
Abstract
We present a case of a 53-year-old person living with human immunodeficiency virus and a new diagnosis of latent tuberculosis. The patient had baseline suppressed HIV viral load on fixed dose combination dolutegravir/abacavir/lamivudine when once-weekly rifapentine 900 mg/isoniazid 900 mg/pyridoxine 25 mg was initiated for 12 weeks. An additional 50 mg dolutegravir dose, administered in the evenings, was added to the daily antiretroviral regimen for treatment duration secondary to rifapentine uridine diphosphate glucuronsyl transferase induction. Dolutegravir trough concentrations decreased during concurrent therapy with noted slight HIV viral load rebound. Upon completion of rifapentine use, and a return to dolutegravir 50 mg daily dose, the trough concentrations increased with a return to an undetectable viral load. We provide suggested dolutegravir dosing considerations with concomitant rifapentine use, not currently addressed in recommended guidelines.
Introduction
Recommended treatment for persons living with human immunodeficiency virus (PLWH) and latent tuberculosis (LTB) includes: once daily (QD) isoniazid (INH) 300 mg for 6-9 months, weekly INH (900 mg)/rifapentine (900 mg) for 3 months, or QD INH (300 mg)/rifapentine (600 mg) for 1 month. 1 Drug-drug interactions (DDIs) with antiretroviral (ARV) therapy and rifamycins exist. 1 Dolutegravir (DTG) is primarily metabolized by uridine diphosphate glucuronosyl transferase (UGT) 1A with minimal contribution from cytochrome P450 (CYP) 3A4, both of which are induced by rifamycins. Guidelines recommend DTG 50 mg QD with weekly rifapentine/INH when no integrase strand transfer inhibitor (INSTI) resistance is suspected. 1 Concurrent rifampin with DTG results in reduced concentrations, necessitating twice daily (BID) dosing. 2
A 3-month LTB pharmacokinetic (PK) analysis (the DOLPHIN study) evaluating weekly rifapentine/INH with QD DTG 50 mg/emtricitabine (FTC)/tenofovir disoproxil fumarate (TDF) assessed INSTI trough concentrations (Ctrough). 3 Although DTG Ctrough maintained >300 ng/mL (the mean Ctrough with QD DTG 10 mg utilized in pre-clinical trials), a 47% reduction in the geometric mean ratio (DTG with rifapentine compared to DTG alone) resulted [90% confidence interval (0.49–0.59)] with eight values <158 ng/mL (5th percentile concentration with DTG 10 mg daily) in two patients.3,4 All 60 patients maintained viral load (VL) suppression. 3 We report a case of LTB treatment in a PLWH utilizing weekly rifapentine/INH with QD DTG 100 mg and INSTI Ctrough analysis to support the use of dose titration for 12 weeks of concurrent use.
Case
A 53-year-old male PLWH on combination dolutegravir/abacavir/lamivudine (D/A/L) and VL suppression for 5 years (brief rebound during the COVID-19 pandemic secondary to insurance issues) tested positive for LTB with two positive QuantiFERON assays (Figure 1), no active TB symptoms, and a negative chest X-ray. Once weekly INH 900 mg/rifapentine 900 mg/pyridoxine 25 mg with an additional 50 mg DTG was initiated for 12 weeks. DTG Ctrough and VL monitoring occurred on day 10-, 39-, and 1-month post treatment. The initial DTG Ctrough was therapeutic with the patient incorrectly taking rifapentine (150 mg daily). The patient completed the course correctly and on LTB day 39 had a reduced DTG Ctrough to 300 ng/mL with a slight VL rebound. One month after LTB treatment completion, a Ctrough returned to baseline with VL suppression. Timeline and therapeutic drug monitoring for concurrent rifapentine and dolutegravir 100 mg.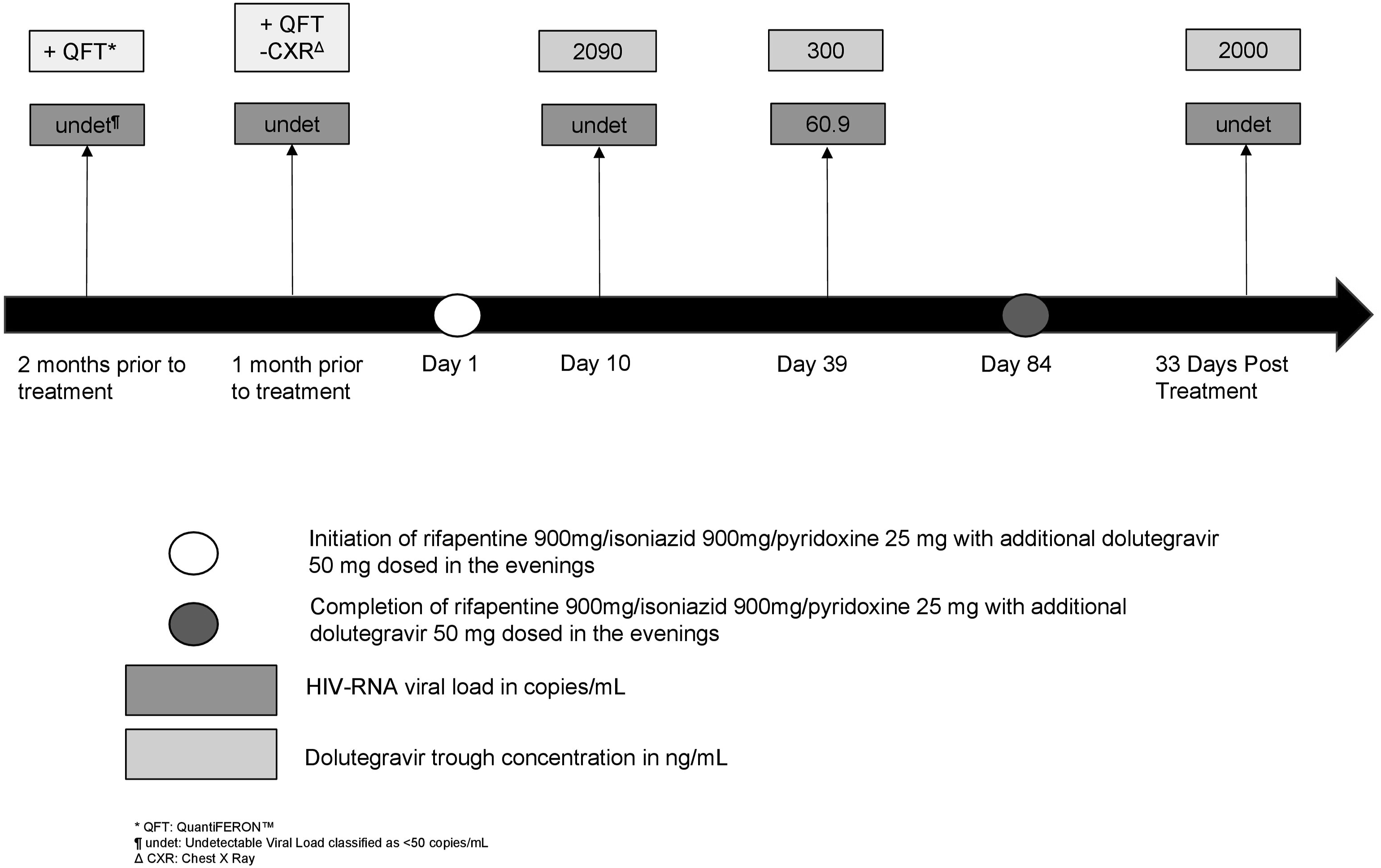
Discussion
The current case suggests an alternative dosing strategy (DTG 100 mg) when used with weekly rifapentine/INH to maintain therapeutic concentrations. Similar to rifapentine, a PK model supporting a DTG 100 mg QD dose suggests similar results maintaining Ctroughs of approximately 220 ng/mL when dosed with rifampin. 5 Additional support for increased DTG dosing was presented with A5372 (N = 25 PLWH) evaluating QD rifapentine 600 mg/INH 300 mg and DTG 50 mg BID for 28 days. 6 At week 4, DTG’s clearance increased from 0.68 L/hr to 1.39 L/hr with reduced Ctrough, but maintained values >158 ng/mL. A5372 compared PK data to the DOLPHIN study. DTG Ctroughs in the DOLPHIN study declined to <158 ng/mL in 2 patients, with increased clearance of 1.37 L/hr (similar to A5372) suggesting dosing inadequacies with QD DTG 50 mg and rifapentine.
In addition to increased DTG clearance, VL suppression rates are reduced with concurrent DTG/rifapentine. 7 453 PLWH receiving QD dolutegravir 50 mg/lamivudine 300 mg/TDF 300 mg (TLD) with 163 participants initiated simultaneously on weekly rifapentine/INH were evaluated. VL suppression rates (<50 copies/mL) at 6 months (3 months after completing LTB treatment) were reduced (66.9%) compared to PLWH who received TLD alone (77.4%, p = .03). At 12 months, VL suppression rates were similar.
Two case reports suggest the necessity of VL and therapeutic drug monitoring (TDM) in PLWH on concurrent DTG and rifamycins.8,9 The first case describes a PLWH and active TB treated with QD DTG 50 mg/FTC/TDF combined with four-drug treatment including rifabutin. 8 DTG concentrations remained therapeutic (>1000 ng/mL), but at week 3 and 26, reduced values (<100 ng/mL and approximately 200 ng/mL, respectively) were reported with rebound viremia and genotypic resistance [nucleoside reverse transcriptase inhibitor (NRTI): M184I/V; INSTI: G118R, R263K]. An ARV switch at week 35 resulted in VL control. 8 Resistance mutations were detected at low frequencies (<0.2%) at baseline, suggesting INSTI resistance developed as a result of inadequate DTG concentrations. In a second case, a newly diagnosed PLWH with a lumbar spine infection requiring rifampin, was initiated on DTG 50 mg BID and FTC/TDF. 9 An initial VL response resulted with subsequent rebound requiring an alternative ARV regimen of boosted darunavir to achieve suppression. Stored sample analysis demonstrated reduced DTG concentrations with resistance (NRTI: M184I/V; INSTI: E157Q, R263K).
These previously reported cases and the A5372 data demonstrate increased DTG clearance and suggestions for incorporation of TDM with concurrent rifapentine. This case adds to existing PK and VL suppression data supporting an alternative dosing strategy (DTG 100 mg) when administered with weekly rifapentine to maintain adequate concentrations, avoid VL rebound, and improve ARV adherence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.