
Abstract
Background
Adherence to antiretroviral therapy (ART) remains a challenge for many people with HIV and was exacerbated during the COVID-19 pandemic. This paper examines factors associated with ART adherence among people with HIV who inject drugs (PWHWID) in Almaty, Kazakhstan during the COVID-19 pandemic.
Methods
A cross-sectional survey was conducted from October 2020 to August 2022 with 66 PWHWID and their treatment support partners (n = 66) to assess associations between ART adherence and sociodemographic, COVID-19 related, social support, and other factors. Multilevel generalized linear mixed models were used to examine factors associated with optimal (≥90%) and standard (≥80%) adherence levels.
Results
We found low medication adherence rates: only 55.8% took ≥80% of their doses, and just 14.7% took ≥90%. People were more likely to take their medication consistently if they had a partner with HIV, experienced less household conflict during COVID-19, or met with addiction professionals. Poor mental health and negative emotional impacts from COVID-19 were associated with low adherence.
Conclusion
These findings suggest that HIV treatment programs should consider the importance of patients’ relationship factors, mental health, and home environment impacts during public health crises.
Introduction
One of the key factors to achieve viral suppression within the UNAIDS 95-95-95 strategy for people with HIV (PWH) is antiretroviral therapy (ART) adherence. Viral suppression is key to improving population health (e.g., reduced HIV transmission, decreased drug resistance)1,2 and individual health (e.g., reduced morbidity and mortality).3,4 The COVID-19 pandemic may have made adherence more difficult, particularly in low- and middle-income countries (LMICs), through factors such as changes in healthcare access and social support. 5 The impacts were more severe for marginalized populations, such as people who inject drugs (PWID), resulting in disrupted addiction treatment and harm reduction services. 6
Kazakhstan has one of the fastest growing HIV epidemics globally, 7 driven primarily by drug injection, with over half of PWH acquiring HIV infection through this route. 8 Kazakhstan experienced several waves of lockdowns during the COVID-19 pandemic, which restricted access to healthcare services and overburdened healthcare systems. These changes resulted in altered social dynamics among PWID such as changes in drug use patterns and behaviors including isolation during drug use and shifts in drugs used leading to overdoses 9 ; alterations in the way PWID access and share drug injection equipment, potentially leading to increased risk of blood-borne infections like HIV and HCV 6 ; and disruptions in the illicit drug supply chain which may affect the availability, purity, and price of drugs. 10 Increasing and maintaining ART adherence among PWID in Kazakhstan, especially during public health crises, is critical to reducing the spread of HIV in the country. Yet there is limited research on factors associated with ART adherence among people with HIV who inject drugs (PWHWID) in Kazakhstan.
COVID-19-related factors that may impact ART adherence include increases in partner or family conflict, potential social isolation, and lack of social support. 11 The immediate environment, especially the household environment and close social circles, play a large role in creating a safe space and facilitating health promotion behaviors. During the COVID-19 lockdown periods, many individuals were confined to their households, and there was an increase in substance use and poor mental health, 12 all of which could adversely affect ART adherence. 13 During the COVID-19 pandemic, social relationships may have had an increased impact on medication adherence for PWH during this stressful period.
Understanding factors associated with ART adherence among PWID during public health crises is key to maintaining their health and reducing further spread of the virus when such crises inevitably arise in the future. Thus, the purpose of this paper was to examine multi-level factors (e.g., partner HIV status, employment, mental health, level of negative financial and emotional impact of the COVID-19 pandemic) associated with ART adherence during the COVID-19 pandemic among PWHWID in Kazakhstan.
Methods
Study design, Recruitment and procedures
Data are from the baseline survey of a study focused on adapting a dyad-based intervention for PWHWID to improve ART adherence. 14 This survey was conducted from October 2020 to August 2022 with 66 PWHWID and their treatment support partners (n = 66). An epidemiologist at the AIDS center reviewed patient records to determine which patients potentially met eligibility requirements (i.e., were diagnosed with HIV, on ART for ≥3 months, not virally suppressed, had a history of injection drug use). AIDS Center nurses informed potentially eligible patients about the study and screened interested individuals. After consent, nurses provided research staff from the Global Health Research Center of Central Asia (GHRCCA) with contact information. Research staff explained the study, answered questions, and conducted confirmatory screening and consent procedures. Eligible participants ('index cases') were asked to invite a treatment support partner (e.g., spouse/romantic partner, family member, friend) to participate. Screening and consent procedures were conducted separately with support partners.
The “index case” (partner initially recruited from the Almaty AIDS Center) must 1) have been diagnosed with HIV by the Almaty AIDS Center; 2) have been on ART for at least 3 months; 3) was not virally suppressed within the past year according to the AIDS Center medical records (≤500 copies/ml), and 4) have injected drugs in the past year. In addition, dyads were eligible to participate if both partners were 1) ≥18 years old; 2) both identified each other as their intimate partner, family member, friend, or other support person within their social network; 3) their relationship had existed for at least 3 months; 4) both reported feeling safe participating with their partner in the study; 5) neither reported any severe physical or sexual violence perpetrated by the other partner in the past year; 6) both were able to provide informed consent and follow study procedures; and 7) both were fluent in Russian. “Partners” may or may not have HIV and may or may not be a PWID. Upon enrollment, the research assistant (RA) sent participants a Qualtrics link to complete the baseline survey.
Measures
Surveys were administered to participants in Russian and contained items on socio-demographics, measures for ART adherence, access to HIV care, COVID-19 related factors, and medication specific social support.
Dependent variable-ART adherence
ART adherence was assessed using a standardized, brief medication adherence scale 15 which contains three items: 1) Days taken -- number of days the patient missed at least one dose of their medication (number of days, 0-30); and two five-point Likert items of 2) Frequency – how often the patient took ART in the past 30 days as prescribed (range: never to always); and 3) Rating – how good a job the patient did in taking their medication in the way they were supposed to in the past 30 days (range: very poor to excellent). Responses were then linearly transformed into a scale of 0–100 (higher scores indicate greater adherence). The average score across the three items was calculated to represent overall adherence. Scale reliability among this sample was high (Cronbach’s α = 0.90). Adherence cutoffs were analyzed at both the optimal (≥90%) and standard (≥80%) thresholds,16,17 with 90% adherence being our primary threshold. 18 With newer ART regimens, lower levels of ART adherence at 80% are sufficient to achieve viral suppression; thus, factors associated with an 80% threshold were examined as secondary outcomes.19,20
Independent variables
The independent variables for the index case included sociodemographic factors, including race/ethnicity, age, gender identity, employment status, having children, and HIV status (determined through medical record). For dyadic outcomes, we used scales and questionnaires to assess potential factors associated with ART adherence across the dyads and calculated the reliability of the scales in our sample. These scales included the Patient Clinic Relationship Scale to assess the participants' perceived quality of relationship with their health-care provider (α = 0.93) 21 ; Life Events Questionnaire to assess exposure to a broad range of potentially traumatic events ranging from home life, financial problems, to health concerns (α = 0.66)22,23; the Substance Abuse and Mental Illness Symptoms Screener (SAMISS) to assess mental health and substance use problems (α = 0.81)24–26; the Perceived Availability of Social Support Scale 27 to assess participants’ perceived availability of someone to provide support for different situations (α = 0.94) 28 ; and the HIV Treatment Related Knowledge Scale to measure HIV treatment knowledge about complex treatment issues such as adherence, side-effects, and drug resistance (α = 0.91). Additionally, COVID-19 questions were developed based on current Kazakh government COVID-19 related priorities and policies and included questions such as financial and emotional impacts of COVID-19. During the same time as this study, the Almaty AIDS Center was rolling out another program using home health nurses to try and improve ART adherence. We also asked participants if they had received a home visit from a nurse.
Analysis plan
The primary objective was to examine sociodemographic, social support, and COVID-19 related factors associated with achieving ≥90% adherence. We conducted descriptive analyses to examine the frequencies and distributions of variables. We conducted multilevel generalized linear mixed models using Bayesian estimation with weakly informative half-Cauchy priors 29 and a binary distribution that incorporated random effects for dyads to account for potential sources of within-dyad statistical correlations. Bayesian estimation has been shown to be superior to maximum likelihood estimation for studies with small sample size. 30 We first conducted bivariable analyses with each factor hypothesized to be related to adherence. We then checked for multicollinearity among variables. For variables that were highly collinear, only one variable was included in the model. Based on recommendations in the literature, factors significant at p ≤ .15 in the bivariable analyses were included in the multivariable model. 31 Significance for multivariable analyses were two-sided at the 0.05 level. Because some research indicates that 80% adherence is sufficient to achieve viral suppression and prevent drug resistance,19,20 we conducted secondary analyses to examine factors associated with ≥80% adherence using these same methods. Analyses were performed using the 'brms' 32 package in R v4.3.3. 33
Results
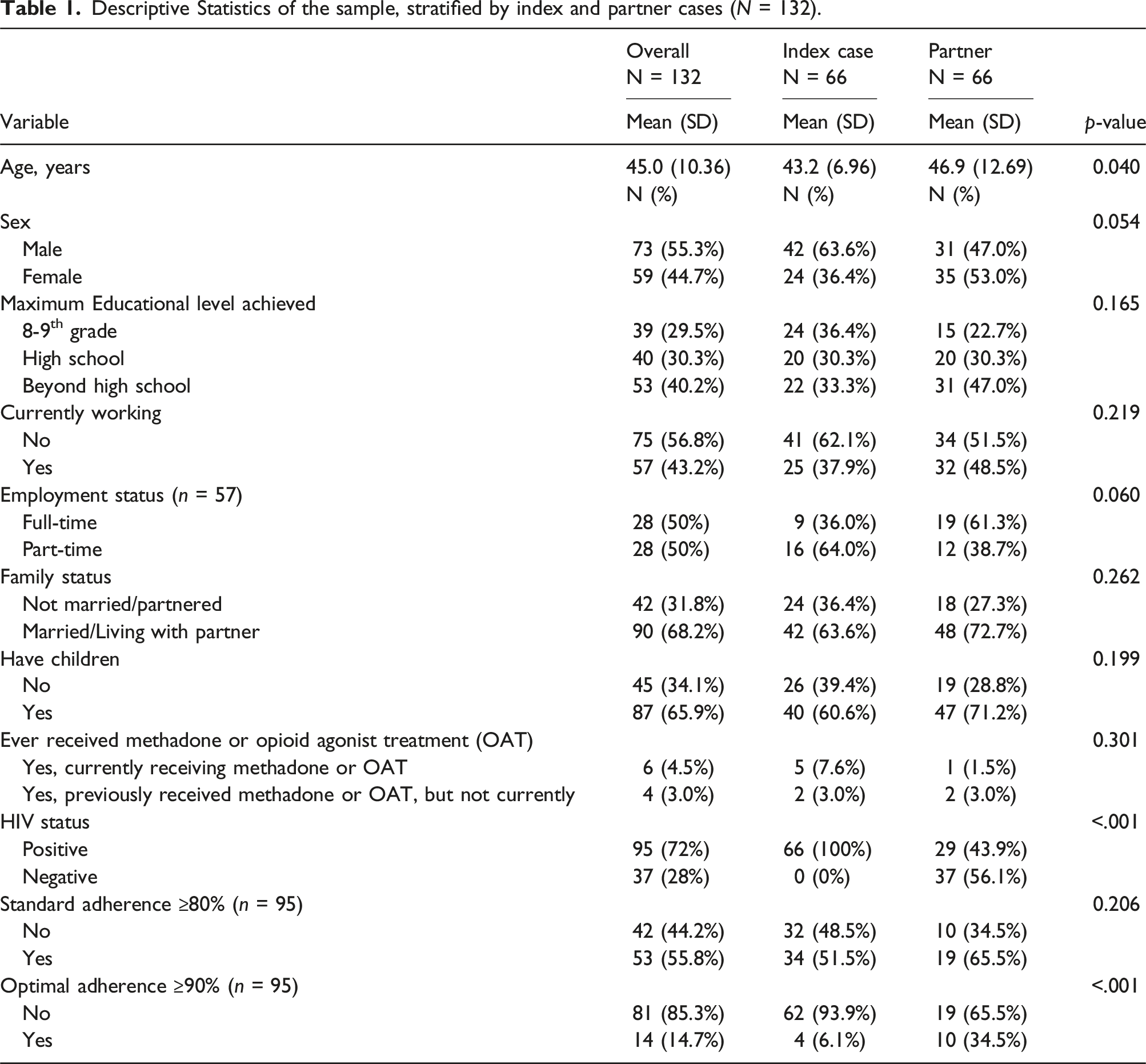
Descriptive Statistics of the sample, stratified by index and partner cases (N = 132).
Unadjusted and adjusted logistic regression for factors associated with optimal ≥90% adherence (N = 95).

aVariable was excluded from the multivariable model due to high multicollinearity with other variables in the model.
In the multivariable model, partner HIV status and conflict in the home due to COVID-19 were significantly associated with ≥90% adherence. The odds of achieving ≥90% adherence were nearly 15 times higher among participants who had partners with HIV compared to those who had partners without HIV (AOR = 14.94, 95% CI: 1.51-420.77, p = .02). Participants reporting decreased conflict at home during COVID-19 (compared to before COVID-19) had significantly higher odds of ≥90% adherence compared to those reporting the same or increased conflict (AOR = 22.77, 95% CI: 1.62-841.84, p = .02). Currently employed individuals had marginally higher odds of achieving ≥90% adherence (AOR = 4.36, 95% CI: 0.92-26.44, p = .07). Since the test only approached statistical significance, this finding should be cautiously interpreted as a potential statistical trend rather than conclusive evidence.
In the bivariate analysis (Table 3), being currently employed was associated with higher odds of ≥80% adherence (OR = 3.14, 95% CI: 1.11-11.22, p = .03). Conversely, having an AIDS center nurse deliver ART medications during COVID-19 (OR = 0.27, 95% CI: 0.08-0.77, p = .01), poorer mental health (OR = 0.13, 95% CI: 0.02-0.51, p < .001), higher HIV treatment knowledge (OR = 0.40, 95% CI: 0.15-0.93, p = .03), and experiencing more negative emotional impact due to COVID-19 (OR = 0.25, 95% CI: 0.07-0.74, p = .01) were associated with lower odds of ≥80% adherence.
Unadjusted and adjusted logistic regression for factors associated with standard ≥80% adherence (N = 95).
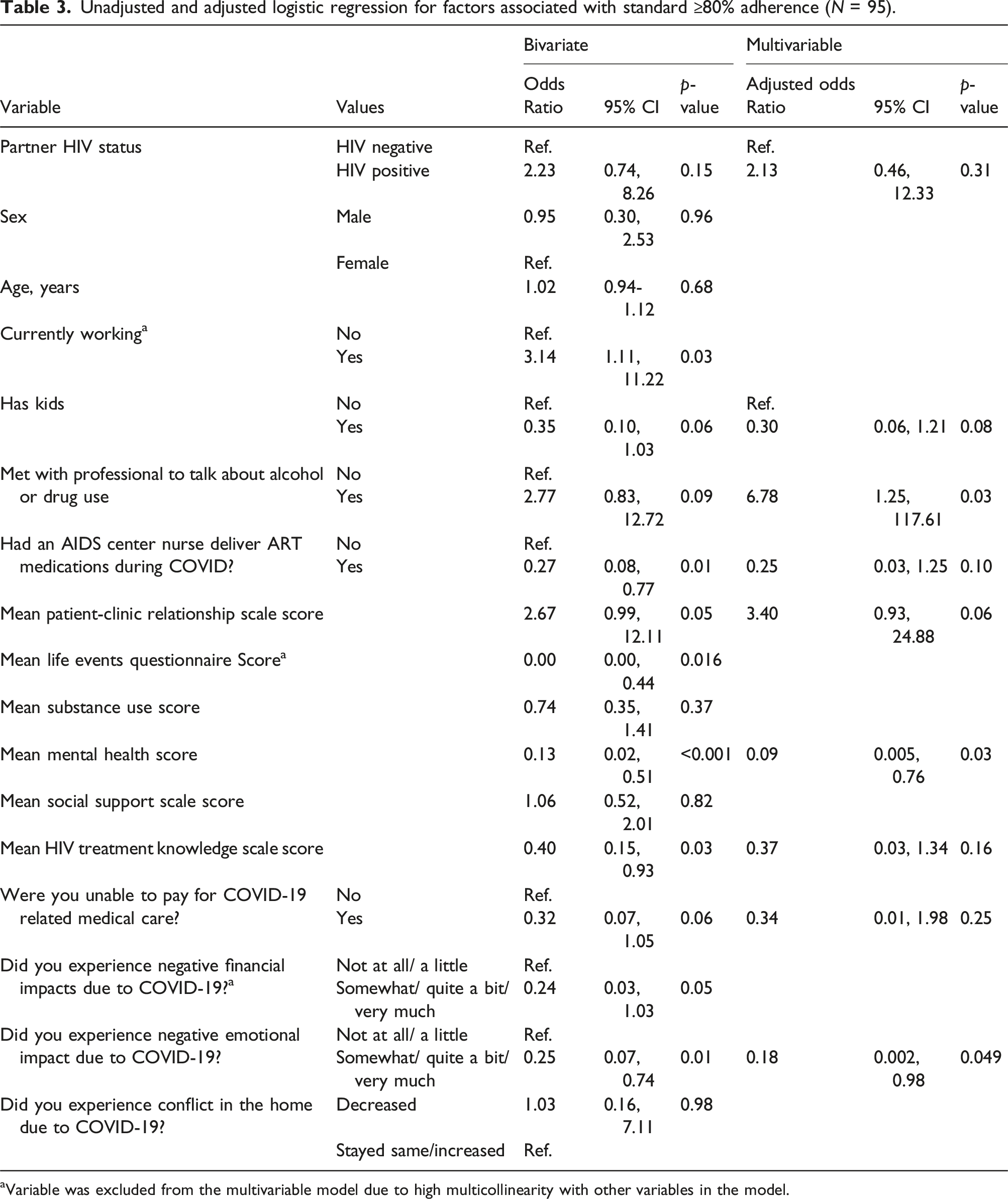
aVariable was excluded from the multivariable model due to high multicollinearity with other variables in the model.
Discussion
Adherence to ART is crucial for effective management of HIV, yet achieving high adherence rates remains challenging. This study aimed to identify factors associated with ART adherence among PWHWID and their treatment support partners during COVID-19 disruptions. An important finding is the association between having a partner with HIV and optimal (≥90%) ART adherence, suggesting the potentially important role of partner characteristics. There is limited data examining differences in support for ART adherence between partners with HIV and partners without HIV, particularly among PWHWID. Many studies have reported partners with HIV on ART may not necessarily provide support for adherence to each other.34–36 However, our findings suggest that among PWHWID, having a partner with HIV was associated with a greater likelihood of achieving ≥90% adherence. Partners with HIV may have aligned priorities, such as shared health-related responsibilities and the need to care for each other. Seroconcordant partnerships may have more open communication about their HIV status and treatment due to their shared treatment experience and understanding of ART adherence importance. This may increase their motivation to adhere to their medication schedule and provide direct support; better equipping them to overcome adherence challenges together. Further research is needed to clarify the relationship between partner HIV status and ART adherence across different populations and settings.
Given that partners can improve ART adherence, clinicians may wish to involve partners in treatment discussions, 37 though inclusion should depend on relationship quality. Research shows dyad-based interventions in clinic and community settings may be particularly effective in promoting shared responsibility for adherence. 38 These interventions can foster mutual accountability and provide a supportive environment for medication adherence. Dyad-based approaches may also address relationship dynamics that impact health behaviors, such as communication patterns and shared decision-making processes. By engaging both partners, these interventions can potentially create a more sustainable support system for long-term ART adherence. Future research should aim to identify best practices for further engaging partners in adherence support efforts to optimize treatment outcomes for PWH. This could involve exploring various models of partner involvement, from education and counseling to more intensive support roles. Researchers might consider investigating the effectiveness of different partner engagement strategies across diverse relationship types and cultural contexts. For those with support partners without HIV, providing additional information or skills-building activities on supporting their partner may help increase adherence. Educational initiatives could focus on enhancing understanding of HIV treatment, addressing misconceptions, and developing practical skills for supporting adherence. These efforts might also incorporate strategies for managing the emotional aspects of being in a serodiscordant relationship, which could indirectly benefit adherence by reducing stress and improving overall relationship quality.
Our findings suggest the importance of considering personal and family dynamics in achieving ART adherence during periods of mass disruption, such as during the COVID-19 pandemic. During public health crises, when external support systems may be disrupted, the stability and supportiveness of the home environment can play a crucial role in helping PWH maintain their medication regimens.39,40 Our results indicate that PWH living in household environments with increased conflict during COVID-19 had lower ART adherence. Identifying strategies to support families of PWH during times of public health crisis could be valuable for maintaining ART adherence. Such strategies could include counseling services (potentially via telehealth) to help families cope with crisis challenges, as well as financial assistance to ensure households can meet basic needs. Additionally, offering resources on maintaining healthy relationships and communication within the family could help create a more supportive environment for PWH. Such strategies may also help reduce the personal emotional impact of crises, which we found to be associated with adherence. By recognizing the significance of family support during public health emergencies, healthcare providers and policymakers can work towards creating a more comprehensive approach to HIV care that promotes optimal ART adherence.
Our results reveal significant associations between mental health, substance use treatment, and ART adherence among PWHWID. Notably, mental health issues, particularly depression and anxiety, can have a detrimental impact on medication adherence among PWH. 41 In addition, individuals who had engaged with a professional to discuss alcohol or drug use were more likely to achieve adherence. These findings emphasize the need for regular mental health screening and substance use interventions in supporting ART adherence. They suggest that integrating mental health services into HIV treatment programs and addressing substance use issues through professional help may have a positive spillover effect on medication adherence behaviors, possibly by improving overall health management skills or reducing substance-related barriers to adherence. These findings collectively emphasize the interconnectedness of mental health, substance use, and ART adherence, particularly in the context of external stressors like the COVID-19 pandemic.
There are limitations that should be noted. First, we have a small sample size of 66 dyads, and ≥90% adherence was a relatively rare outcome among this sample. Although we used Bayesian estimation to improve the precision of our estimates, the small sample size and rare outcome resulted in wide credible intervals. Additional research with larger sample sizes is needed to provide more precise estimates. Despite our small sample size, our findings point to the potential impact of public health crises on home environment factors, which could make ART adherence more challenging. Second, data are drawn from a cross-sectional survey, which precludes causality. We also relied on a measure of self-reported adherence, which can be subject to recall and social desirability bias. Self-reported data may overestimate adherence, which may obscure associations with different factors. However, even with self-reported adherence, very few responded that they had ≥90% adherence and only half had ≥80% adherence, suggesting that participants overall were not artificially inflating their adherence levels. Additionally, participants were PWID living with HIV in Almaty, Kazakhstan. Different factors may be associated with ART adherence in other populations, but our findings lend important insights into a novel population. Also, few scales have been validated in Russian, and it is not clear if Russian-speaking participants interpreted items similarly to English-speaking participants. While most scales exhibited good internal reliability in this sample (α > 0.80), the Life Events Questionnaire had less than ideal internal reliability. However, a lower alpha corresponds to higher measurement error, which causes coefficient attenuation (bias towards the null). Therefore, it is possible that improving the internal reliability of this scale (which was significant in only the bivariate model), would provide more accurate results and potentially a stronger association. Future scale development work among Russian-speaking PWHWID is needed.
In conclusion, this study sheds light on factors associated with adherence to ART among PWHWID in Kazakhstan during the COVID-19 pandemic. Treatment support partners, in particular partners living with HIV, may play a key role in promoting ART adherence. Decreased conflict in the home and lower levels of negative emotional impact during COVID-19 also facilitated adherence. Further research is needed to better understand how partner support may be leveraged to facilitate ART adherence among partners with diverse characteristics. Future studies should employ longitudinal designs with larger samples and use mixed-methods approaches to gain a more comprehensive understanding of the dynamic nature of adherence over time, particularly during periods of disruption. It may be beneficial for healthcare providers to assess social support systems, family and partner dynamics, and mental health when developing adherence support strategies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health; K01DA044853.