that HBV infection risk may already be mitigated by the antiviral effects of HBV PEP. We thus propose that HBIG use in individuals seeking HIV PEP be restricted to those with confirmed exposure to a known HBV-positive contact, and otherwise be phased out of use in this setting.8,36
Simple quality improvement interventions could help boost HBV vaccination rates in the context of HIV PEP encounters and are being considered at our institution. For example, automated reminders could be programmed into digital systems, prompting clinicians to assess HBV susceptibility as part of routine ‘order sets’ for HIV PEP recipients, and reminding them to recommend vaccination to those who are non-immune. Educational materials for PEP recipients could be enhanced with information about HBV immunization and other sexual health vaccines, empowering patients themselves to inquire about their eligibility. Further accompanying such interventions with training sessions for relevant emergency department and infectious diseases clinic staff as well as formal audit/feedback interventions could also be considered. Explicitly identifying HBV vaccine uptake as a quality indicator in this population could further enhance efforts and provide formal mechanisms for evaluating progress over time using time series analysis.
This study is not without limitations. Data were collected through retrospective chart review, meaning that relevant laboratory data were unavailable for roughly 20% of participants. However, our relatively large sample size suggests that our HBV prevalence and susceptibility estimates are likely to be reliable. Similarly, our data do not capture participants who may have received HBV-preventive interventions at follow-up visits with clinicians outside our institution, such as the primary care providers and sexual health clinics to which many participants were discharged. However, HBIG is a blood product that is rarely given outside of hospital settings, and any such decoupling of HBV vaccine administration from HIV PEP care may still represent a missed opportunity for intervention. Finally, our sample was largely comprised of middle-aged, cisgender men who presented for PEP due to condomless anal sex, thus limiting generalizability of our results to other populations.
This 20-year chart review highlights the need for greater awareness and thoughtful uptake of HBV screening and prevention interventions among persons requesting HIV PEP. Any healthcare encounter related to sexual health should ideally be harnessed to promote comprehensive preventive care for all STBBIs.
Footnotes
Acknowledgements
The authors would like to thank Shreya Khera, Matthew W McGarrity and Oscar J Pico-Espinosa for their assistance in study supervision, and the Options Lab staff and trainees for their support. This work was conducted on the traditional lands of the Mississaugas of the Credit, Haudenosaunee, Anishinaabe, Chippewa, and Wendat Peoples. We are grateful to live, learn and play on these lands and are committed to moving forward with the spirit of Truth and Reconciliation.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DHST’s institution has received support from Abbott and Gilead for investigator-initiated research grants and from GlaxoSmithKline for industry-sponsored clinical trials.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DHST is supported by a Tier 2 Canada Research Chair in HIV Prevention and STI Research. This work was supported by funding from the Canadian Institutes of Health Research (FRN 155346).