
Abstract
Background
Chlamydia trachomatis (CT) infections are prevalent and often asymptomatic. Point-of-Care (PoC) tests offer a diagnostic option. We described the incidence and predictors of CT infection using secondary data collected from men who have sex with men (MSM) and transgender women (TGW) attending Community-Based Organizations (CBOs) clinics in Thailand.
Methods
MSM and TGW aged ≥18 and had HIV risks were enrolled and followed for 12 months with visits every 3 months. Behavioral risks and Sexually Transmitted Infection testing were assessed at every visits. Specimens were collected via pharyngeal swab, urine sample, rectal swab, and neovaginal swab for TGW. These specimens were tested for CT using PoC test. The incidence was calculated using survival analysis, and the Cox regression model for multiple failures.
Results
From 2019–2021, 1886 participants were enrolled. Of these, 89.7% were MSM; 10.3% were TGW: 20.7% were lost to follow-up. Of the remaining participants, 18.2% had CT at baseline, with 36.4% experiencing repeat infections. The incidence rate of CT was 42.9 infections per 100 person-years. Predictors of CT infections included enrollment year, age 18–24 years, HIV status, pre-exposure prophylaxis and condom use.
Conclusion
Repeat CT infections were common. CBOs should incorporate POC STI testing into services, and the provision of STI prevention strategies.
Introduction
In the last decade, Thailand has implemented a number of HIV prevention strategies targeting key populations including men who have sex with men (MSM) and transgender women (TGW), with the goal of reducing new HIV infections. These strategies have been scaled up from 2014 to present. 1 The use of oral tenofovir disoproxil fumarate (TDF) alone or in combination with emtricitabine (FTC) as pre-exposure prophylaxis (PrEP) has proven to be highly effective for the prevention of HIV acquisition in MSM 2 and TGW. 3 The analysis of trends in HIV incidence among MSM and TGW attending a sexual health clinic in Bangkok from 2005 to 2018 shows that the increase in HIV prevention initiatives since 2014 was associated with a decline of HIV incidence from 5.4 per 100 Person-Year (PY) in 2009 to 3.0 per 100 PY in 2017. 4
Infection with Chlamydia trachomatis (CT) increase the risk of HIV transmission and Neisseria gonorrhoeae (NG) infection.4,5 Both infections are highly prevalent and often asymptomatic.4,5 A study in San Francisco, California, found that MSM with repeat NG or CT infections in the past 2 years had almost a 9-fold increased risk of incident HIV infection. 6 In Thailand, the prevalence of CT infection detected by laboratory-based nucleic acid amplification tests (NAAT) in MSM and TGW in Bangkok during 2006–2010 was 15.7% (95% Confidence Interval [CI]: 13.9, 17.6). 7 However, screening for CT using NAAT may be infeasible and costly in certain settings. Point-of-Care (POC) tests such as the Cepheid Xpert® CT/NG assay, a near-patient molecular test, which provides results in less than 90 minutes, 7 could be a viable option for CT and NG diagnosis. 9 This test has demonstrated a sensitivity of 100% and a specificity of 99%, regardless of the anatomical site. 9
In this analysis, we aimed to describe the incidence of CT infection and predictors of repeat CT infection among MSM and TGW attending the Community-Based Organizations (CBOs) clinics in Bangkok, Chiang Mai, and Chonburi provinces, Thailand, using results obtained from the Cepheid Xpert® CT/NG assay.
Methods
We conducted a secondary analysis using primary data collected from the prospective cohort study to evaluate the feasibility of integrating the point-of-care testing for sexually transmitted infections and HIV viral load (POC study) from MSM and TGW attending four CBOs clinics in Thailand (Service Workers IN Group (SWING) drop-in center (DIC), Bangkok; Rainbow Sky Association of Thailand (RSAT) DIC, Bangkok; SWING DIC, Chonburi; and M Plus DIC, Chiang Mai). A description of the POC has been previously published. 9 Eligibility criteria for inclusion in the POC included being a Thai national, men or transgender women who have sex with men, at least 18 years of age, had at least one of the following risks for HIV acquisition in the past 6 months: any unprotected sex; more than 5 sexual partners, regardless of condom use and serostatus; history of syphilis, chlamydia or gonorrhea diagnosed or treated; and any stimulant drug use; and being willing and able to provide written informed consent.
Study visit
Eligible participants were followed for a 12-month period. All participants had follow-up visits every 3 months. Additionally, participants who initiated PrEP (TDF 300 mg and FTC 200 mg) at entry visit had an extra follow-up visit at month 1. Those who were already using PrEP before the study did not require this additional visit. Behavioral risk during the previous 3 months was assessed using questionnaire at enrolment and every 3 months in all participants.
Risk reduction counseling and PrEP adherence
Counseling including risk reduction strategies and discussion on PrEP adherence for participants receiving PrEP, was conducted at every visits. Condoms and lubricants were provided to all participants.
STIs (Neisseria gonorrhoeae and Chlamydia trachomatis) testing
All participants underwent STI testing at every visit. Specimens were collected via pharyngeal swab, urine sample, rectal swab, and neovaginal swab for TGW (if applicable), regardless of reported sexual routes or symptoms. For the first 50 participants at baseline, in addition to NAAT testing, these specimens were also tested for Chlamydia trachomatis and Neisseria gonorrhoeae using the Cepheid Xpert® CT/NG POC testing. 7 Following the findings of Thammajaruk et al. (2023), specimens for CT and NG collected from the remaining participants and during follow-up were tested using a pooled sample method.
HIV testing
Participants with unknown HIV status were tested for HIV infection at the entry visit. For HIV-negative participants, HIV testing was conducted at every visit, and PrEP was offered at all visits. The HIV testing method depended on whether the participants received PrEP: participants not receiving PrEP underwent rapid HIV testing, which was the standard of care at all participating DICs; participants who already use or chose to start PrEP underwent both rapid HIV testing and Cepheid Xpert® POC HIV- 1 Viral load testing. For participants living with HIV, only Cepheid Xpert® POC HIV- 1 Viral load testing was performed. Additionally, at baseline, the first 50 participants who were either on PrEP or living with HIV also underwent 4th generation immunoassay and HIV-viral load testing at the Thai Red Cross Anonymous Clinic.
Participants with CT/NG detected by NAAT or Cepheid Xpert® POC CT/NG testing were treated in accordance with national and 2016 WHO guidelines for the management of these infections. Treatment was preferably provided on the same day the results were obtained. Participants enrolled in the study received a compensation of 500 Thai Baht (approximately 15 USD) per study visit to cover travel, meal expense, and loss of income.
Statistical analyses
We defined CT/NG infection as positive by the Cepheid Xpert® CT/ NG POC assay.
Frequencies and proportions were used to describe sociodemographic characteristics. Exact binomial 95% CI were calculated for CT prevalence estimates. Analysis of incident and repeat infection during follow-up visits were limited to participants who did not have evidence of CT infection at baseline. The minimum duration between episodes of CT infections in our sample was 17 days, which exceeds the standard 7-day treatment duration, suggesting reinfection was more likely rather than a treatment failure. 10 The incidence rate of CT infection was calculated using survival analysis, defined as repeat infections, during follow-up. Exact Poisson 95% CI was calculated for CT incidence per 100 PY.
As a result, we used the Andersen-Gill extension of the Cox regression model for multiple failures to evaluate and test predictors of CT infections. 11 Variables associated with CT infection with a p ≤ .10 in bivariate analysis were included in multivariable analysis, with likelihood ratio test and manual backward elimination approach used to determine variables to include in the final model. Statistical significance was evaluated using a two-sided p < 0.05. We performed all analyses using STATA® (Version 17, 2021, Stata Corp., College Station, Texas, USA).
Results
Participant characteristics at enrollment
We enrolled 1886 Thai MSM and TGW during 2019–2021 from four CBOs i.e. SWING Bangkok, RSAT Bangkok, SWING Pattaya; 186 M Plus Chiang Mai (Figure 1). Of the 1,886, 390 (20.7%) never returned for any follow-up visit after enrollment. Among these 390 participants lost to follow-up (LTFU), 332 (85.1%) had enrolled in 2020 or 2021, during COVID-19 outbreak in Thailand. The prevalence of CT infection among participants LTFU was 21.3% (83/390, 95% CI: 17.3, 25.7), which was significantly higher than the 18.2% prevalence among those who remained in the POC study (272/1,496, 95% CI: 16.2, 20.2). About one-third of CT infections at baseline were co-infected with NG (LTFU: 30.1% [25/83] v.s. Remaining 31.6% [86/272]; Figure 1). Participant Flow Diagram of Chlamydia trachomatis Infection among Thai Men who have Sex with Men and Transgender Women Participated in the Study to Evaluate the Feasibility of Integrating Point-of-care Testing for Sexually Transmitted Infections and HIV Into Community-based Clinics for MSM and TGW in Thailand” (POC project), Thailand, 2019–2021. 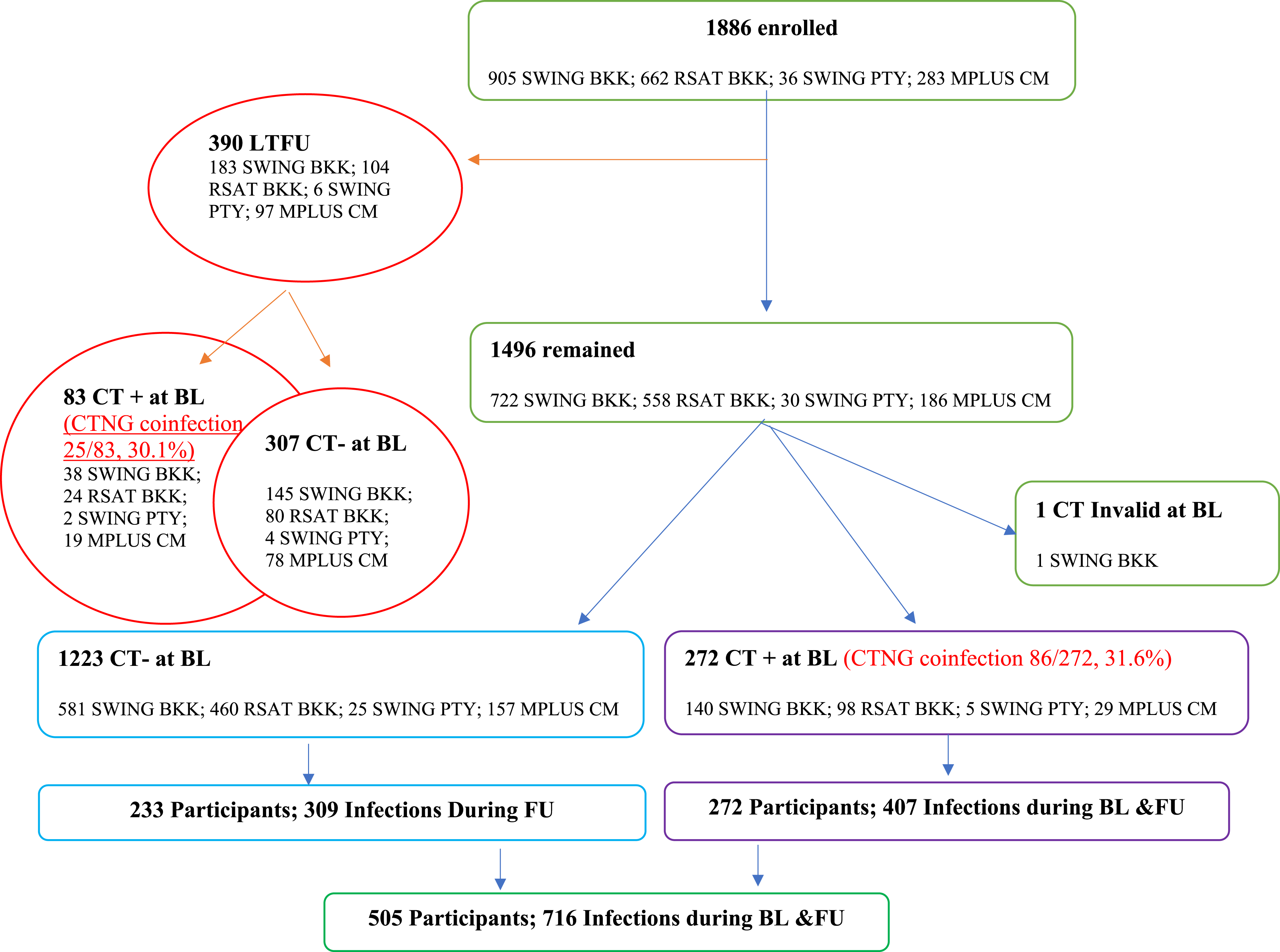
Socio-demographic Characteristics of Thai Men who have Sex with Men and Transgender Women Participated in the Study to Evaluate the Feasibility of Integrating Point-of-care Testing for Sexually Transmitted Infections and HIV Into Community-based Clinics, Thailand, 2019–2021.
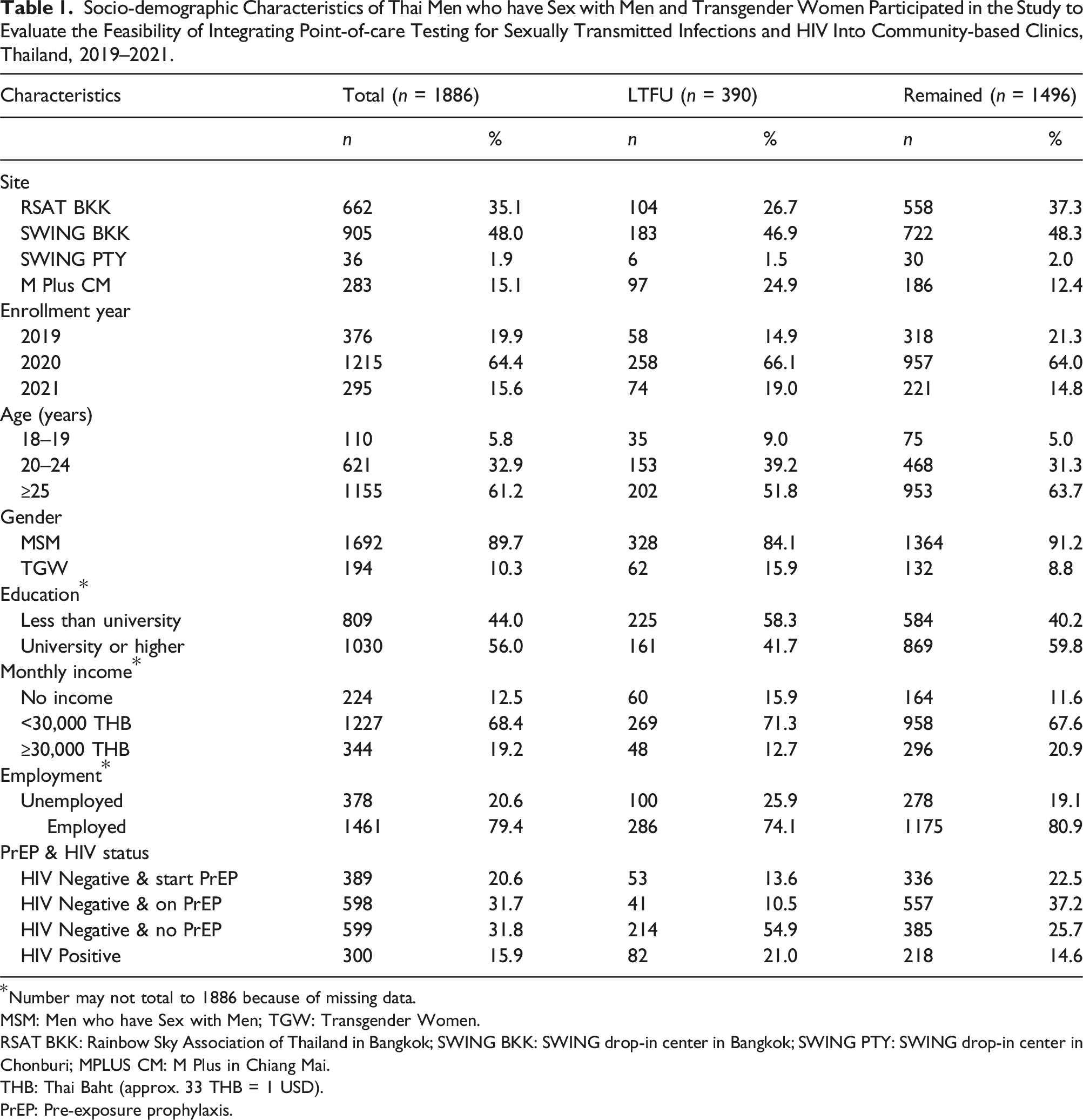
*Number may not total to 1886 because of missing data.
MSM: Men who have Sex with Men; TGW: Transgender Women.
RSAT BKK: Rainbow Sky Association of Thailand in Bangkok; SWING BKK: SWING drop-in center in Bangkok; SWING PTY: SWING drop-in center in Chonburi; MPLUS CM: M Plus in Chiang Mai.
THB: Thai Baht (approx. 33 THB = 1 USD).
PrEP: Pre-exposure prophylaxis.
Figure 2(a) presents the distribution of 505 participants with at least one CT infection, contributing to a total of 716 infections. The proportion of participants who were experienced repeat CT infections during follow-up was similar regardless of their CT infection status at baseline. After excluding participants lost to follow-up and one participant without a CT test result, 272 participants (18.2%, 95% CI: 16.3, 20.2) had a CT infection at baseline. Among these 272 participants, 99 (36.4%, 95% CI:30.7, 42.4) experienced repeat CT infections during follow-up period (Figure 2(b)). Among 1223 participants who were free of CT infection at baseline and attended at least one follow-up visit, 233 (19.0%) were diagnosed with CT infection at least once during follow-up, contributing to a total of 309 infections. Of these 233 participants, 62 (26.6%, 95% CI:21.0, 32.8) experienced repeat CT infections during follow-up period (Figure 2(c)). Number of Chlamydia trachomatis (CT) Infections at Baseline and During Follow-up Among All Participants (a), Participants 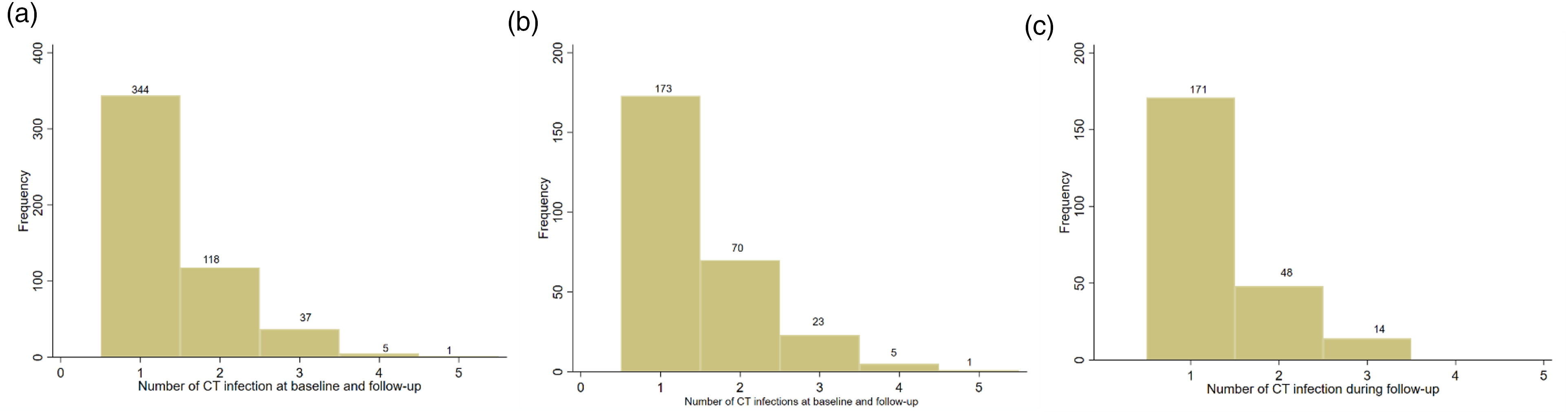
Predictors of Incident Chlamydia trachomatis Infections Among Thai Men who have Sex with Men and Transgender Women Participated in the Study to Evaluate the Feasibility of Integrating Point-of-care Testing for Sexually Transmitted Infections and HIV Into Community-based Clinics, Thailand, 2019–2021.
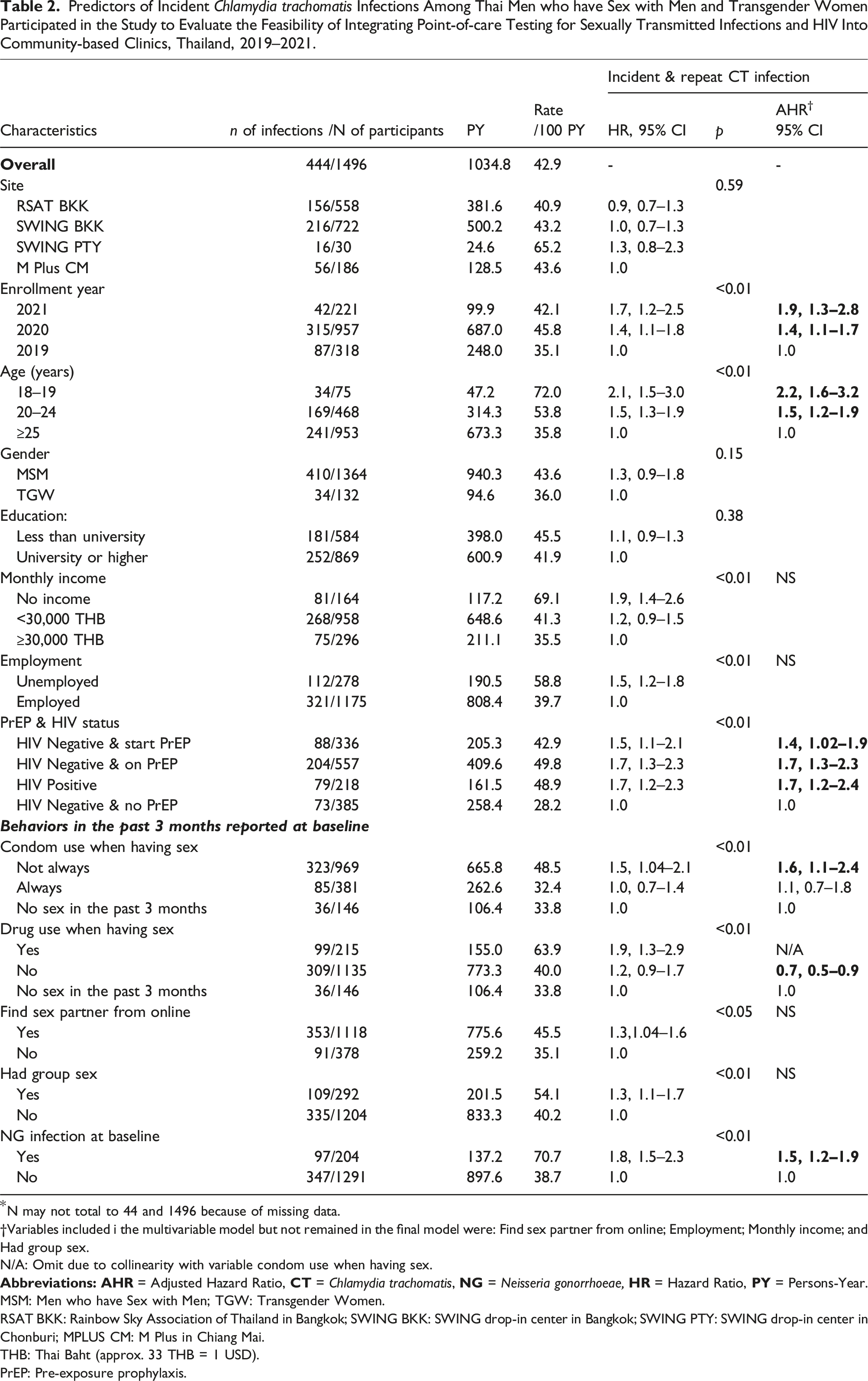
*N may not total to 44 and 1496 because of missing data.
†Variables included i the multivariable model but not remained in the final model were: Find sex partner from online; Employment; Monthly income; and Had group sex.
N/A: Omit due to collinearity with variable condom use when having sex.
MSM: Men who have Sex with Men; TGW: Transgender Women.
RSAT BKK: Rainbow Sky Association of Thailand in Bangkok; SWING BKK: SWING drop-in center in Bangkok; SWING PTY: SWING drop-in center in Chonburi; MPLUS CM: M Plus in Chiang Mai.
THB: Thai Baht (approx. 33 THB = 1 USD).
PrEP: Pre-exposure prophylaxis.
Factors associated with CT infections
In the final multivariable Cox regression model, factors significantly associated with repeat CT infection were: enrollment year (adjusted hazard ratio [AHR]:1.4, 95% CI 1.1, 1.8 for 2020; AHR: 1.9, 95% CI 1.3, 2.8 for 2021); age at enrollment (AHR: 2.2, 95% CI 1.6, 3.2 for 18–19 years; AHR: 1.5, 95% CI 1.2, 1.9 for 20–24 years); HIV status and PrEP use (AHR: 1.4, 95% CI 1.02, 1.9 for HIV negative & start PrEP; AHR: 1.7, 95% CI 1.3, 2.3 for HIV negative & on PrEP; AHR: 1.7, 95% CI 1.2, 2.4 for HIV positive); not using condoms when having sex (AHR 1.6, 95% CI 1.1–2.4); no drug use when having sex (AHR 0.7, 95% CI 0.5, 0.9). The incidence rate of repeat CT infection overall was 42.9 infections per 100 PY (95% CI 39.0, 47.1). When stratified by HIV status and PrEP use, the lowest incidence rate of CT infection was observed among HIV-negative participants not using PrEP, at 28.2 infections per 100 PY (95% CI 22.1, 35.5). Notable, the average PY per partipant declined sharply from 0.8 PY per participant in the 2019 enrollment year (248.0 PY/318 participants) to 0.4 PY per participant in the 2021 enrollment year (99.9 PY/221 participants) (Table 2).
Discussion
Our study found the incidence of repeat CT infections in sexually active MSM and TGW was substantial, with approximately 40% of MSM and TGW diagnosed with CT infection at least once each year, regardless of anatomical site. Nearly one-third of participants diagnosed with CT infection had repeat infection.
The CT prevalence among our POC study participants was slightly higher than the prevalence reported during 2006–2010 (15.7%, 95% CI: 13.9, 17.6). 8 The difference may be attributed to variations in participant profiles. Pattanasin et al. (2018) described MSM and TGW attending a sexual health clinic in Bangkok. But, the POC study participants were recruited from both Bangkok and tourist attraction provinces, such as Chiang Mai and Chonburi. Notably, participants enrolled in Pattaya, located in Chonburi province, had the highest CT incidence among all sites, indicating the presence of high-risk MSM and TGW in the study sample. For repeat CT infection, the estimate reported in this study (26.6%) was comparable to the 27.3% reported among a cohort of MSM and TGW who participated in the Test and Treat Cohort study conducted in five hospitals across Thailand (Bangkok, Lampang, Ubon Ratchathani, and Mahasarakham provinces) during 2012–2013, 12 prior to the implementation of PrEP in Thailand in 2014. 1
This study, to our knowledge, is the first to report CT incidence in MSM and TGW in Thailand. The CT incidence of about forty infections per 100 PY indicates a high prevalence in these populations if undiagnosed and untreated. To overcome challenges related to under-diagnosis, POC testing can be considered. The performance and feasibility of the Cepheid Xpert® CT/ NG POC assay, conducted by Key-Pop lay providers, has proven effective in detecting both CT and NG infections. 9 However, the high cost associated with the testing approach, which requires testing multiple anatomical sites (pharyngeal, urethral and rectal), can be a financial burden. A previous study found that CT is frequently detected in the rectum among Thai MSM and TGW. In settings where screening of all specimens is not feasible, rectal screening should be a priority. 8
We found that predictors associated with repeat CT infection included enrollment year, young age (<25 years), PrEP and HIV status, condom use during sex reported at baseline, drug use during sex reported at baseline, and NG infection at baseline. Additionally, the average PY per participant declined sharply from 0.8 PY per participant in the 2019 enrollment year to 0.4 PY per participant in the 2021 enrollment year. During 2020–2021, the COVID-19 pandemic arrived in Thailand, which was part of the worldwide pandemic of severe acute respiratory syndrome coronavirus 2 identified in 2019 (COVID-19 pandemic). From first detection through early January 2022, 2,420,000 COVID-19 cases have been confirmed in Thailand, with 22
We found that HIV-negative participants using PrEP had a higher incidence of CT infections compared to HIV-negative participants not using PrEP. This is consistent with findings from Weir et al. (2023), who enrolled participants from the same CBOs in Bangkok and Pattaya between 2017 and 2019. They also reported a high prevalence of CT, with higher CT incidence observed among participants using PrEP during the study. However, the incidence rate of CT among HIV-negative participants not using PrEP is still concerning, as it may reflect inconsistent condom use. This group remains vulnerable to both HIV and other STIs. In addition, although not statistically significant, the CT incidence rate among HIV-negative participants not using PrEP in our study was higher than that reported by Weir et al. (2023) for 2017–2019 (19.7 infections per 100 PY; 95% CI 14.3, 26.4), suggesting a potential upward trend in CT incidence within this vulnerable populations.
Our study had several limitations. Firstly, the reported incidence rates are likely underestimated, given that approximately 70% of LTFU participants who were HIV-negative and not using PrEP reported not using condoms during sex in the past 3 months. Secondly, it is challenging to determine whether these infections during follow-up were reinfections or persistent infection. However, given that the time between the first and the seconds infections exceeds the standard 7-day treatment duration, they are likely reinfections. By using the pooled testing strategy, site-specific infections could not be identified. However, the results obtained did not affect treatment options. Lastly, the sexual behaviors included in the bivariable, and multivariable analysis were those reported at baseline. Nonetheless, assuming no change in sexual behavior over the approximately one-year follow-up period may be reasonable.
In conclusion, our study demonstrated that repeat CT infections were common and associated with several factors. CBOs clinic providing STI testing for MSM and TGW should integrate the Cepheid Xpert CT/NG assay into routine STI screening and treatment services to enhance access to testing and care. This should be complemented with the provision of STI prevention strategies, such as condoms and PrEP, to support overall health and well-being.
Footnotes
Acknowledgements
The authors kindly acknowledge and are thankful for the support of the Rainbow Sky Association of Thailand (RSAT), and the Service Workers in Group Foundation (SWING), M Plus Foundation, and Institute of HIV Research and Innovation (IHRI).
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
We obtained written informed consent from all participants of the POC Study. The study was reviewed and approved by the Ethical Review Committee for Research in Human Subjects of the Faculty of Public Health, Mahidol University (MUPH 11/2025).