
Abstract
Background
We assessed the feasibility of point-of-care testing (POC) for Chlamydia trachomatis (CT) among Men who have Sex with Men (MSM) and Transgender Women (TGW) attending community-based clinics (CBOs) in Thailand.
Methods
A secondary analysis using data from a study that enrolled participants aged ≥18 years who were at risk of HIV. They were tested for CT and Neisseria gonorrhoeae (NG) using Cepheid Xpert® POC tests. Behaviors were assessed using a questionnaire. Logistic regression was used to evaluate factors associated with CT infections.
Results
A total of 1885 participants were enrolled between 2019 and 2021, with 89.7% identifying as MSM. Of all participants, 15.9% were living with HIV (PLHIV), 20.6% initiated PrEP, 31.7% were already using it, and 31.8% had never used PrEP.
Of all participants, 13.4% and 18.8% tested positive for NG and CT, respectively. CT prevalence was associated with age groups: 34.6% in 18–19 years (AOR 3.2), 24.1% in 20–24 years (AOR 1.7), compared to 14.5% in those ≥25 years. CT prevalence was higher in PLHIV (28.3%) compared to those who were HIV-negative and had never used PrEP (17.0%).
Conclusions
Almost one-fifth of Thai MSM and TGW had CT infection. POC testing is feasible and should be integrated into STI screening.
Background
Infections with Chlamydia trachomatis (CT), and Neisseria gonorrheae (NG) are increasingly prevalent sexually transmitted infections (STIs) that can facilitate both the acquisition and transmission of HIV. 1 A recent study among men who have sex with men (MSM) and trangender women (TGW) in Bangkok found that these infections are not only highly prevalent but also often asymptomatic.2,3 Routine screening and treatment for chlamydia, even in the absence of symptoms, are essential in preventing transmission.
The prevalence of CT infection detected by laboratory-based nucleic acid amplification tests (NAAT) in MSM and TGW in Bangkok during 2006–2010 was 15.7% (95% Confidence Interval [CI]: 13.9, 17.6). 3 Additionally, coinfection with CT and NG was approximately 3%. 2 However, screening for CT using NAAT may be unfeasible and costly in certain settings. Point-of-Care (POC) tests such as the Cepheid Xpert® CT/NG assay, a molecular POC test, which provides results in less than 90 minutes, could be a viable option for CT and NG diagnosis. 4 This test has demonstrated a sensitivity of 100% and a specificity of 99%, regardless of the anatomical site. 4
To address gaps in the diagnosis of CT and NG infections among MSM and TGW, the United States Agency for International Development funded a project titled Point-Of-Care testing for STIs and HIV in community-based clinics for MSM and TGW in Thailand, or the POC study. In this analysis, we aimed to describe the prevalence of CT infection and identify factors associated with CT infection among MSM and TGW who participated in the study conducted at Community-Based Organization (CBOs) clinics in Bangkok, Chiang Mai, and Chonburi provinces, Thailand, using results obtained from the Cepheid Xpert® CT/NG assay.
Methods
We conducted the secondary analysis using the primary data collected from the study to assess the feasibility of integrating point-of-care testing for sexually transmitted infections and HIV Viral Load (POC study), a longitudinal study with 3-month follow-up visits for a period of 12 months. The analysis presented in this manuscript included only the data collected at enrollment. The POC study recruited participants from MSM and TGW populations at four CBOs clinic sites in Thailand. These sites included the SWING drop-in center (DIC) in Bangkok and Chonburi, the Rainbow Sky Association of Thailand (RSAT) DICs in Bangkok, and the M Plus DIC in Chiang Mai. Details of the POC study have been previously described in Thammajaruk et al. (2023). The eligibility criteria for inclusion in the POC study required participants to be Thai nationals, identify as men or transgender women who have sex with men, be at least 18 years old, and have met at least one of the following HIV acquisition risk factors within the past 6 months: having engaged in sex without a condom, having had more than five sexual partners regardless of condom use or serostatus, having a history of syphilis, chlamydia or gonorrhea diagnosis or treatment, or having used any stimulant drug use. Additionally, participants needed to have been willing and able to provide written informed consent.
At enrollment, participants received HIV testing and counseling. Participants who tested HIV-negative were offered the option to initiate daily oral Pre-exposure prophylaxis (PrEP) (TDF 300 mg and FTC 200 mg) and were scheduled for an additional follow-up visit at month 1. Participants already using PrEP before the study were not required to attend an additional visit. Behavioral risk during the previous 3 months was assessed using a questionnaire at enrolment for all participants. Additionally, condoms and lubricants were provided to all participants.
STIs (Neisseria gonorrhoeae and Chlamydia trachomatis) testing
At each visit, all participants underwent STI testing. Specimens were collected using pharyngeal swabs, urine samples, rectal swabs, and neovaginal swabs for TGW (if applicable), regardless of reported sexual activities or symptoms. These samples were tested for Chlamydia trachomatis and Neisseria gonorrhoeae using the pooled method with the Cepheid Xpert® CT/NG POC test. For the first 50 participants, specimens were tested using both POC and laboratory-based NAAT methods for CT and NG. Based on the findings of Thammajaruk et al. (2023), specimens from the remaining participants were tested using only the pooled POC method.
HIV testing
The HIV testing method varied depending on whether participants were receiving PrEP. Those not using PrEP underwent rapid HIV testing, which was the standard of care at all participating CBOs. Participants who were already using or chose to start PrEP underwent both rapid HIV testing and Cepheid Xpert® POC HIV-1 Viral load testing. For participants living with HIV, only Cepheid Xpert® POC HIV-1 Viral load testing was performed.
Participants with CT/NG detected by NAAT or Cepheid Xpert® POC CT/NG testing were treated according to national guidelines and the 2016 WHO guidelines for the management of these infections. Treatment was preferably provided on the same day the results were received. Participants enrolled in the study were compensated 500 Thai Baht (approx. 15 USD) to cover travel, meal expenses, and loss of income.
Statistical analyses
We defined CT/NG infection as positive by the Cepheid Xpert® CT/ NG POC assay.
Frequencies and proportions were used to describe sociodemographic characteristics. Exact binomial 95% CI were calculated for CT prevalence estimates. Factors associated with CT infection were evaluated using logistic regression, and those with a p ≤ .10 in bivariate analysis were included in multivariable analysis. Likelihood ratio test was used to determine factors to include in the final model (two-sided p < .05). We performed all analyses using STATA® (Version 17, 2021, Stata Corp., College Station, Texas, USA).
Ethical review
We obtained written informed consent from all participants of the POC Study. The study was reviewed and approved by the Ethical Review Committee for Research in Human Subjects of the Faculty of Public Health, Mahidol University (MUPH 11/2025).
Results
Participant characteristics
We enrolled 1885 Thai MSM and TGW during 2019–2021 from four CBOs (SWING Bangkok, RSAT Bangkok, SWING Pattaya, and Mplus Chiang Mai).
Socio-demographic Characteristics of Thai Men who have Sex with Men and Transgender Women participated in the Study to evaluate the Feasibility of Integrating Point-of-Care Testing for Sexually Transmitted Infections and HIV Into Community-based Clinics, Thailand, 2019–2021.
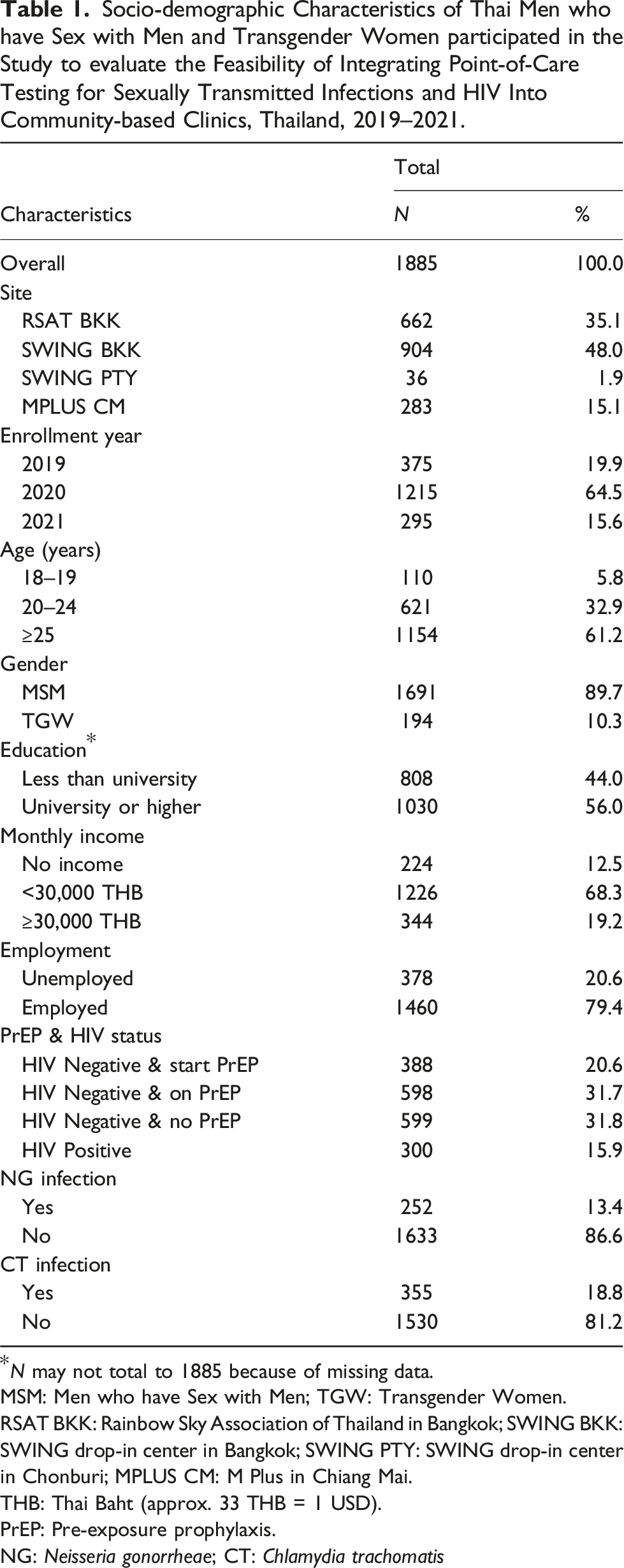
*N may not total to 1885 because of missing data.
MSM: Men who have Sex with Men; TGW: Transgender Women.
RSAT BKK: Rainbow Sky Association of Thailand in Bangkok; SWING BKK: SWING drop-in center in Bangkok; SWING PTY: SWING drop-in center in Chonburi; MPLUS CM: M Plus in Chiang Mai.
THB: Thai Baht (approx. 33 THB = 1 USD).
PrEP: Pre-exposure prophylaxis.
NG: Neisseria gonorrheae; CT: Chlamydia trachomatis
Three hundred participants (15.9%) were living with HIV. Among the remaining participants who were HIV-negative, 388 (20.6%) initiated PrEP use at baseline, 598 (31.7%) were already on PrEP before joining the study, and 599 (31.8%) never initiated PrEP.
CT and NG infections were common, with 13.4% of participants testing positive for NG infection (95% CI: 11.9, 15.0) and 18.8% testing positive for CT infection (95% CI:17.1, 20.7). Additionally, 111 participants (5.9%; 95% CI: 4.9, 7.0) had CT and NG coinfection.
Factors associated with CT infections
Prevalence of CT was associated with the age of participants, NG infection, and HIV status.
There was no-significant difference in overall CT prevalence between MSM and TGW, with percentage of 18.7% (95% CI:16.9, 20.6), and 19.6% (95% CI:14.2, 25.9), respectively (p = .78). However, there was a statistically significant difference in CT prevalence among participants who tested positive for NG infection compared to those who did not, at 44.0% (95%CI:37.8, 50.4) versus 14.9% (95% CI:13.2, 16.8) (p < .01), AOR = 4.1, 95% CI: 3.1, 5.5 (p < .001).
CT prevalence was associated with: younger age (i.e., <25 years), 34.6% in the 18–19 years group (AOR = 3.2, 95% CI: 2.0, 5.0 (p < .001), 24.1% in the 20–24 years group (AOR = 1.7, 95% CI: 1.3, 2.3 (p < .001), and 14.5% in the 25 years and over group, which served as the reference group.
Factors associated with Chlamydia trachomatis Infection Among Thai Men who have Sex with Men and Transgender Women participated in the Study to evaluate the Feasibility of Integrating point-of-care testing for Sexually Transmitted Infections and HIV Into Community-based Clinics, Thailand, 2019–2021.
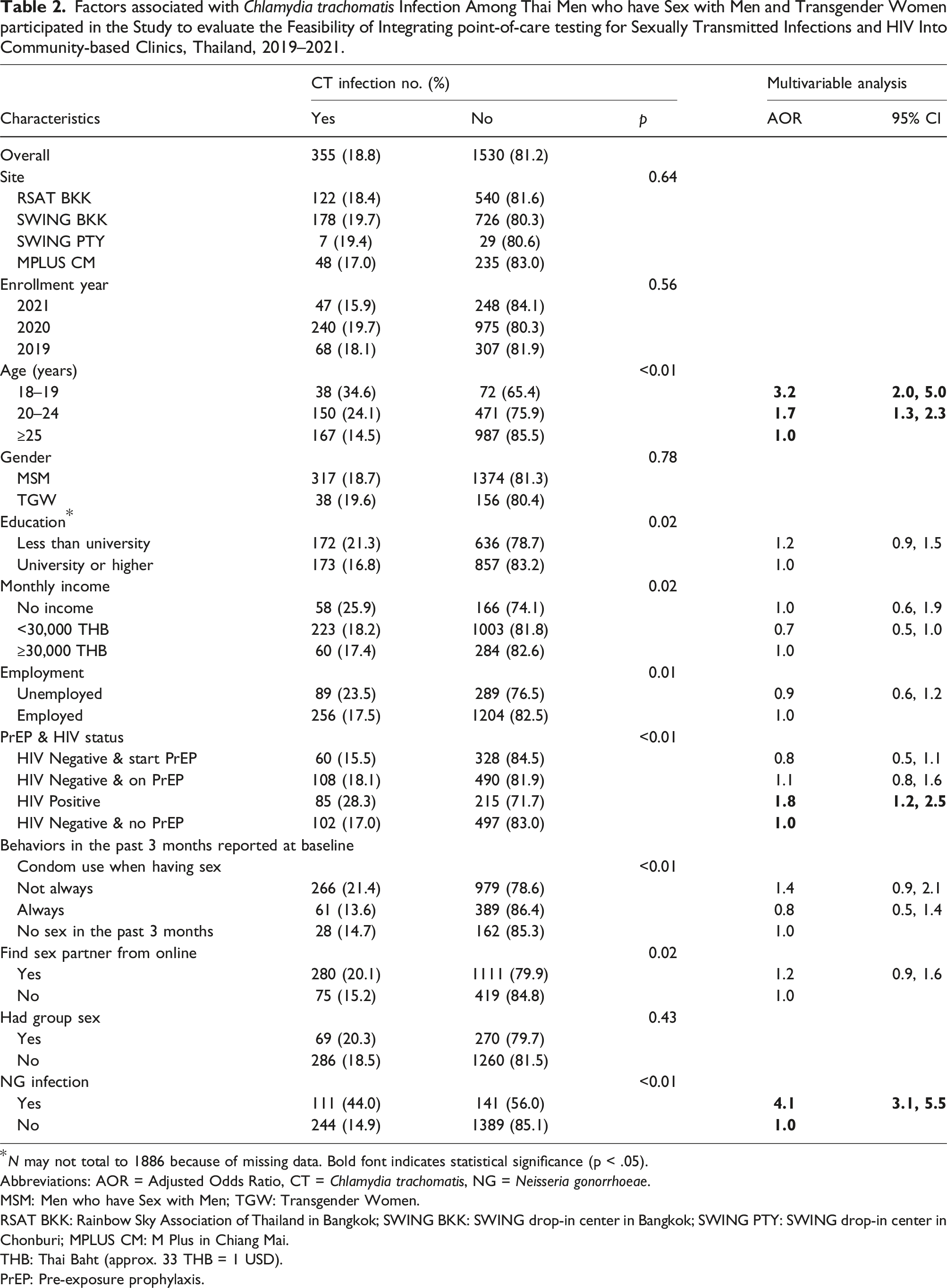
*N may not total to 1886 because of missing data. Bold font indicates statistical significance (p < .05).
Abbreviations: AOR = Adjusted Odds Ratio, CT = Chlamydia trachomatis, NG = Neisseria gonorrhoeae.
MSM: Men who have Sex with Men; TGW: Transgender Women.
RSAT BKK: Rainbow Sky Association of Thailand in Bangkok; SWING BKK: SWING drop-in center in Bangkok; SWING PTY: SWING drop-in center in Chonburi; MPLUS CM: M Plus in Chiang Mai.
THB: Thai Baht (approx. 33 THB = 1 USD).
PrEP: Pre-exposure prophylaxis.
Discussion
Our study found the prevalence of CT infection among sexually active MSM and TGW was high (18.8%), particularly among young individuals aged 18–19 years, where approximately one-third had CT infection regardless of symptoms. Similarly, about one-third of PLHIV were found to have CT infection. Additionally, nearly half (44%) of individuals with NG infection also had CT infection.
The CT prevalence of 18.8% among POC study participants was comparable to the 19% reported among MSM and TGW who participated in a study conducted in Bangkok from 2006 to 2010. 2 It was also similar to the 21.4% (95% CI: 17.6, 25.6) reported in a study conducted in five hospitals across Thailand (Bangkok, Lampang, Ubon Ratchathani, and Mahasarakham provinces) during 2012–2013. 5 Additionally, our analysis revealed that among participants who tested negative for HIV, PrEP use was not associated with CT infection. The findings contrast with results from the open-label intervention ACCESS study in Australia (2016–2018), which reported an increased incidence of STIs (CT, NG, and syphilis) following PrEP initiation compared with pre-enrollment. 6 In Thailand, the Ministry of Public Health (MOPH) recommended daily oral PrEP for high-risk individuals, including MSM, in 2014. 7 The first self-pay PrEP program was introduced in Bangkok that same year, followed by several PrEP demonstration projects. By 2016, PrEP became available at government hospitals. 8 However, there has been no significant change in CT prevalence in Thailand before or after PrEP implementation.
In Thailand, NG is typically diagnosed using a combination of Gram staining and NAAT, while CT is diagnosed using NAAT alone. Both methods rely on laboratory-based testing. However, the distance between laboratories and clinics often results in delays in CT/NG diagnosis and management, reducing opportunities to mitigate transmission risks and associated complications. To address these challenges, this study integrates community engagement and Cepheid Xpert® CT/ NG testing into CBOs clinics. This approach enables MSM and TGW diagnosed with CT or NG to receive same-day diagnostic results and treatment, along with prompt referral for appropriate management. Notably, the Cepheid Xpert® CT/NG POC assay, when administered by Key-Pop lay providers, has demonstrated high performance and feasibility in detecting both CT and NG infections, further supporting its implementation in community-based settings. 4 However, the high cost associated with testing multiple anatomical sites (pharyngeal, urethral, and rectal) can pose a significant financial burden. A previous study found that CT is most frequently detected in the rectum among Thai MSM and TGW. In settings where screening all specimens is not feasible, prioritizing rectal screening is a practical and cost-effective approach.3,9
We found that factors associated with CT infection included young age (<25 years), HIV infection, and NG infection.
Aligned with findings from various countries, young MSM and TGW demonstrated a higher likelihood of CT infection, attributed to engagement in sexual activities without a condom (China 10 ; Brazil 11 ; Nigeria 12 ; and Thailand 2 ). However, we were unable to demonstrate a relationship between condom use and CT infection in our study. This may be attributed to the timeframe differences: condom use was assessed over a 3-month period, whereas the study’s inclusion criteria covered a 6-month timeframe. MSM and TGW with asymptomatic CT infections could have been infected for longer than 3 months, making condom use irrelevant to the CT infections detected at baseline in this study.
Previous diagnoses of CT and NG have been identified as risk factors for HIV acquisition. 13 However, it is also possible that CT and NG are not directly causal but instead act as a confounding factor in the relationship between sexual behavioral risks and HIV acquisition. Since these behaviors are linked to an increased risks of STI infections, distinguishing the causal relationship between these infections and HIV remains challenging. 13
The enrollment of the POC Study was during 2020–2021, the COVID-19 pandemic in Thailand, which is part of the worldwide pandemic of severe acute respiratory syndrome coronavirus identified in 2019. In response to the situation, the study team set up a visible platform outside their anonymous clinic in April 2020 with a screening system for clients to provide HIV testing and prevention supplies (e.g., condoms, postexposure prophylaxis (PEP), and PrEP). 14 The study successfully enrolled participants during the pandemic, highlighting the need for HIV prevention services to remain accessible and flexible for vulnerable populations during emergencies and public health crises. It is crucial to maintain access to routine HIV services and avoid disruptions to ensure continuity of care and support.
Our study had several limitations. Firstly, participants enrolled during the COVID-19 pandemic may not be representative of those who would have been enrolled during non-epidemic periods. Sexual behaviors were assessed using self-report, which may have been influenced by social desirability bias. Lastly, there might be a timeframe discrepancy between the assessment of sexual behaviors (i.e., during the last 3 months) and the occurrence of CT infection.
Conclusions
In conclusion, our study demonstrated that CT infection was associated with several factors. HIV testing venues for MSM and TGW should integrate routine STI screening and treatment, re-screening, and the implementation of STI prevention strategies, including the provision of condoms and PrEP.
Footnotes
Acknowledgements
The authors kindly acknowledge and are thankful for the support of the Rainbow Sky Association of Thailand (RSAT), the Service Workers in Group Foundation (SWING), M Plus Foundation, the Institute of HIV Research and Innovation (IHRI), and the United States Agency for International Development.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.