
Abstract
Background
The global burden of syphilis has remained persistently high with globally prevalent cases of syphilis, estimated to be 49.71 million in 2019. In India, where rates of syphilis screening remain sub-optimal, an accurate point-of-care (POC) test is convenient to carry out and guide immediate treatment. Here, we sought to evaluate the performance of an indigenous rapid POC test (Syphicheck -WB).
Methods
This study was carried out in the serology laboratory of our tertiary care center over 2 months. Five hundred serum samples were chosen randomly. Performance parameters of the POC test were calculated in comparison to the Treponema pallidum hemagglutination test, which was considered the reference standard.
Results
One hundred and six samples (21.2%) were reactive for syphilis by the reference method (TPHA). The sensitivity and specificity of the POC test, were 81.13% and 98.48% respectively. The sensitivity and specificity of the reverse algorithm using POC test for screening, were 81.13% and 99.75% respectively, and of the traditional algorithm using VDRL were 77.36% and 100% respectively.
Conclusion
This POC test is a promising candidate as a rapid treponemal screening test. It is likely to improve screening for syphilis under both laboratory as well as field conditions.
Introduction
Syphilis, known since ancient times, is a complex infection affecting multiple organ systems, caused by the non-cultivable spirochaete Treponema pallidum, which is transmitted by direct sexual contact or vertically from mother to child during pregnancy. 1 The global burden of syphilis has remained persistently high. The total number of globally prevalent cases of syphilis, in 2019, was estimated to be 49.71 million. 2 In 2022, 8 million adults between 15 and 49 years of age acquired the disease. 3 In 2020, the global rate of congenital syphilis was 425 cases per 100 000 livebirths. 2 Among the 81 priority countries (including India) with high rates of deaths in the under 5 year age group, less than 50% of pregnant women were screened for syphilis in 2020.4,5 In 2022, as per WHO data for India, only 58.3% of women accessing ante-natal care (ANC) services were screened for syphilis, of whom 0.18% tested positive. 3 Though showing an improving trend, the coverage for ante-natal screening of syphilis in India is still sub-optimal.
Further, the estimates of syphilis in men who have sex with men (MSM) is deeply concerning. In a meta-analysis of data from 2000 till 2020, the global pooled prevalence of syphilis among MSMs was disproportionately high at 7.5% compared to 0.5% men in the general population.6,7 In India, despite a lack of nation-wide data on syphilis in MSMs, studies have documented an explosive increase in prevalence, ranging from 7% in a 2 year study (2013-2014) to almost 41.8% in the last 3 years (2016-2019) of a 17 year study.8,9
Screening for syphilis is performed using serological tests which detect treponemal and non-treponemal antibodies using either the traditional algorithm or the reverse algorithm.10,11
Current guidelines in the Indian scenario, recommend using non-treponemal tests such as the Rapid Plasma Reagin (RPR), Venereal Disease Research Laboratory (VDRL) tests or a rapid treponemal test for screening patients with sexually transmitted infections (STI). 12 Especially for the elimination of parent to child transmission (E-PTCT), use of an initial treponemal point-of-care (POC) test, has been advised, at health-care service points without laboratories and for women coming directly in labour. 13 As the syphilis algorithm may require confirmatory or reflex testing, laboratory-based serologic testing would take 3–5 days, causing patients to be lost to follow-up. An accurate POC test result is convenient to carry out under field conditions and guides immediate treatment.13–15
Therefore, rapid treponemal POC tests play a critical role in improving syphilis screening by increasing the coverage and frequency of testing. Currently the Syphilis Health Check (Diagnostics Direct, LLC, Stone Harbour, NJ) is approved by the FDA while the DPP HIV- Syphilis Assay (Chembio Diagnostic Systems, Hauppauge, NY, USA) and SD Bioline HIV/Syphilis Duo (Standard Diagnostics, Yongin, South Korea), are both FDA approved and WHO pre-qualified.14,16,17 In this study, we sought to evaluate the performance of an indigenous rapid POC test Syphicheck -WB (Zephyr biomedicals, Tulip Diagnostics, Goa, India) under our laboratory conditions.
Materials and methods
This study was carried out in the serology laboratory of our tertiary care center from October to December 2024. As per our standard operating protocol, the traditional algorithm is used for routine testing of syphilis [non-treponemal test: venereal disease research laboratory test (VDRL - Institute of Serology, Kolkata); treponemal test: Treponema pallidum hemagglutination assay (TPHA – SPINREACT, Coloma, Spain)]. Five hundred serum samples were chosen randomly from samples received in the serology laboratory for routine testing of syphilis.
Demographic data which was readily available on the requisition form or on the hospital website, such as age, gender, referring department was collected. Serum samples were used for the study only after informed consent was given by the patient. Any information given by the patient was kept strictly confidential and all samples were identified by a code.
Whole blood (3 mL–5 mL) was collected using a vacutainer tube without an anticoagulant, coagulants, or a serum separator component. After collection of whole blood, the tube was left undisturbed at room temperature for approximately 15–30 minutes to allow for clot formation and then centrifuged at 1000–2000g for 10 minutes. Serum samples were stored at 2°C–8°C (35.6°F–46.4°F) and used for this study within 5 days, as per our sample storage policy.
Each serum sample was tested in parallel using the following the following methods: Treponemal POC test: Syphicheck-WB; Non-treponemal Test: VDRL; Treponemal Reference Standard: TPHA.
For the venereal disease research laboratory Test (VDRL) serum was heated at 56°C for 30 minutes. VDRL antigen supplied by the Institute of Serology, Kolkatta is an alcoholic solution containing cardiolipin 0.03%, purified lecithin 0.21% and cholesterol 0.9%. Antigen emulsion was prepared by adding 0.5 mL of antigen to 0.4 mL buffered saline. Heated serum (0.05 mL) was pipetted onto concavity slides and 1 drop of antigen emulsion was added to the serum. Slide was rotated for 4 minutes, followed by reading of results under low power objective (100x magnification). For reactive samples, serial two fold dilutions of serum were made in 0.9 % saline and tested, with results being reported as the highest dilution of serum producing a definite reaction.
Treponema pallidum hemagglutination assay (TPHA – SPINREACT, Coloma, Spain) was carried out as per manufacturer’s instructions. Serum samples were diluted at 1:20 (10 µl serum and 190 µl diluent) with diluent comprising Phosphate Buffered Saline containing T. pallidum (Reiter extract). 25 µl of diluted serum was added to adjacent wells of a microtitration plate. Control cells comprising stabilized solution of avian erythrocytes were added to the first column followed by Test cells containing stabilized avian erythrocytes sensitized with T. pallidum (Nichols) antigen. The microplate was incubated at room temperature for 45–60 minutes, followed by macroscopic examination of the agglutination patterns of the cells.
The POC test is an indigenous commercial rapid qualitative, two site double antigen sandwich immunoassay, developed by Tulip Diagnostics, India, for the detection of antibodies to Treponema pallidum in human serum, plasma or whole blood specimen. As per the manufacturer’ instructions, 25 µl of sample was added to the port A of the test device, followed by four drops of diluent buffer into port B. Results were read after 15 minutes in the control and test window, a positive result showing as a distinct pink/purple band in both windows.
This POC test utilizes the principle of agglutination of antibodies / antisera with respective antigen in immunochromatography format. As the test sample flows through the membrane assembly of the test device, the recombinant Treponema pallidum antigens (47 kDa, 17 kDa) colloidal gold conjugate forms a complex with Treponema-specific antibodies in the sample. On moving further to the test region, it is immobilized by the recombinant Treponema pallidum antigens (47 kDa, 17 kDa) coated on the membrane leading to the formation of a pink to deep purple band at the ‘T’ or test region. The unreacted conjugate and unbound complex, moves further and is subsequently immobilized by agglutination sera for rabbit globulin coated at the control ‘C’ region of the membrane, forming a pink/purple band. The control band serves to validate the test.
Evaluation of performance characteristics of POC test and VDRL
Performance characteristics were calculated for both POC test and VDRL, using TPHA as the reference standard. Performance characteristics for POC test and VDRL were also calculated for samples received from STI/ART clinics and ANC clinics, with reference to TPHA.
Evaluation of diagnostic algorithms
Traditional Algorithm
The results of VDRL followed by TPHA were analyzed to determine performance metrics relative to the reference standard.
Reverse Algorithm
The results of POC test followed by VDRL, and TPHA (when required in view of discordant results between the POC test and VDRL), were used to evaluate the reverse algorithm.
Results
Out of the 500 patients who underwent serological testing, 242 participants were women (48.4%), 256 (51.2%) were men and 2 (0.4%) belonged to the transgender category. As per age group distribution, 16 (3.2%) belonged to the pediatric age group with a median age of 18 years [IQR 14,18], 467 (93.4%) to the working age group with a median age of 30 years [IQR 26,36] and 8 (1.6%) to the geriatric age group with a median age of 73.5 years [IQR 70.5,87] respectively. As per the modified Kuppuswamy scale, 22% belonged to the lower class, 40% of participants belonged to the upper lower class, 32% to the lower middle class, 6% to the upper middle class. 18
Department-wise distribution of samples showed 38.6% (193/500) samples from STI clinic, 28.6% (143/500) samples from ANC clinic, 5.2% (26/500) samples from medicine outpatient department, 1.8% (9/500) from the antiretroviral treatment (ART) center and the rest (25.8% (129/500)) samples from other departments.
106 samples (21.2%) were reactive for syphilis by the reference method. 92 samples were reactive via the POC test, of which false positive results in comparison to the reference method were 1.2% (6/500). Similarly, 124 samples were reactive via VDRL in which the false positive results were 8.4% (42/500).
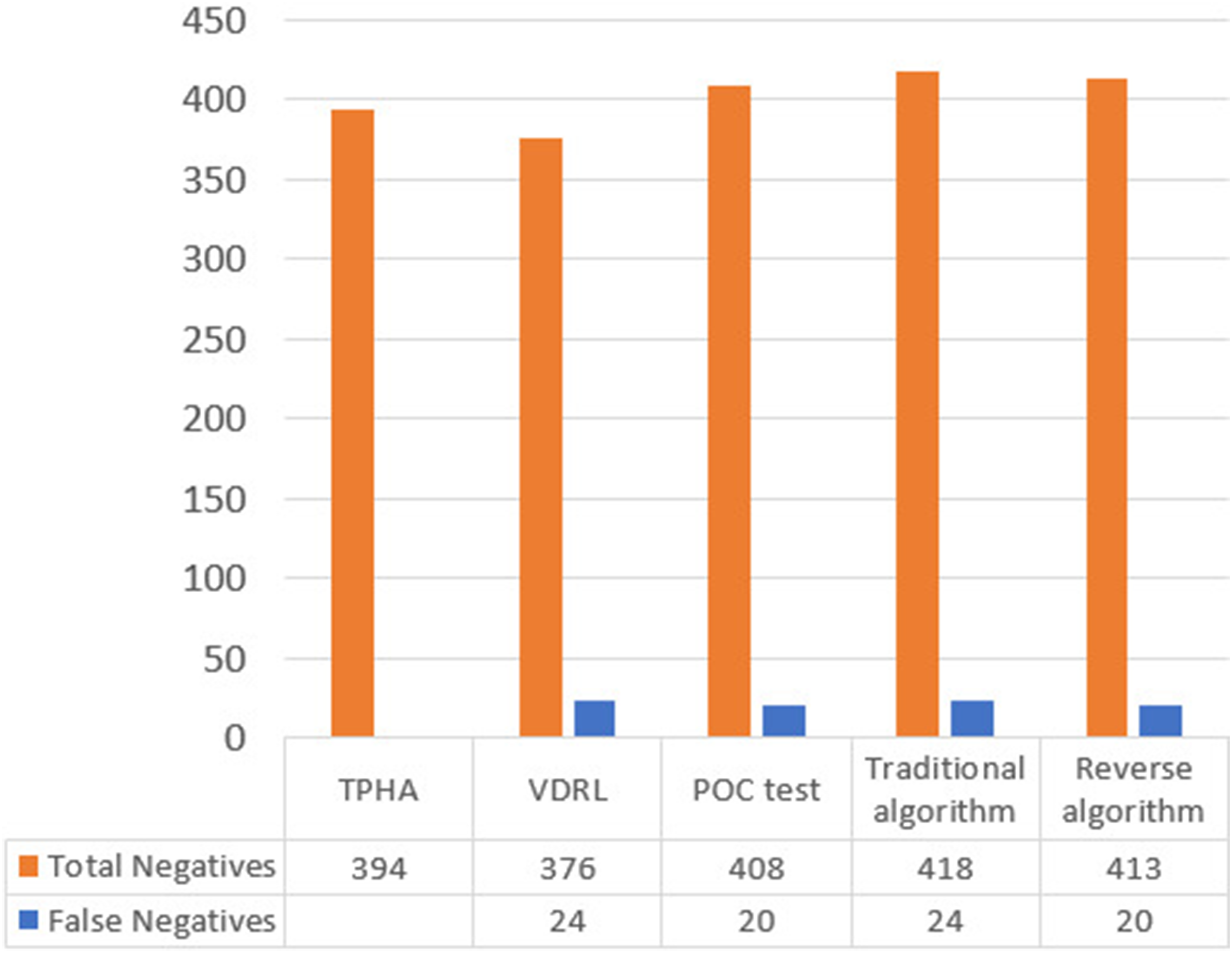
A comparison of the overall false positive and false negative results by each method is shown in Figures 1 and 2. The POC test showed 1.28% (6/467) false positives in the working age group and none in the pediatric and geriatric age groups whereas VDRL showed maximum false positives 8.5% (40/467) in the working age group compared to the 12.5% (2/16) in the pediatric age group and none in the geriatric age group. In the samples for ante-natal screening of syphilis, the POC test showed a false positive rate of 0.69% (1/143), whereas VDRL showed a false positive rate of 11.8% (17/143). Comparison of false positives between VDRL, POC test, traditional algorithm & reverse algorithm. Comparison of false negatives between VDRL, POC test, traditional algorithm & reverse algorithm.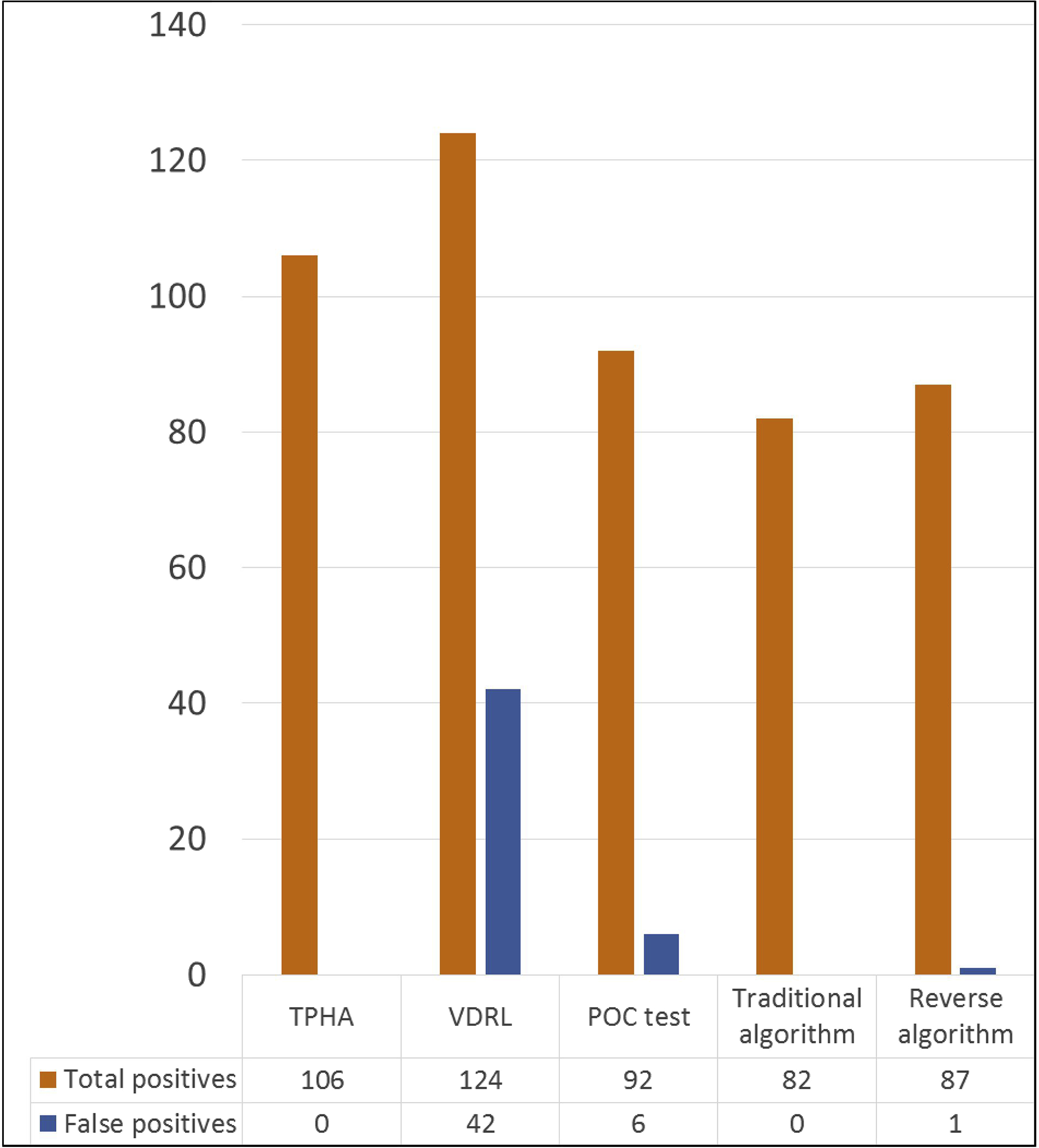
The sensitivity of the POC test against the TPHA reference standard was 81.13% (95% CI; 72.38–88.08) and the specificity of the test was 98.48% (95% CI; 96.72–99.44). The sensitivity of the VDRL test compared to the TPHA reference standard was 77.36% (95% CI; 68.21–84.92) and the specificity of the test was 89.34% (95% CI; 85.86 – 92.21).
Performance characteristics of POC test, VDRL, traditional algorithm and reverse algorithm.
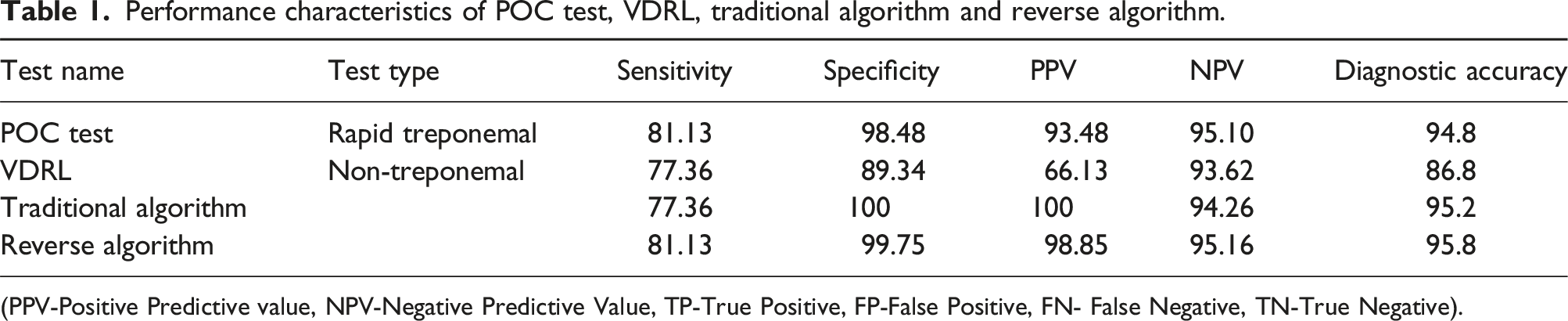
(PPV-Positive Predictive value, NPV-Negative Predictive Value, TP-True Positive, FP-False Positive, FN- False Negative, TN-True Negative).
Performance characteristics of POC test & VDRL in samples from STI/ART and ANC clinic.
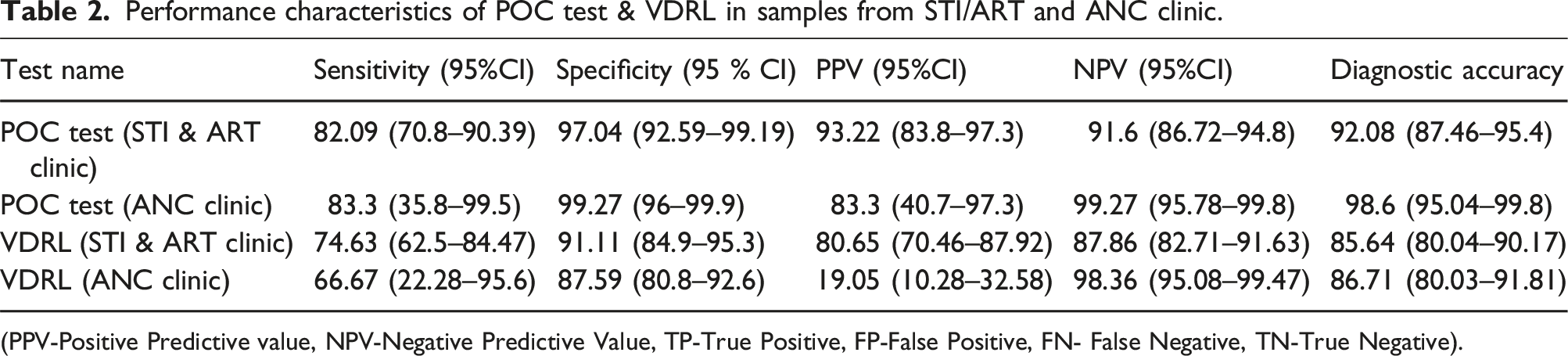
(PPV-Positive Predictive value, NPV-Negative Predictive Value, TP-True Positive, FP-False Positive, FN- False Negative, TN-True Negative).
Discussion
Confirmed diagnosis of syphilis requires identification of clinical signs and symptoms along with identification of T. pallidum in darkfield microscopy, in tissues with silver or immunohistochemical staining or detection of T. pallidum DNA via PCR, for primary, secondary and tertiary syphilis. These diagnostic modalities can be undertaken only in specialized laboratories and are cumbersome, time consuming, and expensive.19–21 The serodiagnosis of syphilis via reactive treponemal and nontreponemal tests is classified as probable diagnosis for primary and secondary syphilis but is easier to perform, being less technically demanding and expensive. However, it is the mainstay of diagnosis for latent syphilis, on the basis of documented seroconversion or a four fold or more rise in titer for nontreponemal test along with seroconversion of a treponemal test for early latent, and a four fold or greater rise in nontreponemal test titer for late latent syphilis respectively. 20 Nontreponemal tests can be used to monitor progression of disease and response to treatment. However, their sensitivities in diagnosing primary syphilis and tertiary syphilis are low, along with the possibility of a prozone phenomenon in sera with high antibody titers.14,19 We have used VDRL in the study, as it is routinely used in our serology laboratory, and is recommended by CDC and National AIDS Control Organization (NACO), India.14,15 For serum, it has a sensitivity comparable to RPR in primary and secondary syphilis as described by the CDC, though some studies show a better sensitivity of RPR for primary syphilis.14,22 For latent and tertiary syphilis, very few studies on RPR have been done, whereas studies on VDRL in early latent, late latent and tertiary syphilis show sensitivities of 82.1–100%, 63–71%, and 47% respectively.14,22 Acute false positive results due to hepatitis, infectious mononucleosis, viral pneumonia, other viral infections, malaria, and pregnancy and chronic false positive reactions due to connective tissue disorders, leprosy and malignancy have been associated with nontreponemal tests.19–21
Treponemal tests such as fluorescent treponemal antibody absorption test (FTA-ABS), T. pallidum particle agglutination test (TPPA), microhemagglutination assay for T. pallidum (MHA-TP) and T. pallidum hemagglutination assay (TPHA) have similar sensitivities for secondary, early latent and late stages of syphilis.14,22,23 In primary syphilis TPPA and TPHA have better sensitivities compared to FTA-ABS and MHA-TP. TPHA was used as the reference standard in our study as it is recommended by Indian guidelines for confirmation of diagnosis. 15 TPHA has good sensitivity in primary (86%), secondary (100%), early latent (100%) and late latent (99%) syphilis and is comparable to TPPA. 22 These tests remain positive for a lifetime and do not have a prognostic value.
In the traditional algorithm a non-treponemal test is performed as a screening test, followed by confirmation by a treponemal test, if required. Specimens which are reactive in the initial screening and non-reactive by the confirmatory test are regarded as biological false positives. In comparison, the reverse algorithm uses a treponemal test for screening, followed by a quantitative non-treponemal test. Any discordance between the treponemal and non-treponemal tests are resolved using a second treponemal test which preferably detects different antigens compared to the screening test. This makes the diagnosis more sensitive for primary and latent disease while increasing the performance parameters of the combined test.10,14,20,21
Traditional and reverse algorithms are both used by laboratories today. Low-volume laboratories generally use the traditional algorithm due to the low cost of manual non-treponemal tests. Until very recently, there were no FDA cleared automated non-treponemal platforms. Therefore high-volume laboratories opt to perform the reverse algorithm as FDA-cleared automated treponemal assays that increase throughput are widely available. With a shortage of medical laboratory technicians, automated systems reduce labour costs as well as the repetitive pipetting steps of manual assays. 21 However, POC tests for syphilis screening represent a different challenge as these are to be designed to be used under field conditions or basic health facilities without laboratory infra-structure. The performance of a POC test may vary significantly depending upon the population being screened, the temperature and humidity conditions prevalent, the field worker or test operator and the test stability under available storage conditions. 16
In 2006, WHO introduced the ASSURED criteria for point-of-care tests: affordable, sensitive, specific, user-friendly, rapid and robust, equipment-free and deliverable to end users. WHO has further defined the POC test for syphilis as a single use diagnostic test, which is small, portable and handheld with no requirement for power supply. 24 For POC tests based on the reference technology of treponemal tests such as T. pallidum particle agglutination (TPPA), the minimum sensitivity and specificity have been kept as >80% and >90% respectively. 24 In this study we have not evaluated performance characteristics under field conditions using fingerprick blood. Earlier studies on treponemal POCTs using finger prick blood have shown a lower sensitivity ranging from 50% to 98%, compared to serum, which includes the FDA-approved Syphilis Health Check. 25 However, despite the lower sensitivity in many studies, use of POCTs has resulted in an increase in screening in high risk population groups and in resource limited settings.26,27 Indian guidelines have also recommended the use of RDT based tests both in the field and in higher centres such as the District STI/RTI clinics, where phlebotomy would be undertaken. 15 This indigenous rapid POC test with a sensitivity and specificity and diagnostic accuracy of around 81.13% , 98.48% and 94.8% respectively, is therefore likely to improve screening for syphilis as per the reverse algorithm, under both laboratory as well as field conditions. The diagnostic accuracy of 94.8% compared to that of VDRL which is 86.8%, is of relevance in our scenario, where screening of at risk populations remains sub-optimal and patients are lost to follow-up.
The results of our study, especially the specificity, compare favorably with the FDA-approved Syphilis Health Check rapid treponemal test and WHO pre-qualified SD Bioline HIV/Syphilis Duo. Meta-analysis of retrospective and prospective laboratory evaluations for Syphilis Health Check showed sensitivities ranging 88.7%–100% and 50%–100% with specificities ranging from 83.3% to 100% and 50%–100% respectively.25,28–30 Similarly previous studies on SD Bioline show sensitivities ranging from 88% to 91.8% and specificities of 82.9–99.4%.25,28–30 In most of these studies, the performance evaluation was done only on attendees of STI and ANC clinics, whereas a limitation of this study is that samples were included randomly from various out-patient departments in addition to ANC and STI clinics, which would have resulted in a lower sensitivity. Performance characteristics of the POC test on samples from STI and ART clinics as well as ANC clinics showed improved sensitivity compared to overall values (Table 2). The sensitivity of VDRL for samples coming from the ANC clinics showed a lower sensitivity as a result of pregnancy induced false positives in a nontreponemal test. However, the results of the test were not correlated with patient’ history, symptoms and diagnosis. This precluded correlation of test results for symptomatic versus asymptomatic patients, immunocompromised patients and those with co-infections. During the testing of isolates, we also found that the band for the test line was light in colour which would make it difficult to read under field conditions without a light source.
Conclusion
This rapid POC test is a promising candidate for syphilis screening of “at-risk” populations via the reverse algorithm. Further studies are required to address the shortcomings of Syphicheck WB, which if improved upon, can make it suitable for rapid treponemal testing under field conditions as well.
Footnotes
Author contributions
Study conception and design was given by HG. Supervision was done by HG, PB and BKD. Material preparation, data collection and analysis were performed by MN. Statistical analysis was performed by MN. The first draft of the manuscript was written by MN and draft review and editing was done by all authors. All authors read and approved the final manuscript and are accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
All data generated or analysed during this study are included in this article.