
Abstract
Background
There are limited data available regarding the efficacy of long-acting injectable antiretroviral (LAI) treatment [cabotegravir/rilpivirine] in individuals with HIV viral suppression where baseline genotypic resistance is unknown. 1
HIV proviral DNA genotypic resistance sequencing can detect archived HIV resistance mutations in individuals with low-level viremia or complete viral suppression. British HIV Association (BHIVA) and European AIDS Clinical Society (EACS) guidelines do not recommend proviral DNA genotypic resistance testing in the absence of baseline HIV resistance. 2 Locally, we have a clinical cohort of approximately 2400 individuals living with HIV and at the start of LAI rollout, began routinely requesting proviral DNA genotypic resistance testing for all individuals being considered for LAI when HIV resistance data or subtype were unavailable. The presence of proviral resistance mutations to cabotegravir or rilpivirine precluded patients from being offered LAI therapy.
The aim of this pilot review was to explore the prevalence of significant resistance mutations from proviral DNA genotypic resistance reports from virologically supressed individuals who were being assessed for LAI treatment with no baseline resistance data.
Method
Using our clinic electronic patient record system, we identified individuals who were being considered for LAI between June 2022 and January 2024 who were virologically suppressed and had no baseline resistance data – but instead, had proviral genotyping requested. Data were extracted including proviral resistance mutations, HIV sub-type and date of HIV diagnosis. Mutations were analysed using the Stanford HIV Drug Resistance Database. 3
Results
APOBEC & significant mutations to cabotegravir/rilpivirine detected from proviral resistance genotyping.
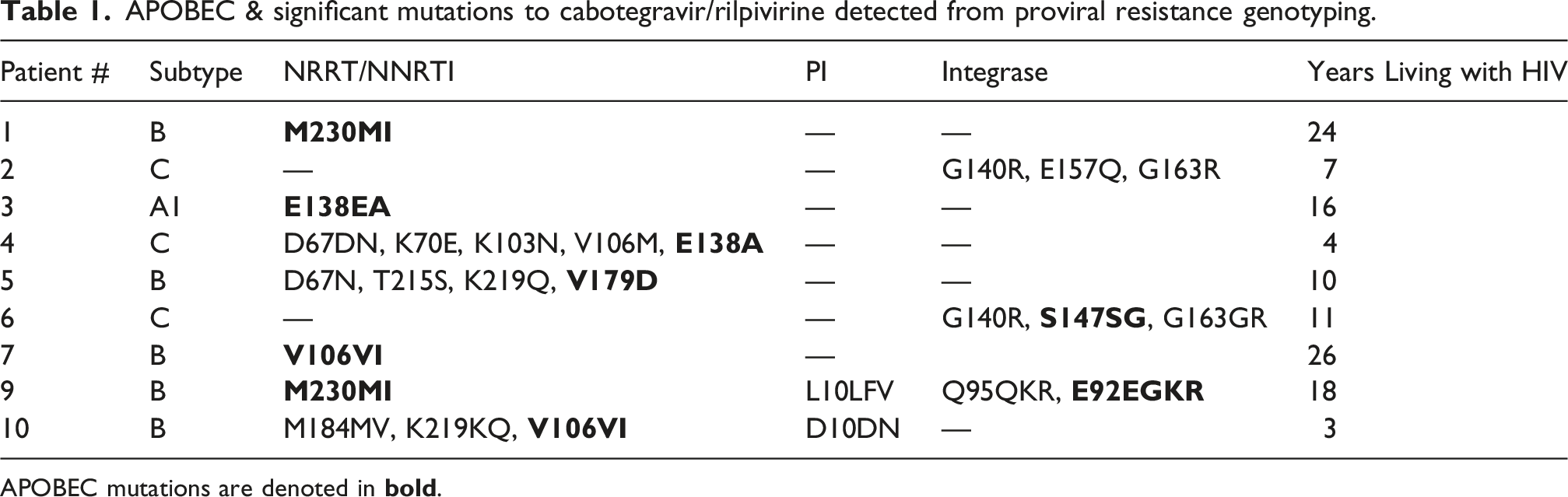
APOBEC mutations are denoted in
Discussion
These data suggest that proviral DNA genotypic resistance testing offer limited benefit for individuals considering LAI therapy in the absence of baseline resistance. Proviral DNA mutations may represent archived viral variants that are no longer replication-competent, which could lead to an overestimation of resistance. Conversely, proviral genotyping may fail to detect low-level or minor resistant variants that could still be clinically significant. 3
HIV viral APOBEC mutations are caused by the human enzyme APOBEC3G, which changes or deaminates cytosine to uracil in the viral DNA, causing G-to-A mutations in the viral RNA genome making it unable to replicate effectively. 4 The interpretation of APOBEC mutations in virologically suppressed patients remains uncertain and could further complicate clinical decision-making as it is likely that APOBEC mutations have no impact on the effectiveness on antiretroviral therapies in virologically supressed individuals. 5 Therefore, a detailed review of previous treatment history, adherence, and virological outcomes should remain key in antiretroviral decision making. However, proviral DNA testing can provide valuable insight in determining HIV subtype and avoiding LAI therapy use in individuals with subtype A6 combined with BMI >30 kg/m2, where significantly reduced treatment efficacy has been reported.
This study has several limitations. As a single-centre pilot analysis with a small sample size, the findings may not be generalisable, and the estimates of resistance prevalence are associated with wide confidence intervals. The retrospective design and absence of clinical outcome data following LAI initiation mean that the clinical relevance of detected proviral resistance mutations cannot be determined. In addition, proviral DNA sequencing may both overestimate resistance through detection of non-replication-competent variants and fail to identify low-frequency resistant species.
Conclusion
In this single-centre pilot analysis, 17% of individuals being assessed for long-acting ART with a suppressed HIV viral load had evidence of cabotegravir/rilpivirine resistance from proviral DNA genotypic resistance testing. The significance of this is unclear, but more work is needed to understand how to safely implement injectable HIV treatment in individuals without baseline HIV resistance testing.
Footnotes
Ethical consideration
No ethical approval was required for this retrospective anonymous clinical review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Colin Fitzpatrick is a colleague of the Editor-in-Chief of the journal, Professor Daniel Richardson. Professor Daniel Richardson did not take part in the manuscript handling, peer review or decision-making process for this submission which was handled by the associate editor, Dr Claire Broad.
Data Availability Statement
Data available on request.