
Abstract
Background
The Community Liver Health Checks Programme offers population-level screening to identify those with fibrosis or cirrhosis. In this study, we describe the population characteristics and results for our cohort to ascertain the clinical utility of routine FibroScan.
Methods
Prospective observational study of PLWH who had a FibroScan as part of the programme. All participants had risk factor(s) for liver fibrosis.
Results
A total of 382 people were included in the study. There were 291 males, with a median age of 48 years (range 26–75). Half (n = 191) were white British, and 31.4 % (n = 120) were Black African. Sixty-two percent (n = 237) were men who have sex with men (MSM). Median time since HIV diagnosis was 16 years, with a median CD4 of 642. Ninety-five percent were undetectable. The most common indication for FibroScan referral was BMI >30 in 47.4% (n = 181). Other common indications include NAFLD (31%, n = 118), Alcohol (27.1%, n = 103). 24.9% (n = 95) had more than two risk factors. Overall, 53.7% (n = 205) had evidence of steatosis (≥S1), 19.4% (n = 74) had evidence of fibrosis (≥F1), and 1% (n = 4) had evidence of cirrhosis. In bivariate analysis, BMI >30 and a known diagnosis of NAFLD were associated with steatosis (≥S1) (OR 3.1 and 1.8 respectively). Of those with multiple risk factors (≥2), 74.7% (n = 71) had evidence of steatosis, 20% (n = 19) had evidence of fibrosis, 2.1% (n = 2) had evidence of cirrhosis. Bivariate analysis shows a significant correlation between the presence of multiple risk factors and ≥F1 fibrosis (OR = 2.3) and ≥S1 steatosis (OR = 3.2).
Conclusions
Our data shows a low prevalence of liver cirrhosis, increasing in the presence of multiple liver risk factors. We recommend FIB-4 score as an inexpensive primary screening tool for fibrosis/cirrhosis, and Fibroscan for those with multiple risk factors or high FIB-4 score.
Introduction
The Community Liver Health Checks is a programme of the National Health Service (NHS) - the United Kingdom’s publicly funded healthcare system - aimed at using transient elastography (TE) as a first-line screening tool to improve detection of liver fibrosis and cirrhosis and support early diagnosis of cancer at population level. 1 Launched in 2022, the service is free at the point of access and all persons with established liver risk factors are eligible. These risk factors include past/current hepatitis C infection, hepatitis B infection, long term excess alcohol use, obesity or diabetes. The programme uses mobile scanners to bring the service directly to communities including GP practices, food banks, and other public spaces. 2 Initial pilot programmes found that 1 in 10 people screened in high-risk areas had advanced fibrosis or cirrhosis. By August 2025, almost 113,000 people had a Fibroscan of their liver performed, and almost 8500 referred on for further investigations to delineate liver morphology (e.g. the presence of cirrhosis) and to exclude hepatocellular carcinoma. The Faster Diagnosis Standard which measures the percentage of people who have hepatocellular carcinoma ruled out or diagnosed reached a peak of 76.8% in June 2025, the highest June since the standard was introduced. 3
NICE (National Institute for Health and Care Excellence) recommends this community strategy to screen more people outside secondary or specialist care, and thereby improve access for underserved communities, but recognises there is limited evidence on the performance of TE in these alternative settings due to uncertain disease prevalence in different populations. 4
The prevalence of liver disease among PLWH is highly variable depending on geography and assessment methods used, with one study based on elastography assessment describing the prevalence of significant fibrosis (TE >7.2 kPa indicating F2 and above) in untreated HIV-positive individuals to be 7.8%. 5 Another study performed liver biopsy of PLWH at baseline and found 43% already had some degree of liver fibrosis. 6 Current guidelines for liver fibrosis/cirrhosis screening recommend 2–3 yearly monitoring of risk using non-invasive fibrosis tests and calculation of fibrosis scores (eg FIB-4) to guide risk stratification of the presence of liver disease among PLWHIV. 7 Those with a FIB-4 score less than 1.3 are deemed low risk, while those with a score of between 1.3 and 2.67 may proceed to transient elastography (TE).
In this service evaluation, we describe the population characteristics and TE outcomes of PLWH who underwent TE as first-line screening to determine the clinical utility of targeted TE at population level.
Methods
Study design and patient selection
We undertook a retrospective case note review of PLWH attending three sexual health clinics based in Manchester. Participants were seen during routine follow-up between November 2022 and June 2024. All FibroScan assessments performed during the study period were extracted from the electronic health record system. The study aimed to evaluate the prevalence of liver fibrosis and steatosis, identify associated metabolic and behavioural risk factors, and assess the relationship between antiretroviral therapy (ART) exposure and liver outcomes.
Data collection and definitions
Liver risk factors
The presence of recognised liver disease risk factors was extracted from clinical review notes and coded as follows: • Obesity: body mass index (BMI) > 30 kg/m2 • Non-alcohol fatty liver disease (NAFLD) risk: clinical diagnosis or documentation of fatty liver disease • Alcohol use: alcohol consumption recorded as exceeding 14 units/week • Other risk factors: viral hepatitis coinfection, diabetes, or metabolic syndrome where present
Patients were categorised as having multiple risk factors if they had two or more of the above.
Transient elastography
Liver fibrosis and steatosis were assessed by FibroScan® using the M or XL probe according to manufacturer guidelines. Results were reported using standard thresholds: • Fibrosis: F0–F4 staging; significant fibrosis defined as ≥F1; high-grade fibrosis as F3–F3/4; cirrhosis as F4 • Steatosis: S0–S3 staging; clinically relevant steatosis defined as ≥S1
Antiretroviral therapy exposure
ART regimens at the time of FibroScan were recorded, with specific attention to: • Current use of tenofovir alafenamide (TAF) in combination with an integrase strand transfer inhibitor (INSTI) • Historical exposure to older nucleoside analogues, particularly didanosine or stavudine
ART exposure was categorised as current, past, or none, based on documented treatment history.
Statistical analysis
Descriptive analysis of demographics data, liver risk factors and Fibroscan outcomes was completed using Microsoft Excel. Continuous variables were reported as medians and ranges, and categorical variables as counts and percentages.
Bivariate logistic regression was performed to evaluate the association between: 1 .Multiple (≥2) liver risk factors and the presence of significant fibrosis (≥F1) and steatosis (≥S1) 2 .Exposure to Tenofovir alafenamide (TAF) plus an integrase strand inhibitor (INSTI) and steatosis (≥S1) 3 .Exposure to historical ART agents (didanosine or stavudine) and liver outcomes
Odds ratios (ORs), 95% confidence intervals (CIs), and p-values were reported. Statistical analyses were conducted using Statistical Package for the Social Sciences (SPSS) version 29, with a pre-specified significance level (α) of <0.05.
Ethical considerations
As a service evaluation project, this work did not fall under the remit of the NHS Health Research Authority (HRA); therefore, formal ethical approval was not required as per UK HRA decision tool: https://www.hra-decisiontools.org.uk/ethics/
Results
Population characteristics
Demographic data of patients included.
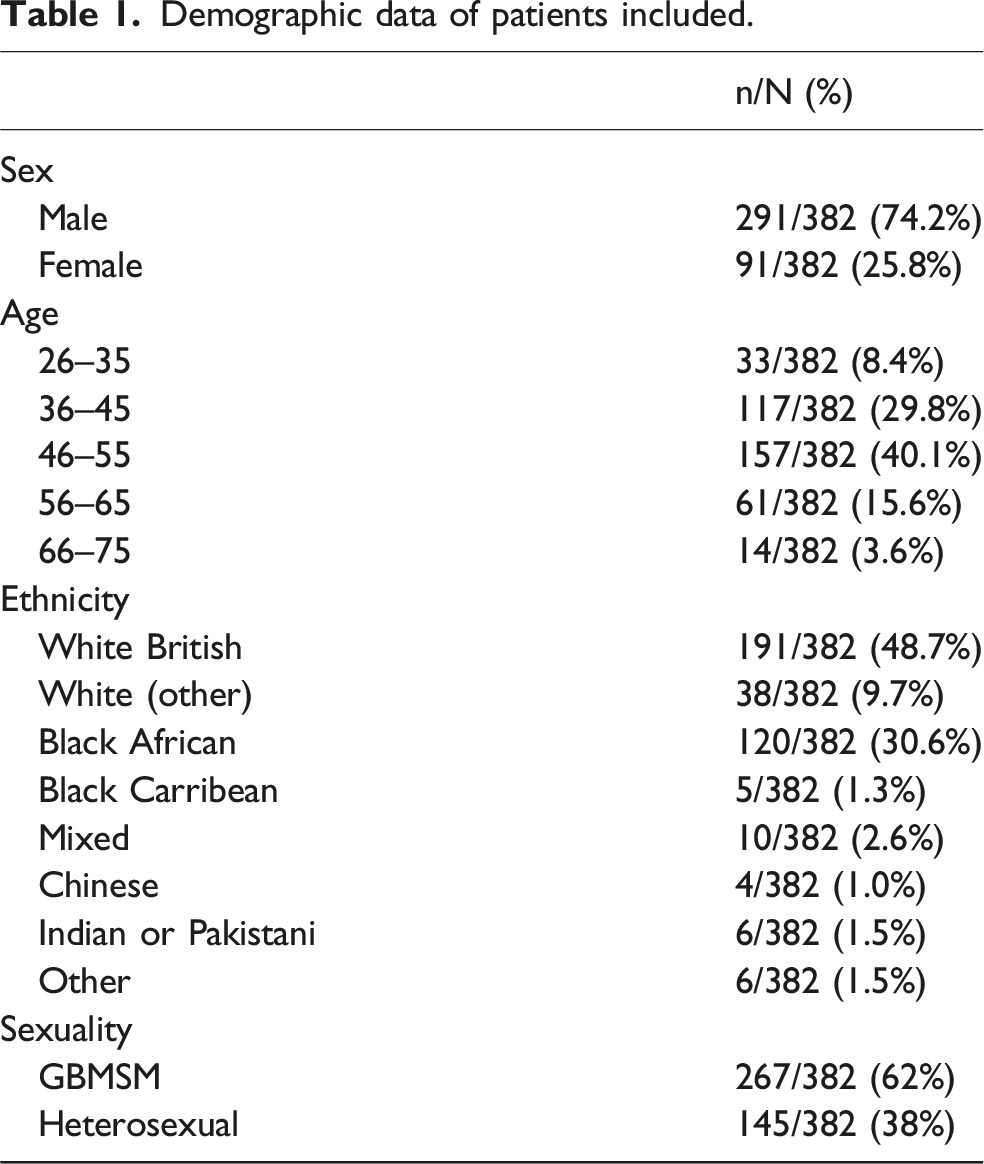
The median time since HIV diagnosis is 16 years (range 26–75 years), with a median CD4 count of 641 cells/µL (range 127–6354 cells/µL). 95% had undetectable HIV viral load at time of scanning.
Liver risk factors
As depicted in Figure 1, the most common indication for FibroScan referral was BMI >30 in 47.4% (n = 181/382). Other common indications include NAFLD (31%, n = 118/382), alcohol (27.1%, n = 103/382). Number of patients per risk factor for liver fibrosis.
24.9% (n = 95/382) had two or more risk factors.
Transient elastography results
As illustrated in Figure 2, 19.4% (n = 74/382) had evidence of fibrosis (≥F1). The rate of high-grade fibrosis (F3, F3–F4) was 3.1% (n = 12/382) and 1% (n = 4/382) had evidence of cirrhosis (F4) (see Figure 1). 53.7% (n = 205/382) had evidence of steatosis (≥S1). Number of patients per grade of fibrosis as determined by transient elastography scanning.
Of those with multiple liver risk factors (≥2), 74.7% (71/95) had evidence of steatosis, 20% (19/95) had evidence of fibrosis, 2.1% (2/95) had evidence of cirrhosis. Bivariate analysis shows a significant correlation between the presence of multiple risk factors and ≥ F1 fibrosis (OR = 2.3, 95% CI: 1.2–4.4, p = 0.008) and ≥ S1 steatosis (OR = 3.2, 95% CI: 2.0–5.7, p < 0.001).
Impact of antiretrovirals
Of the 82 persons on tenofovir alafenamide (TAF) and an integrase inhibitor, there was no association with fibrosis (p = 0.326), and only a borderline inverse association with steatosis (OR = 0.6, 95% CI: 0.363–0.993, p = 0.046). Of the 12 persons with historical exposure to didanosine, there was no association with the development of liver fibrosis or steatosis (p = 0.711 and p = 0.0.581 respectively). Similarly, for those with historical exposure to stavudine (n = 16/382), there was no association with the development of fibrosis (p = 0.884) or steatosis (p = 0.548).
Discussion
Metabolic dysfunction-associated steatotic liver disease (MASLD) is now the most common cause of chronic liver disease. 8 The European Association for the Study of the Liver (EASL) have updated their nomenclature for NAFLD, describing the spectrum of MASLD as ranging from steatosis and metabolic dysfunction-associated steatohepatitis (MASH, formerly NASH), through fibrosis/cirrhosis to MASH -related hepatocellular carcinoma. This change closely aligns MASLD to other cardiometabolic risk factors including obesity and T2DM. The prevalence of MASLD is expected to rise, and with it, liver-related mortality. Already, the UK saw deaths from liver disease rise by 27% between 2019 and 2023. 9
Our data show that almost half of all participants had a BMI over 30, with a third of participants diagnosed with NAFLD. The prevalence of obesity in our cohort is higher than the average of 27.1% for adults over 18 years in Greater Manchester, England. 10 This highlights the high prevalence of metabolic risk factors, and the need for close monitoring of liver risk.
Despite the high prevalence of obesity, the detection rates of high-grade fibrosis and cirrhosis among PLWH with a single liver risk factor is low. Detection rates however increased in the presence of multiple liver risk factors, and we therefore recommend FIB-4 score for those with single liver risk factor, and TE for those with multiple risk factors or elevated FIB-4 score.
European AIDS Clinical Society (EACS) provide a useful resource for evaluating PLWH at risk of MASLD and recommend 2–3 yearly assessment with a liver risk scoring system such as FIB-4 or Non-alcoholic fatty liver disease Fibrosis Score (NFS), with those at intermediate risk recommended for further serologic or imaging assessment with elastography.
The lack of association between historic use of hepatotoxic antiretrovirals is likely due to insufficient data on duration on these antiretrovirals as well as small numbers of persons on this regimen. Other pharmacologic studies have demonstrated a causal relationship between stavudine and didanosine and the development of microvesicular steatotic injury.11–13
Limitations
Our service evaluation was limited to one geographical location and as such may not be generalisable to the rest of the UK or indeed, internationally. It is also important to interpret the results in the light of low patient numbers for certain risk factors such as historic didanosine or stavudine use.
Footnotes
Acknowledgements
The authors wish to thank the technical team for their help in extracting the required data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.