
Abstract
A 19 year old man was diagnosed newly acquired HIV and prescribed bictegravir/emtricitabine/tenofovir alafenamide at his initial visit for HIV care. The genotype results from that initial visit returned two weeks later, showing high-level multi-class transmitted drug resistance, including multiple resistance-associated mutations (RAM) in the integrase gene. Although he had an initial substantial decline in viremia in the first 4 weeks, it was felt that the risk of subsequent failure was too high, and his antiretroviral treatment (ART) regimen was therefore changed to daily dolutegravir and darunavir/cobicistat/emtricitabine/tenofovir alafenamide, plus injected lenacapavir. He had durable virologic suppression on this new regimen for 12 months as of his last follow-up. This case of high-level multi-class transmitted drug resistance, in the context of rapid emergence of resistance to dolutegravir where it has been used as part of a salvage regimen, suggests that assessing for RAM in the integrase gene should be added to the currently recommended resistance testing for all patients with newly acquired HIV prior to initiating ART.
Keywords
Introduction
Non-nucleoside reverse transcriptase inhibitor (NNRTI) and protease inhibitors (PI) revolutionised HIV care in 1995 by allowing combination antiretroviral therapy (cART) that, for the first time, suppressed HIV viremia, resulting in immunological recovery. 1 The antiretroviral (ARV) medications comprising the early cART regimens had low genetic barriers to resistance, however, development of drug resistant mutations (DRM) was common, causing drug resistance, failure of regimens, and recrudescence of AIDS.2,3
An additional consequence of acquired drug resistance is onward transmission of drug-resistant viruses. Transmission of drug-resistant viruses is not the rule, however–most transmissions from people with drug-resistant viruses are of wild-type, rather than drug-resistant virus–but nonetheless, 12 to 24% of newly acquired HIV in the US were with drug resistant viruses, termed transmitted drug resistance (TDR). 3 This observation led to the recommendation for obtaining pre-treatment genotype testing, specifically assessing the pol gene (which encodes both polymerase and protease gene products) for resistance-associated mutations (RAM), for all those with newly acquired HIV to avoid empirical treatment with ARV to which the acquired virus was resistant.
Between 1995 and 2008, new ARVs were developed with better potency and tolerability, both in the existing and in new drug classes. However, it wasn’t until darunavir (DRV) was released in 2008, followed by dolutegravir (DTG) in 2013, and subsequently bictegravir (BIC), that initial treatment regimens achieved sufficiently high genetic barriers to resistance to where acquisition of drug resistance might potentially no longer occur.4–6 Further, since most acquired drug resistance had been due to selection by early generation ARV, most TDR had not been of sufficient magnitude to result in treatment failure of these modern initial regimens, and so controversy developed about whether baseline resistance testing remained clinically worthwhile, 7 which, in any case, evaluates just the genes encoding polymerase and protease, and not integrase. 8
We report a case of recently-acquired HIV with multi-class resistance, including to second generation INSTI, predicted to result in treatment failure of all first-line cART.
Case
A 19-year-old man presented to a New York City community health clinic one day after testing positive for HIV at his homeless shelter. At this initial visit, he reported no acute retroviral syndrome symptoms. He reported condomless anal intercourse with men (receptive and insertive) and condomless vaginal intercourse with women, no use of drugs by injection, and had never taken PrEP or PEP. The exact date of HIV acquisition is unknown, as the patient had no prior documented HIV testing. However, based on the patient’s reported risk behaviors, we felt acquisition would have occurred within the past 12 months. We contacted the New York City Department of Health (NYC DOH) who told us that they were aware of this individual and had followed their protocols for newly-diagnosed individuals, but, as per DOH policy, could not tell us anything further about contact tracing, partner notification, or if they performed any testing themselves, such as antibody avidity testing. Initial testing included HIV resistance testing, including the integrase gene (Quest Diagnostics) in alignment with New York Department of Health (DOH) HIV guidelines. 9 He was prescribed BIC/emtricitabine (FTC)/tenofovir alafenamide (TAF) the same day.
HIV-1 genotype assay results at treatment baseline and 4 weeks after treatment of a man with recently acquired HIV.
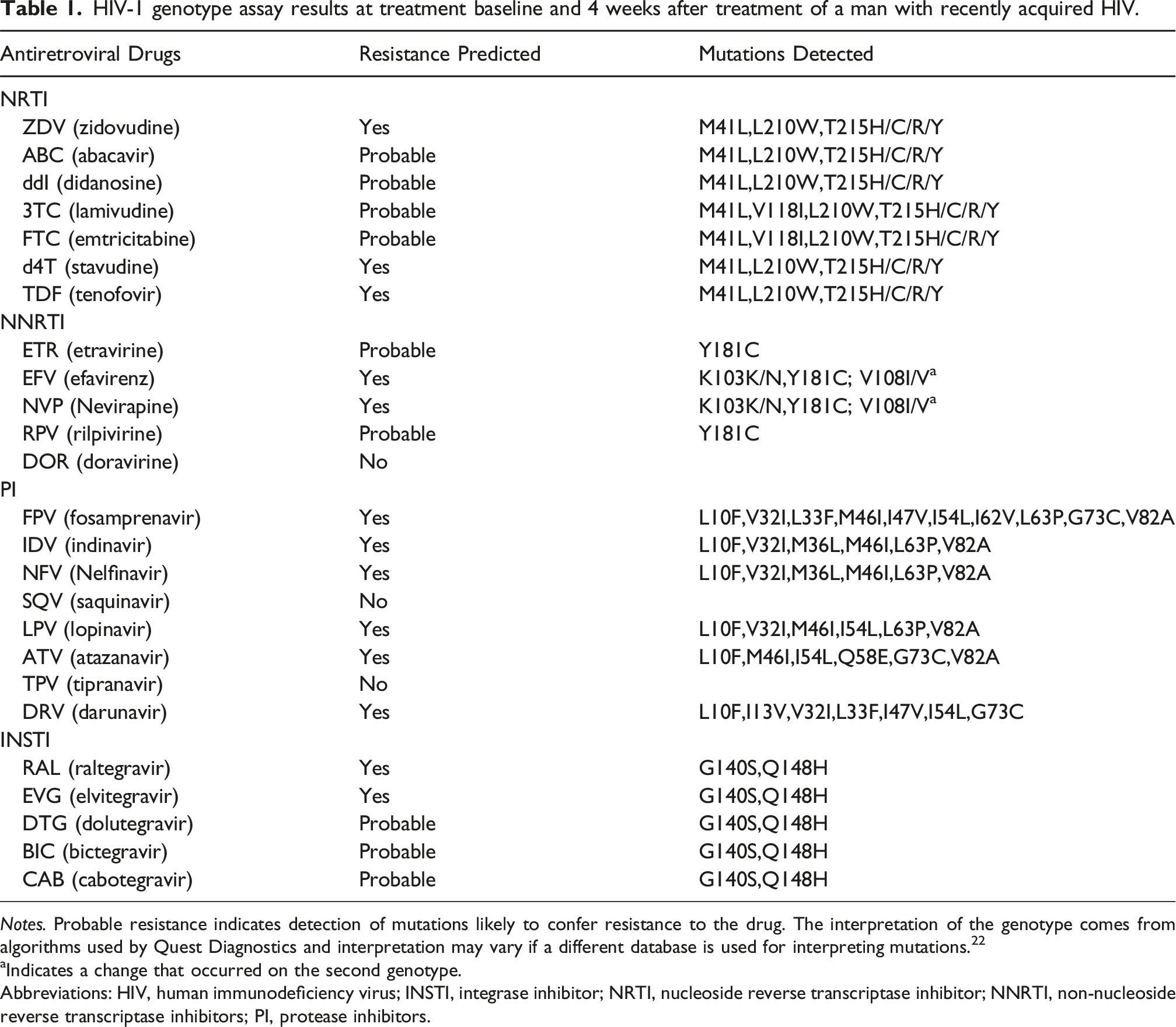
Notes. Probable resistance indicates detection of mutations likely to confer resistance to the drug. The interpretation of the genotype comes from algorithms used by Quest Diagnostics and interpretation may vary if a different database is used for interpreting mutations. 22
aIndicates a change that occurred on the second genotype.
Abbreviations: HIV, human immunodeficiency virus; INSTI, integrase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitors; PI, protease inhibitors.
Discussion
We report on one of the first U.S. cases of multi-class TDR of sufficient magnitude to lead to failure of all the recommended regimens for initial cART, that is, RAM in protease sufficient to mediate resistance to boosted DRV, and also in integrase sufficient to mediate resistance to the entire INSTI class. Specifically, the virus contained the non-polymorphic G140S/Q148H double mutation. Each of these RAM, singly, decreases susceptibility to first generation INSTIs: G140S reduces elvitegravir (EVG) susceptibility; and Q148H reduces susceptibility to raltegravir (RTG),EVG, and CAB in the range of by 5 to 20 fold. 11 However, Q148H in combination with G140S reduces DTG susceptibility by 2-10 fold and BIC susceptibility by 2-5 fold, both considered to be clinically significant decrements. 11
Therefore, after reviewing his genotype and the literature, we felt there was too high a risk of virological failure of his initial regimen of BIC/TAF/FTC, even with his initial decline in viremia, and he needed a more robust regimen. In designing the new regimen, we included consideration of the issues of his being young, medication-naïve, and with housing instability and limited social support, and felt we needed balance potency with providing a once-daily regimen with as few pills as possible. We therefore chose a combination of oral and injected treatment. For the oral component we chose once-daily dolutegravir and darunavir/cobicistat/emtricitabine/tenofovir alafenamide. Given the risk that boosted DRV would not be fully active, and that daily DTG would not maintain adequate blood levels for full activity throughout the day, we chose to add injected LEN, due to the registration trials demonstrating its effectiveness in the setting of “salvage” therapy, where optimized background treatment was suboptimally active in the setting of multidrug resistance.12,13 Although a few agents were available from other drug classes to which there was not evidence of drug resistance, such as fostemsavir or maraviroc, these are dosed twice daily; and for that reason we also did not dose DTG twice daily.
We would not have detected this significant drug resistance to be able to make this modification in treatment, however, if we had strictly followed current US guidelines, which do not recommend baseline INSTI resistance testing unless INSTI TDR is suspected (e.g., prior long-acting cabotegravir PrEP or INSTI-based nPEP use), 14 neither was the case in this patient. But although published evidence from the US does not suggest high levels of TDR to INSTI-based regimens based on literature from early years of INSTI use,15–18 INSTI DRM are likely to increase with increasing use as part of salvage regimens, as had been predicted in Africa, where DTG resistance is increasing significantly. 19
In summary, we believe that this case should serve as a cautionary note that some patients with newly acquired HIV may have high-level TDR, potentially to four classes of ARV, that could mediate resistance to our most potent initial ART regimens. Given the expanding global use of INSTIs, our case suggests that incorporating INSTI RAM assessment into baseline resistance testing should be considered for addition into the US guidelines alike other international guidelines20,21 for treatment of people with HIV.
Footnotes
Ethical considerations
This report did not require Institutional Review Board (IRB) approval as it consists solely of a case report and did not contain any human or animal trials.
Consent for publication
Written informed consent was obtained from the patient, including written consent to publish the details of the case.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.