
Abstract
Bullying is a serious problem for schools, parents, and public-policymakers alike. Bullying creates risks of health and social problems in childhood, but it is unclear if such risks extend into adulthood. A large cohort of children was assessed for bullying involvement in childhood and then followed up in young adulthood in an assessment of health, risky or illegal behavior, wealth, and social relationships. Victims of childhood bullying, including those that bullied others (bully-victims), were at increased risk of poor health, wealth, and social-relationship outcomes in adulthood even after we controlled for family hardship and childhood psychiatric disorders. In contrast, pure bullies were not at increased risk of poor outcomes in adulthood once other family and childhood risk factors were taken into account. Being bullied is not a harmless rite of passage but throws a long shadow over affected people’s lives. Interventions in childhood are likely to reduce long-term health and social costs.
Keywords
Introduction
Psychologists, economists and policymakers are interested in how early inputs in the life cycle affect later productivity (Heckman, 2006). Children’s psychological problems (Goodman, Joyce, & Smith, 2011) or exposure to abuse (Currie & Spatz Widom, 2010) impact functioning decades later in adulthood. There is little information, however, about the long-term effects of problematic peer relationships, although schoolchildren spend more time, at school or out of school, with their peers than with their parents.
Bullying is systematic abuse of power and refers to repeated aggression against another person that is intentional and involves an imbalance of power (Olweus, 1994). The repeated aggression can be either direct (e.g., name calling, beating) or relational, that is, with the intent to damage relationships (e.g., spreading rumors; Wolke, Woods, Bloomfield, & Karstadt, 2000). Children can be perpetrators or victims of bullying, and some children both bully and get victimized (bully-victims). Being bullied or bullying others is a relatively common experience in childhood and adolescence (Nansel et al., 2001).
Children who are withdrawn, physically weak, or prone to show a reaction (e.g., run away, become upset), who have poor social understanding (Woods, Wolke, Nowicki, & Hall, 2009), or who have few or no friends who can stand up for them (Wolke, Woods, & Samara, 2009) (Arseneault, Bowes, & Shakoor, 2010) are more likely to become victims of bullying at school. Victims of bullying are at increased risk of adverse outcomes in childhood, including physical health problems, emotional and psychological problems (Reijntjes, Kamphuis, Prinzie, & Telch, 2010), and reduced academic achievement (Arseneault et al., 2010; Nakamoto & Schwartz, 2010). The poorer educational attainment of victims in childhood may have adverse effects on income across adulthood (Brown & Taylor, 2008).
In contrast, pure bullies are often strong, healthy children (Wolke, Woods, Bloomfield, & Karstadt, 2001), and some research has suggested that they are competent in emotion recognition (Woods et al., 2009) and social understanding and effective in manipulating others (Sutton, Smith, & Swettenham, 1999). They have high social impact in school despite being controversial (i.e., liked by some children but disliked by their victims), come from disturbed families, and are deviant in their behavior but not emotionally troubled (Juvonen, Graham, & Schuster, 2003). Bullies, particularly those who are boys (Sourander et al., 2011), have been reported to be at increased risk for later offending (Ttofi, Farrington, Lösel, & Loeber, 2011).
It is bully-victims, those who are victims of bullying but also bully others, that seem to be the most troubled: impulsive, easily provoked, low in self-esteem, poor at understanding social cues, and unpopular with peers (Arseneault et al., 2010). Bully-victims are also more likely to come from dysfunctional families (Lereya, Samara, & Wolke, 2013) or have preexisting behavioral or emotional problems, and it has been suggested that these factors, rather than bullying per se, may explain their outcomes in adulthood (Sourander et al., 2009).
Finally, there is some evidence for a dose-response relationship between duration of being bullied and adverse outcomes in childhood. Those who are chronically bullied by peers (i.e., over the course of years), compared with those bullied at one time point only, have been reported to have a higher risk for adverse outcomes, such as psychiatric problems in childhood (Schreier et al., 2009; Winsper, Lereya, Zanarini, & Wolke, 2012).
This was the first study to investigate how involvement in childhood bullying and chronicity of being bullied affect a range of adult outcomes, including health, risky or illegal behavior, wealth, and social relationships. We tested the unique contributions of exposure to bullying in different roles, above and beyond the effects of adverse family relationships and pre- or coexisting psychiatric problems in childhood.
Method
Sample
The Great Smoky Mountain Study is a population-based study of three cohorts of children, aged 9, 11, and 13 at intake, recruited from 11 counties in western North Carolina in 1993 using a multi-stage-household, equal-probability/accelerated-cohort design (see Fig. 1; for full details of the study, see Costello et al., 1996). Of all subjects recruited, 80% (n = 1,420) agreed to participate in the present study. The weighted sample was 49.0% female and 51% male.

Schematic illustrating subject recruitment and the subject-ascertainment strategy in the Great Smoky Mountain Study (Costello et al., 1996).
Annual assessments were completed with the subject and his or her primary caregiver until he or she reached age 16 and then with the subject again at ages 19, 21, and 24 to 26 years (M = 25.0 years, SD = 0.79). An average of 83% of possible interviews was completed overall (range = 75%–94%). Before interviews, participants signed informed-consent forms approved by the Duke University Medical Center institutional review board.
Of the 1,420 subjects assessed in childhood, 1,273 (89.6%) were followed up in young adulthood. Follow-up rates were similar across groups (bullies: 100 of 112 subjects, 89.3%; victims: 305 of 335 subjects, 91.0%; bully-victims: 79 of 86 subjects, 91.9%; subjects not involved in bullying: 789 of 887 subjects, 89.0%). There were no differences in follow-up rate between the not-involved-in-bullying group and any of the three other groups (subjects not involved in bullying vs. bullies, p = .39; subjects not involved in bullying vs. victims, p = .95; subjects not involved in bullying vs. bullies, p = .93).
Measures of childhood bullying and victimization
At each assessment when subjects were between the ages of 9 and 16, the child and his or her parent reported on whether the child had been bullied or teased or had bullied others in the 3 months prior to the interview as part of the Child and Adolescent Psychiatric Assessment (Angold & Costello, 1995, 2000; full definitions are provided in Table 1). Being bullied or bullying others was counted if it was reported by either the parent or the child at any childhood or adolescent assessment. If the informant reported that the subject had been bullied or had bullied others, then the informant was asked separately how often the bullying had occurred in the prior 3 months in the following three settings: home, school, and the community. Our focus in the current study was peer bullying in the school context only. Parent and child agreement on peer bullying (κ = .24) was similar to that of other measures of bullying (Schreier et al., 2009). Although this level of agreement may seem low, a large meta-analysis of data on parent-reported and self-reported behavioral and emotional functioning of children showed similar concordance levels (Achenbach, McConaughy, & Howell, 1987).
Definitions and Interview Probes for Bullying and Being Bullied in Childhood

Note: The interviewer began by asking the standard questions shown in the Interview Questions column, but he or she could ask additional questions to ensure that the definition was met in full. When the subject reported being bullied, the interviewer asked who the perpetrator was (siblings or peers). Only peer bullying was coded for this study. Frequency and onset of bullying or being bullied (i.e., the age when it had started) were also assessed.
All subjects were categorized as victims only (i.e., they never indicated at any assessment that they had bullied others; n = 335; 23.6%), bullies only (i.e., they never indicated that they had been a victim of bullying; n = 112; 7.9%), bully-victims (i.e., they had indicated that they bullied others and had been victims of bullying at any of the assessments; n = 86; 6.1%), or not involved in bullying (n = 887; 62.5%). Compared with the not-involved-in-bullying group (52.2% female, 47.8% male), both bully-victims and bullies were more likely to be male, but victim status did not differ by sex (bully-victims: 72.4% male, p = .009; bullies: 69.1% male, p = .02; victims: 52.9% male, p = .34). For both victims and bully-victims, it was relatively common to report having been bullied at more than one time point (all percentages shown here are weighted percentages): 159 children and adolescents (120, or 31.9%, of those in the victim group, and 39, or 43.6%, of those in the bully-victim group; not significantly different, p = .24) reported being bullied at more than one assessment point (chronic victims). The groups also did not differ in terms of the percentage of subjects who reported being bullied at three or more assessments.
Assessment of adult outcomes
All outcomes except for officially recorded criminal offenses were assessed through interviews with the subjects when they were young adults, using the Young Adult Psychiatric Assessment (Angold et al., 2012). The four broad domains were health, risky or illegal behaviors, wealth, and social relationships.
Health
Participants reported whether they had been diagnosed with a serious physical illness or been in a serious accident at any point during young adulthood and whether they had had a sexually transmitted disease (i.e., a positive test result for herpes, genital warts, chlamydia, or HIV). Weight and height measurements were used to derive body mass index, with obesity defined as a body mass index greater than or equal to 30 kg/m2. Participants were assessed for a Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), psychiatric diagnosis (any DSM-IV anxiety disorder, any depressive disorder, and antisocial personality disorder). Regular smoking was defined as smoking one or more cigarettes per day for 3 months. Self-reported perceived poor health, high illness-contagion risk, and slow illness recovery were derived from a physical-health-problems survey (National Center for Health Statistics, 1988).
Risky or illegal behaviors
Official felony charges were garnered from North Carolina Administrative Office of the Courts records. Self-report data were used to assess recent police contact; frequent lying to others; frequent physical fighting; breaking into a home, business, or property; frequent drunkenness (drinking to excess at least once weekly for 3 months); recent use of marijuana or other illegal substances; and frequency of one-time sexual encounters with strangers (“hooking up” with strangers for a one-night stand).
Wealth: financial and educational accomplishments
Poverty was coded using thresholds based on income and family size issued by the U.S. Census Bureau (2012). Failure to complete high school and completion of any college education were coded on the basis of the subject’s educational status at the last adult assessment. Job problems were assessed as being dismissed or fired from a job and quitting a job without financial preparations. Finally, other financial problems assessed were failing to honor debts or financial obligations and being a poor manager of one’s finances.
Social relationships
Marital, parenthood, and divorce status were determined through self-report at the last adult assessment. The quality of the subject’s relationship with his or her parents, spouse or significant other, and friends (including arguments or violence) was assessed at each assessment. Variables were included to indicate any violence in a romantic relationship, a poor relationship with one’s parents, absence of a best friend or confidante, and problems making or keeping friends.
Assessment of childhood hardships
Childhood hardships were assessed using dichotomized risk scales for the following factors: low socioeconomic status (SES; Nakao & Treas, 1992), unstable family structure (presence of two or more of the following indicators: single-parent structure, stepparent in household, parental divorce, parental separation, or change in parenting structure), maltreatment (any of the following indicators: sexual abuse, physical abuse, neglect), and family dysfunction (five or more of the following indicators: inadequate parental supervision; overinvolvement of a parent; physical violence between parents; high frequency of parental arguments; parental marital relationship characterized by absence of affection, apathy, or indifference; distress caused by or active involvement in arguments between parents; high maternal scores on depression questionnaire; high frequency of arguments between parent and child; and tense parent-child interactions (codebooks for all items are available at http://devepi.duhs.duke.edu/codebooks.html).
Childhood psychiatric problems
Childhood psychiatric variables were assessed when subjects were between 9 and 16 years of age (Costello, Mustillo, Erkanli, Keeler, & Angold, 2003) and consisted of the following DSM-IV diagnoses: any anxiety disorder, depressive disorders (the same as those assessed in adulthood), disruptive behavior disorders (including conduct disorder, attention-deficit/hyperactivity disorder, and oppositional defiant disorder), and substance-use disorder (including any abuse or dependence).
Analyses
All associations were tested using weighted regression models in a generalized-estimating-equations framework implemented in SAS PROC GENMOD. Robust variance (sandwich-type) estimates were used to adjust the standard errors of the parameter estimates for the sampling weights applied to observations. Bullies, victims, and bully-victims were compared with subjects who were not involved in any bullying in childhood. Negative primary outcomes were aggregated across each of the four domains (health, risky or illegal behaviors, wealth, and social relationships), and these scales were standardized (M = 0, SD = 1; i.e., the mean of 0 represents the mean score for each domain in the total sample). Role-in-bullying status predicted standardized domain scores in a series of weighted linear regression models (Fig. 2). For follow-up bivariate analyses of individual indicators within the four broad domains, logistic regression was used, and odds ratios and 95% confidence intervals are reported (Tables 2 and 3). Multivariable analyses (Table 4) involved the prediction of young-adult outcome variables by role-in-bullying status, controlling for childhood psychiatric variables and hardships that could have occurred prior to, concurrent with, or after the first reported incident of involvement in bullying. Table 5 shows the unadjusted and adjusted associations for single-time-point and chronic victims versus subjects who were not involved in bullying for each of the outcome domains in adulthood.
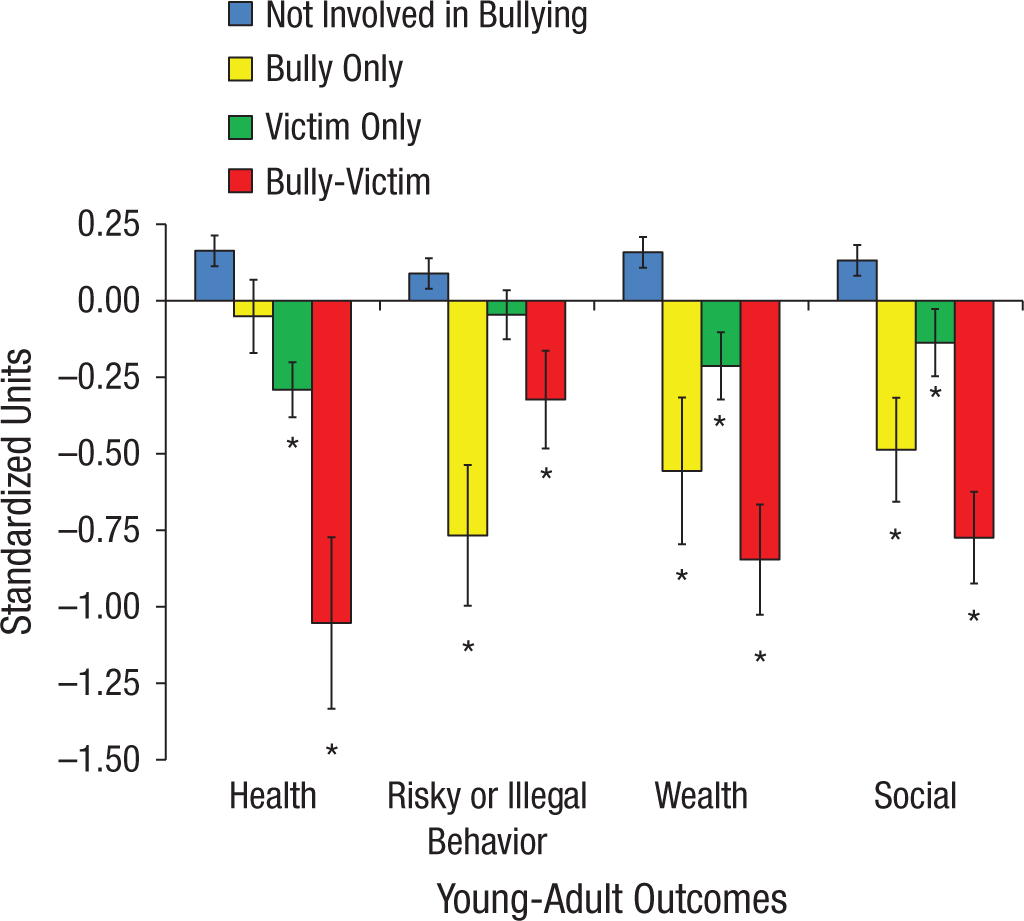
Associations between childhood role in bullying and young-adult standardized outcome scales (unadjusted for childhood family hardships and childhood psychiatric problems). Across all domains, negative scores indicate more problems than the mean for the total sample, and positive scores indicate fewer problems. Asterisks indicate significant differences from the not-involved-in-bullying group (p < .05).
Associations of Role in Bullying in Childhood With Health Functioning and Risky or Illegal Behaviors in Young Adulthood

Note: Values in brackets are 95% confidence intervals. OR = odds ratio.
Associations of Role in Bullying in Childhood With Financial and Social Functioning in Young Adulthood
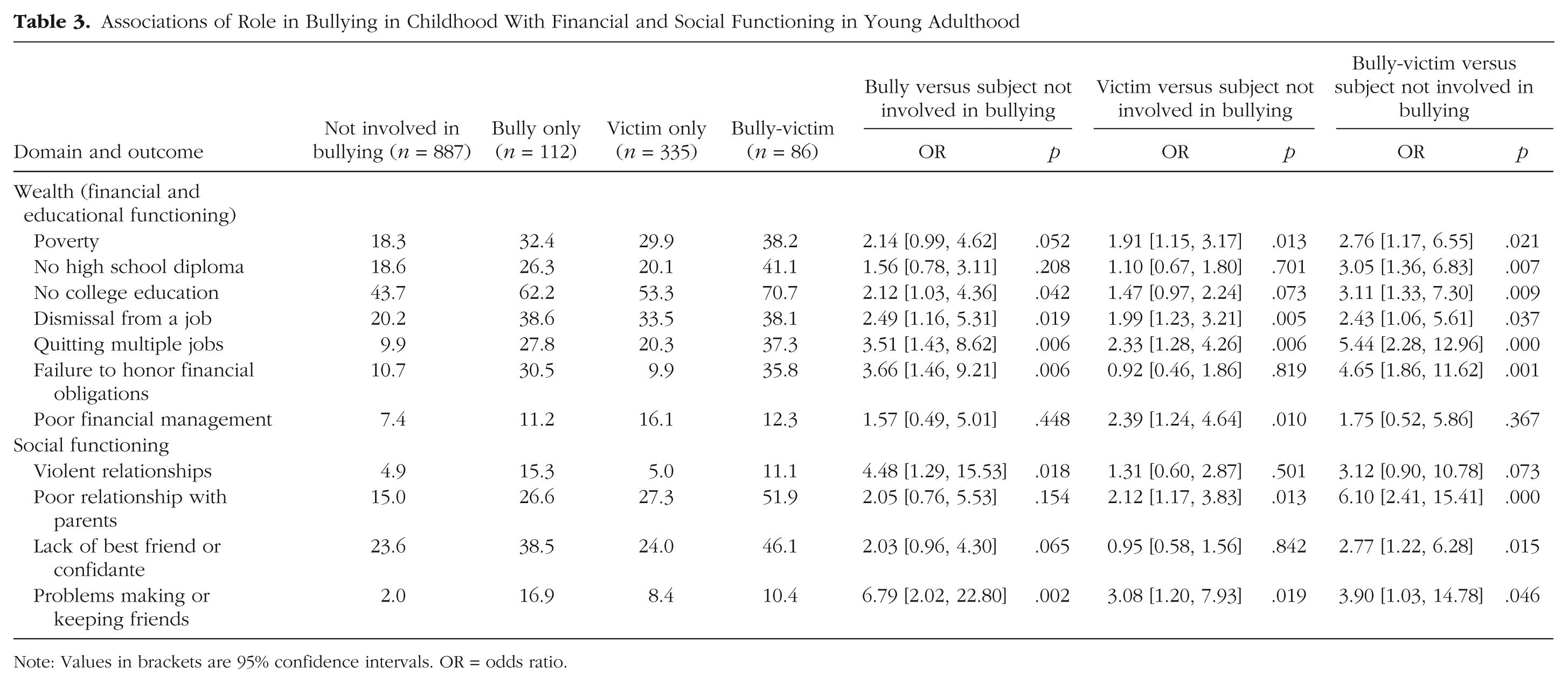
Note: Values in brackets are 95% confidence intervals. OR = odds ratio.
Associations of Role in Bullying in Childhood With Outcomes in Young Adulthood Accounting for Childhood Family Hardships and Childhood Psychiatric Problems
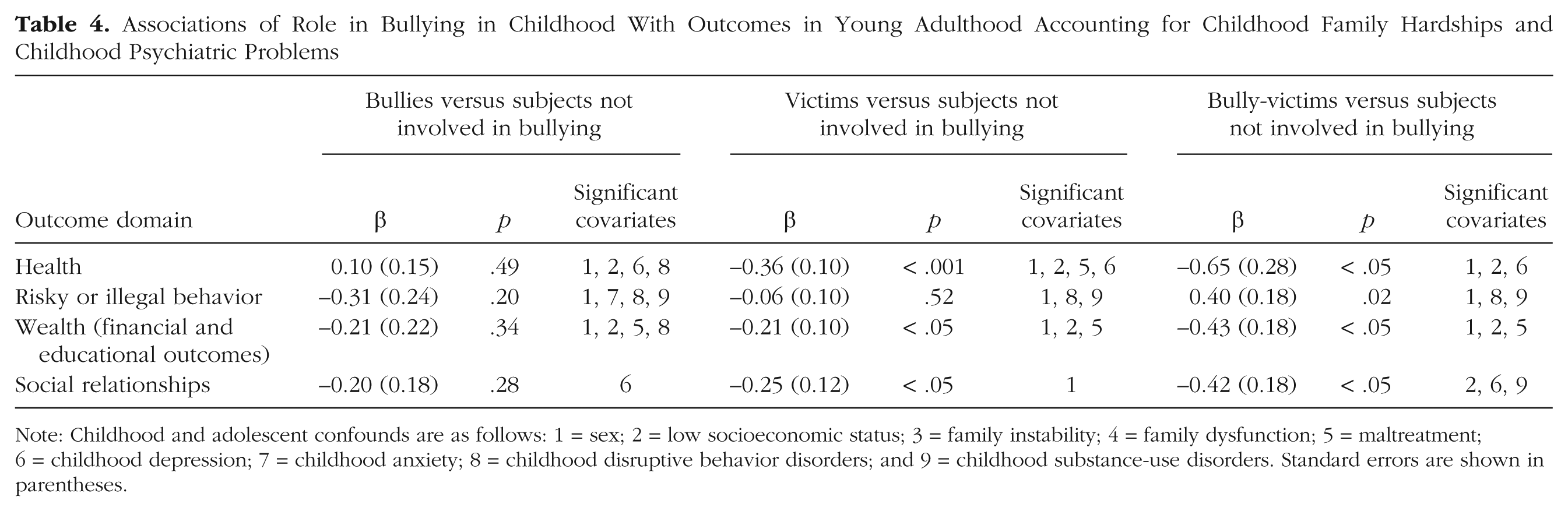
Note: Childhood and adolescent confounds are as follows: 1 = sex; 2 = low socioeconomic status; 3 = family instability; 4 = family dysfunction; 5 = maltreatment; 6 = childhood depression; 7 = childhood anxiety; 8 = childhood disruptive behavior disorders; and 9 = childhood substance-use disorders. Standard errors are shown in parentheses.
Raw and Adjusted Associations of Single-Time-Point and Chronic Bullying Victimization With Outcomes in Childhood and Young Adulthood
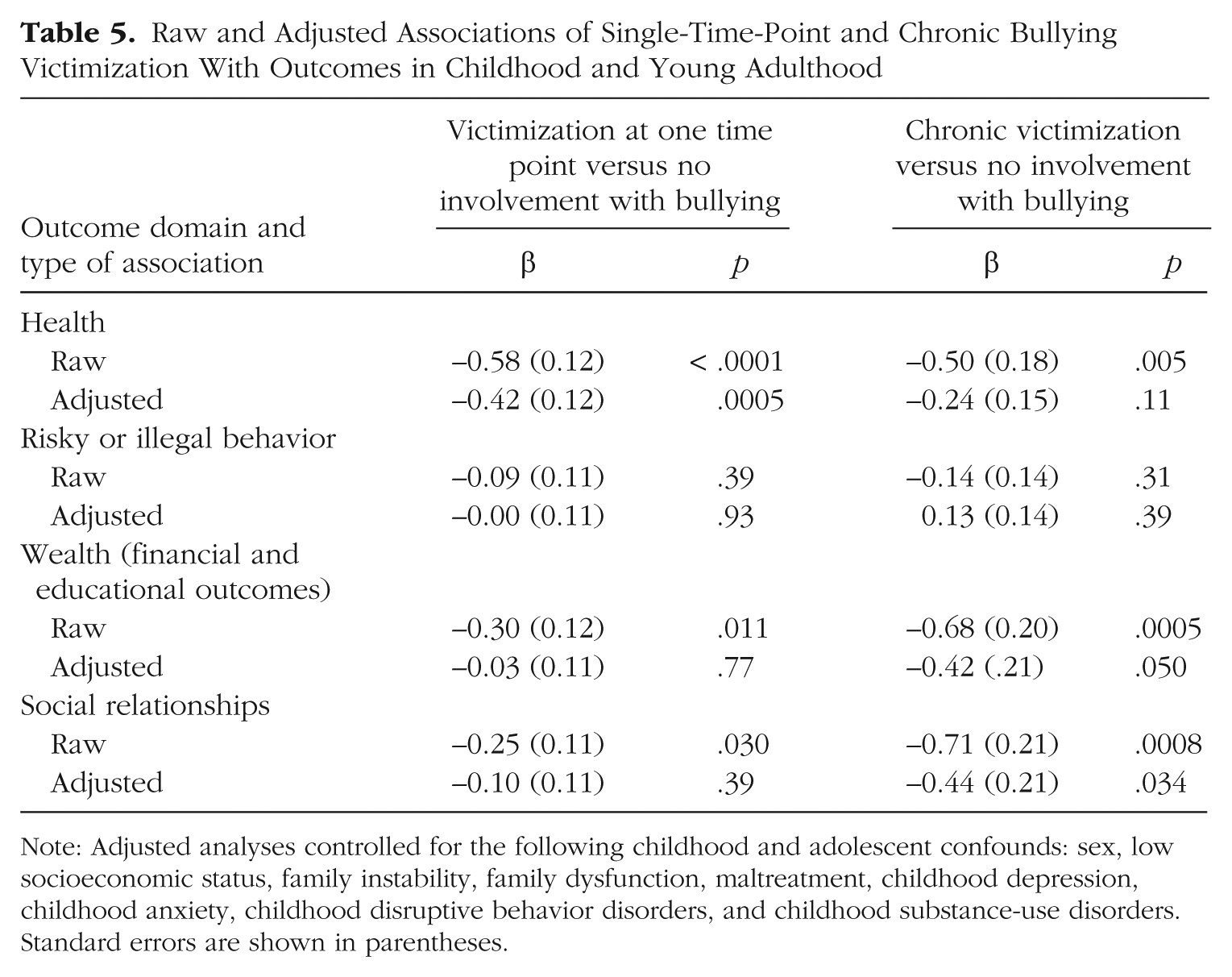
Note: Adjusted analyses controlled for the following childhood and adolescent confounds: sex, low socioeconomic status, family instability, family dysfunction, maltreatment, childhood depression, childhood anxiety, childhood disruptive behavior disorders, and childhood substance-use disorders. Standard errors are shown in parentheses.
Results
Bullying role in childhood and specific aspects of health and risky behavior in adulthood
Table 2 displays the unadjusted associations between childhood role-in-bullying status and adult health outcomes and risky or illegal behaviors. Each association was tested with weighted logistic regression models, and associations are reported as odds ratios with 95% confidence intervals and associated p values for all subjects involved in bullying compared with subjects in the not-involved-in-bullying group. Bully-victims in school had the worst health outcomes in adulthood (increased rates of poor outcomes on six of nine indices), with markedly increased likelihood of having been diagnosed with a serious illness, having been diagnosed with a psychiatric disorder, regular smoking, and slow recovery from illness. Bullies and victims were both elevated on two of nine indices: psychiatric problems and regular smoking. Risky or illegal behaviors were more commonly engaged in by bullies (six of nine indices) and bully-victims (two of nine indices). Bullies had elevated rates for a range of behaviors, including felonies, substance use, and self-reported illegal behavior. There was no evidence of elevated risk for risky or illegal behavior among victims.
Bullying role in childhood and specific aspects of wealth and social relationships in adulthood
Unadjusted associations were also tested for wealth (financial-educational outcomes) and social outcomes (Table 3). The area with the most evidence of impairment across all groups was financial-educational functioning. Bullies had elevated rates of four of seven outcomes, bully-victims of six outcomes, and victims of three outcomes. All groups were at risk for being impoverished in young adulthood and having difficulty keeping jobs. Both bullies and bully-victims displayed impaired educational attainment. There were no significant differences across groups in the likelihood of being married, having children, or being divorced, but social relationships were disrupted for all subjects who had bullied or been bullied.
Overall effect of bullying role on health, risky behavior, wealth, and social relationships in adulthood
Figure 2 displays unadjusted z scores for each of the four outcome domains for all groups. Bully-victims were at elevated risk for negative outcomes across all domains, and both bullies and victims were at elevated risk across three of the four domains. Specifically, both victims and bully-victims showed poorer health (victims: β = −0.45, SE = 0.11, p < .001; bully-victims: β = −1.22, SE = 0.28, p < .001), but bullies did not (β = −0.21, SE = 0.14, p = .11). For risky or illegal behaviors, bullies and bully-victims had more negative outcomes (bullies: β = −0.82, SE = 0.25, p < .001; bully-victims: β = −0.44, SE = 0.19, p = .02), but victims did not (β = −0.13, SE = 0.10, p = .16). All three groups involved in bullying had poorer financial-educational outcome (bullies: β = −0.71, SE = 0.24, p = .002; victims: β = −0.37, SE = 0.11, p < .001; bully-victims: β = −1.00, SE = 0.18, p < .001). For social functioning, all three groups involved in bullying displayed more negative problem scores (bullies: β = −0.62, SE = 0.24, p = .009; victims: β = −0.27, SE = 0.11, p = 0.01; bully-victims: β = −0.91, SE = 0.31, p = .003).
Bullying role in childhood and adult outcomes adjusted for childhood psychiatric problems and family hardship
These associations, however, might be accounted for by family hardships and psychiatric problems in childhood, both of which influenced or were concurrent with risk for bullying or victimization. All significant associations were retested accounting for childhood family hardships (family SES, family stability, family dysfunction, and maltreatment) and child psychiatric problems (childhood depression; childhood anxiety; childhood disruptive behavior disorders; childhood substance-use disorders). Bullies’ risk for all adult outcomes was no longer elevated after we adjusted for confounds. In contrast, status as a victim or a bully-victim continued to be associated with poor outcomes in adulthood (see Table 4). Being a victim or, in particular, a bully-victim continued to be an independent predictor of diminished health, wealth, and social relationships in adulthood. For example, although the unadjusted prediction of poor health by bully-victim role versus not-involved-in-bullying status was β = -1.22 (SE = 0.28, p < .001), it became attenuated but remained significant after adjustment (β = -0.65, SE = 0.28, p < .05; Table 4) with male sex, low SES, and childhood depression explaining the difference. Bullying involvement did not predict risky or illegal behavior in adjusted models.
Chronicity of peer victimization and adult outcomes
Of the 421 victims and bully-victims, 159 (37.8%) were chronically bullied. Table 5 compares those who were victims at one time point only or at two or more time points (chronic victims) with those who were neither perpetrators nor victims of bullying with regard to all outcome domains. The findings are consistent with a dose-response pattern of effects of being bullied on wealth and social relations in adulthood. After adjustments for confounds, the likelihood of subjects who were chronically bullied having financial-educational and social-relationship problems remained elevated. Direct comparisons of chronically bullied victims and victims bullied at only one time point (not shown) revealed that the chronically bullied subjects had significantly higher levels of social problems (p = .046) and showed a trend toward greater financial problems (p = .083). There was no evidence of differences between groups in risky or illegal behavior or health outcomes.
Discussion
Involvement with bullying in any role was predictive of negative health, financial, behavioral, and social outcomes in adulthood. Once we adjusted for family hardship and childhood psychiatric disorders, risk of impaired health, wealth, and social relationships in adulthood continued to be elevated in victims and bully-victims. The greatest impairment across multiple areas of adult functioning was found for bully-victims. In contrast, pure bullies were not at increased risk of poor outcomes in adulthood once other family and childhood risk factors were taken into account. Finally, there was evidence to support a dose-response effect of being bullied for poor wealth and social outcomes.
Previous longitudinal research has suggested that victimization or perpetration of bullying in childhood may be a marker of present and later psychopathology rather than a cause of long-term adverse outcomes (Sourander et al., 2009). Other short-term longitudinal studies have suggested that the effects of victimization are unique and occur over and above any preexisting behavior or emotional problems (Kim, Leventhal, Koh, Hubbard, & Boyce, 2006) or genetic liability (Arseneault et al., 2008). Previous cross-sectional studies and short-term longitudinal studies of children (Arseneault et al., 2010; Zwierzynska, Wolke, & Lereya, 2013) or retrospective studies of adults (Lund et al., 2009) have indicated the presence of increased physical, psychosomatic, and mental health problems in victimized children and, in particular, those who were bully-victims.
It has been suggested that some children may bully others as a response to being bullied, rather than becoming targets of other bullies after engaging in bullying (Arseneault et al., 2010). This move from victim to bully-victim may occur more often when victims are from deprived families, show poor emotional regulation, or have mental health problems and lack the resources to deal with the stress. Indeed, victims have been described as withdrawn, unassertive, easily emotionally upset, and lacking emotional or social understanding (Camodeca, Goossens, Schuengel, & Terwogt, 2003; Woods et al., 2009), whereas bully-victims tend to be aggressive, easily angered, and frequently bullied by their siblings (Wolke & Skew, 2012). In the present study, victims and, in particular, bully-victims differed from children who were not involved in bullying by growing up more often in deprived families (Lereya et al., 2013) and having more mental health problems in childhood. By adjusting for these preexisting or concurrent problems, this study provides strong evidence of unique and direct effects, not only on health but on wealth (Brown & Taylor, 2008) and social functioning in adulthood, of exposure to peer victimization and, in particular, of being chronically victimized by peers or being a bully-victim (Lehti et al., 2012). Controlling for family and childhood psychiatric problems attenuated these relationships but did not eliminate them.
In contrast, risky or illegal behaviors ranging from felonies to illicit drug use or one-night stands with strangers were attenuated and no longer explained by involvement in bullying once family and child psychiatric factors were controlled for. Boys and subjects with childhood disruptive disorders (including conduct disorder, attention-deficit/hyperactivity disorder, and oppositional defiant disorder) and childhood substance-use disorder were more likely to engage in risky or illegal behaviors. Thus, risky or illegal behavior in adulthood was explained not by childhood bullying or victimization per se but by a persistent overall antisocial tendency (Odgers et al., 2008), for which involvement in bullying as perpetrator may have been an early indicator rather than a cause (Niemelä et al., 2011). Similarly, a recent meta-analysis found that the perpetration of bullying was related to later offending, but that the size of this effect decreased as more confounds were included in the analysis and follow-up periods increased (Ttofi et al., 2011).
There are a variety of potential routes by which being victimized may affect later outcomes. Being bullied may alter physiological responses to stress (Ouellet-Morin et al., 2011); interact with a genetic vulnerability, such as variation in the serotonin transporter gene (Sugden et al., 2010); affect telomere length or the epigenome (Shalev et al., 2012); change cognitive responses to threatening situations (Mezulis, Abramson, Hyde, & Hankin, 2004); or affect school performance. Altered hypothalamic-pituitary-adrenal–axis activity and altered cortisol responses may not only increase the risk for developing mental health problems (Harkness, Stewart, & Wynne-Edwards, 2011) but increase susceptibility to illness by interfering with immune responses (Segerstrom & Miller, 2004). Both altered stress responses and altered social cognition (e.g., hypervigilance to hostile cues; van Dam et al., 2012) and neurocircuitry (Teicher, Samson, Sheu, Polcari, & McGreenery, 2010) related to bullying exposure may affect social relationships with parents, friends, and coworkers. Finally, victimization, particularly that of bully-victims, has been found to be associated with poor concurrent academic achievement (Nakamoto & Schwartz, 2010). However, for victims, this association is usually weak. Indeed, we found no increased risk of failure to complete high school or college among single-time-point victims but increased overall financial and educational problems among chronic victims. Similarly, bully-victims were at higher risk for academic failure and poor job performance. This result is in contrast to findings from a previous report that, however, did not distinguish between victims and bully-victims but considered them together as victims (Brown & Taylor, 2008).
This study has the advantages of a prospective, longitudinal design within a representative community sample that used structured interviews to assess bullying involvement in childhood and outcomes in young adulthood. There are also limitations. This sample is not representative of the U.S. population, given that American Indians were overrepresented and African Americans were underrepresented. The prevalence rates of bullying and peer victimization reported by subjects of the present study in childhood are similar to rates reported in population-based studies (Analitis et al., 2009; Nansel et al., 2001). Bullying involvement was coded by aggregating across multiple observations. For the bully-victim group, this might have meant that subjects moved between the roles of victim and bully across time (Arseneault et al., 2010). It is not at all clear how different patterns of movement between perpetrating and being victimized by bullying might affect short- or long-term outcomes (van Dam et al., 2012). Family hardships and childhood psychiatric problems were assessed throughout childhood and adolescence and were accounted for in adjusted analyses. It is possible that psychiatric problems, in particular, might have been the consequence of involvement in bullying in some cases (Arseneault et al., 2008; Reijntjes et al., 2010) rather than a confound as in the analysis. This would suggest that our findings may underestimate the long-term effects of involvement in bullying. There is always the possibility of unmeasured confounding, such as potential genetic factors, in longitudinal research. Finally, despite our use of a large community sample, there were not sufficient numbers of subjects in some groups to allow us to test differences by race/ethnicity or sex.
Conclusion
Being bullied is not a harmless rite of passage or an inevitable part of growing up but throws a long shadow over affected children’s lives. Victims, in particular chronic victims and bully-victims, are at increased risk for adverse health, financial, and social outcomes in adulthood. These problems are associated with great costs for individuals and society. Involvement with bullying can be easily assessed and monitored by health professionals and school personnel, and effective interventions for reducing victimization are available (Ttofi & Farrington, 2011). Such interventions are likely to reduce human suffering and long-term health and social costs.
Footnotes
Acknowledgements
The authors would like to thank Saverio Stranges for comments on a draft of this manuscript.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
The work presented here was supported by the National Institute of Mental Health (Grants MH63970, MH63671, and MH48085), the National Institute on Drug Abuse (Grant DA/MH11301), the Brain & Behavior Research Foundation (Early Career Award to W. E. Copeland), the William T. Grant Foundation, and the U.K. Economic and Social Research Council (Grant ES/K003593/1).