
Abstract
Early life stressors are associated with elevated inflammation, a key physiological risk factor for disease. However, the mechanisms by which early stress leads to inflammation remain largely unknown. Using a longitudinal data set, we examined smoking, alcohol consumption, and body mass index (BMI) as health-behavior pathways by which early adversity might lead to inflammation during young adulthood. Contemporaneously measured early adversity predicted increased BMI and smoking but not alcohol consumption, and these effects were partially accounted for by chronic stress in young adulthood. Higher BMI in turn predicted higher levels of soluble tumor necrosis factor receptor type II (sTNF-RII) and C-reactive protein (CRP), and smoking predicted elevated sTNF-RII. These findings establish that early adversity contributes to inflammation in part through ongoing stress and maladaptive health behavior. Given that maladaptive health behaviors portend inflammation in young adulthood, they serve as promising targets for interventions designed to prevent the negative consequences of early adversity.
Stressful early experiences have been linked to elevated inflammation later in life (e.g., Danese, Pariante, Caspi, Taylor, & Poulton, 2007). Although an acute inflammatory response is necessary for fighting infection and healing wounds, chronic inflammation is implicated in the development and progression of a number of serious diseases (e.g., Koenig et al., 1999). Thus, chronic inflammation is hypothesized to be a key physiological process by which early stress influences physical health (Miller, Chen, & Parker, 2011). However, the mechanisms by which early stressors lead to later inflammation are largely unknown.
A number of processes, mostly neurobiological in nature, have been hypothesized to contribute to the long-term effects of early adversity on inflammation (Miller et al., 2011). However, the role of health behaviors as potential mediators of this relationship has received less attention. Certain early adversities, such as poverty and maltreatment, have been linked to later smoking, alcohol consumption, and elevated body mass index (BMI; Goldstein, Flett, & Wekerle, 2010; Midei & Matthews, 2011; Najman, Toloo, & Siskind, 2006). Cross-sectional studies have linked these health behaviors, in turn, to elevations in systemic inflammation (Ambrose & Barua, 2004; Festa et al., 2001; Imhof et al., 2004).
Previous research on early adversity-inflammation associations has tended to control for the effects of health behaviors, rather than directly examining them as mechanisms of these associations (e.g., Danese et al., 2007; Kiecolt-Glaser et al., 2011); yet several recent studies provide evidence that specific early adversities, such as low socioeconomic status (Brummett et al., 2013; Hagger-Johnson, Mõttus, Craig, Starr, & Deary, 2012) and abuse (Matthews, Chang, Thurston, & Bromberger, 2014), affect the inflammatory marker C-reactive protein (CRP) indirectly through unhealthy behaviors and increased BMI. The current study therefore tested whether maladaptive health behaviors serve as mechanisms of the effects of cumulative early adversity on inflammation in a large community sample of young adults. Moreover, because early adversity has been linked to continued stress throughout development (Hazel, Hammen, Brennan, & Najman, 2008), we tested whether early adversity influences health behaviors through more proximal life stress. Our prospective design expanded on prior studies by allowing contemporaneous, rather than retrospective, assessment of a broad range of early life adversities. We hypothesized that early adversity would predict increased smoking, BMI, and alcohol consumption in young adulthood, in part through ongoing chronic stress in young adulthood, and that negative health behaviors would, in turn, predict elevated inflammation.
Method
Participants
Although most research on early stress and inflammation has been conducted with adults, the current analyses used a sample of young adults, given recent evidence that childhood adversity could influence markers of inflammation as early as adolescence (Slopen, Koenen, & Kubzansky, 2012). Participants were drawn from more than 7,000 children included in the Mater-University of Queensland Study of Pregnancy (MUSP; Keeping et al., 1989), a longitudinal birth-cohort study of children’s development. From this birth cohort, 815 mother-child pairs were originally selected when the children were 15 years of age for a follow-up study of children at risk for depressive and other disorders. Pairs were selected on the basis of mothers’ reports of depressive symptoms from pregnancy through 5 years after the child’s birth. These families were selected to represent a range of symptom presence, chronicity, and severity of maternal depression (see Hammen & Brennan, 2001, for details). The adolescent sample at age 15 was 50.6% male and 49.4% female. Families were largely lower and lower-middle income and predominantly Caucasian (91.4%; 3.6% were Asian, and 5% responded “other” or did not report ethnicity).
These 815 youths were contacted for additional follow-ups at the ages of 20 and 21 years, during which time they completed questionnaires about depressive symptoms and health behavior, as well as interviews about recent stressful experiences. At one final time point between the ages of 22 and 25, participants were recruited to contribute blood samples, which resulted in a reduced sample of 444 youths who completed all follow-ups and provided blood samples. Some participants were excluded from analyses because of extreme values for certain study measures, as detailed in the Measures section. This left a final sample of 389 (57% female, 43% male) participants for the current study. These participants did not differ from the rest of the original sample of 815 youths in terms of maternal depression history, χ2(1, N = 681) = 0.98, p = .32, family income, t(782) = 0.89, p = .38, cigarette smoking, t(573) = 0.77, p = .44, depressive symptoms, t(693) = 0.78, p = .44, or alcohol consumption rates, t(575) = −1.82, p = .07. However, participants included in the final sample had slightly lower BMI scores, t(427) = 2.42, p < .05, and were more likely to be female, χ2(1, N = 815) = 15.04, p < .001, compared with participants in the original sample.
Procedure
Mothers completed measures about the child’s early rearing environment at four time points during the first 5 years of the child’s life: at their first prenatal visit (typically in the first trimester of pregnancy), 3 to 4 days after the child’s birth, 6 months after birth, and 5 years after birth. Youths completed questionnaires about health behaviors and depressive symptoms at 20 and 21 years of age, completed interviews about experiences with stress at age 20, and provided blood samples at one time point between the ages of 22 and 25. Participants all gave informed consent, and the institutional review boards and ethics panels of the University of Queensland, Emory University, and the University of California, Los Angeles (UCLA), approved the research protocol.
Measures
Early adversity
Early adversity was assessed using mothers’ reports on five indicators of adversity measured in the first 5 years of the child’s life. These specific indicators were selected based on a review of studies that have examined links between cumulative indices of early adversity and various physical- and emotional-health outcomes (e.g., Felitti et al., 1998; Kiecolt-Glaser et al., 2011). Maternal psychopathology was coded as present if mothers reported any Axis I diagnosis (excluding specific phobia) between the child’s birth and the age-5 assessment on the Structured Clinical Interview for DSM-IV for lifetime disorders (First, Spitzer, Gibbon, & Williams, 1995), which was administered to mothers when children were 15 years old. The most common diagnoses were major depressive disorder (n = 78), dysthymic disorder (n = 68), and social phobia (n = 34).
Parental discord was coded as present if mothers consistently endorsed high levels of quarreling across the early childhood assessments. Harsh discipline was coded as present if mothers consistently reported at the age-5 assessment that they would hit or smack their child as a method of discipline. Family income was measured using the average maternal rating of the family’s annual income on a 7-point scale completed at three of the early childhood assessments: pregnancy, 6 months after the child’s birth, and 5 years after the child’s birth. Individuals falling within the lowest third of family income were coded as having this early adversity. Finally, parental criminal behavior was scored as present or absent based on mothers’ reports about whether they or their partner had been arrested or spent time in prison at any point during the first 5 years of their child’s life.
An early-adversity composite was created, given that risk for poor mental and physical health has been shown to rise with increasing numbers of early adversities (e.g., Felitti et al., 1998). In the present study, a count of the number of early adversities present for each child was used. Because few participants had all five adversities, participants with four or more adversities were combined to create a composite with a more normal distribution (range = 0–4).
Body mass index (BMI)
BMI was calculated from youth self-reports of height and weight at the blood draw between the ages of 22 and 25 years. If these data were not reported at the blood draw, the youth’s height and weight at the age-21 assessment were used to calculate BMI. One participant was excluded from the current analyses because of an extreme BMI value (59.9), which was more than 6 standard deviations above the mean for males in this sample.
Smoking
Youths completed a self-report measure of the number of cigarettes smoked per day at the age-21 assessment (1 = did not smoke, 2 = 1–9 cigarettes per day, 3 = 10–19 cigarettes per day, 4 = 20–29 cigarettes per day, 5 = 30–49 cigarettes per day, 6 = 50+ cigarettes per day). Because few participants endorsed the highest smoking category, participants who reported smoking 30 or more cigarettes per day were combined to create a measure with a more normal distribution (range = 1–5).
Alcohol consumption
At age 21, youths reported how many alcoholic beverages they typically consumed per day on a scale ranging from 1 (0 drinks per day) to 5 (3.5 or more drinks per day).
Depressive symptoms
Youths’ depressive symptoms at age 20 were assessed using the second edition of the Beck Depression Inventory (BDI-II; Beck, Steer, & Brown, 1996), a well-validated self-report questionnaire. The coefficient alpha in the current sample was .93.
Young adulthood chronic stress
At the age 20 assessment, target youth experiences with chronic stress in the prior 6 months were measured using the UCLA Life Stress Interview, a semistructured interview that probes stressful ongoing conditions across a number of life domains (Hammen & Brennan, 2001). The interview contains queries about several developmentally appropriate domains: social life, close friendship, romantic relationships, family relationships, financial difficulties, work problems, academic problems, and health problems of close family. For each domain, trained advanced graduate students used standard probes and semistructured follow-up queries to make an objective rating of chronic stress on a 5-point scale (1 = superior/exceptional functioning, 5 = severe difficulties), using behaviorally anchored descriptors. Total chronic stress levels were computed by summing across all domains. Evidence of the convergent and predictive validity of the UCLA Life Stress Interview in the current sample is reported in Hammen, Brennan, and Keenan-Miller (2008). In the current sample, the mean intraclass correlation across all domains at age 20 was r = .81.
Inflammatory markers
Plasma levels of two inflammatory markers, CRP and soluble tumor necrosis factor receptor type II (sTNF-RII), were assessed between the ages of 22 and 25 years. CRP is an acute-phase protein produced by the liver in response to the proinflammatory cytokine interleukin 6 (IL-6) and serves as a reliable marker of chronic inflammation. The soluble receptor sTNF-RII is shed from a cell surface after stimulation of the cell by the proinflammatory cytokine tumor necrosis factor (TNF)-alpha and serves as a marker of TNF activity.
Blood samples were collected in ethylenediaminetetraacetic acid (EDTA) plasma and stored at −80° C for subsequent batch testing. Plasma levels of sTNF-RII were determined using an enzyme-linked immunosorbent assay (ELISA; R&D Systems, Minneapolis, MN) according to the manufacturer’s protocols, with a lower limit of detection of 234 pg/ml. CRP levels were determined using a high-sensitivity ELISA (Immundiagnostik, ALPCO Immunoassays, Salem, NH) according to the manufacturer’s protocol, but with an extended standard curve to a lower limit of detection of 0.2 mg/L. All samples were run in duplicate. To address nonnormality, we log-transformed CRP values for all analyses. Participants were excluded from the current study if they had CRP values greater than 10 or sTNF-RII values greater than 400 (n = 54), because such levels may be indicative of an acute inflammatory response rather than chronic inflammation (Pearson et al., 2003).
Data analysis
Structural equation modeling was used to examine direct and indirect paths among variables because of its ability to test complex mediational models. The hypothesized model examined the effects of early adversity on the two inflammatory markers through health behaviors (see Fig. 1). Because rates of depression in females are increased across adolescence and adulthood, we controlled for gender in all paths of this model (Hankin et al., 1998). We also ran the model including depressive symptoms as another mechanism of the effects of early adversity on later inflammation to control for the effects of depression, given the close links between depression and early life stress (Hammen, 2005), negative health behaviors (e.g., Allgöwer, Wardle, & Steptoe, 2001), and inflammation (Kiecolt-Glaser & Glaser, 2002). Finally, we examined a second model, in which early adversity contributed to health behaviors indirectly via more proximal chronic stress at age 20 (Fig. 2).

Path model examining cigarette use and body mass index (BMI) as pathways from early adversity to levels of C-reactive protein (CRP) and soluble tumor necrosis factor receptor type II (sTNF-RII) in young adulthood. Standardized regression coefficients are shown. Asterisks indicate statistically significant paths (†p < .10, *p < .05, **p ≤ .01).

Path model examining the role of chronic stress in the effects of early adversity on cigarette use, body mass index (BMI), and levels of C-reactive protein (CRP) and soluble tumor necrosis factor receptor type II (sTNF-RII) in young adulthood. Standardized regression coefficients are shown. Asterisks indicate statistically significant paths (†p < .10, **p < .01).
All analyses were carried out in Mplus (Version 5; Muthén & Muthén, 2007) using full-information maximum-likelihood methods to accommodate missing data. Because of univariate and multivariate nonnormality of the data, robust maximum-likelihood procedures were used to estimate standard errors. Overall model fit was evaluated using several standard fit indices: the likelihood-ratio chi-square test, the comparative fit index (CFI; Bentler, 1990), the root-mean-square error of approximation (RMSEA; Browne & Cudeck, 1993), and the standardized root mean-square residual (SRMR; Hu & Bentler, 1998).
Results
Descriptive statistics for all main study variables, as well as Pearson correlations between these variables, are presented in Table 1. Alcohol consumption at age 21 years was not significantly correlated with experiences of early adversity by age 5 years or the two inflammatory markers. As a result, only smoking behavior and BMI were included in subsequent analyses testing health behaviors as pathways from early adversity to inflammation.
Descriptive Statistics and Pearson Correlations Among Early Adversity, Health Behaviors, Depressive Symptoms, Chronic Stress, and Inflammatory Markers
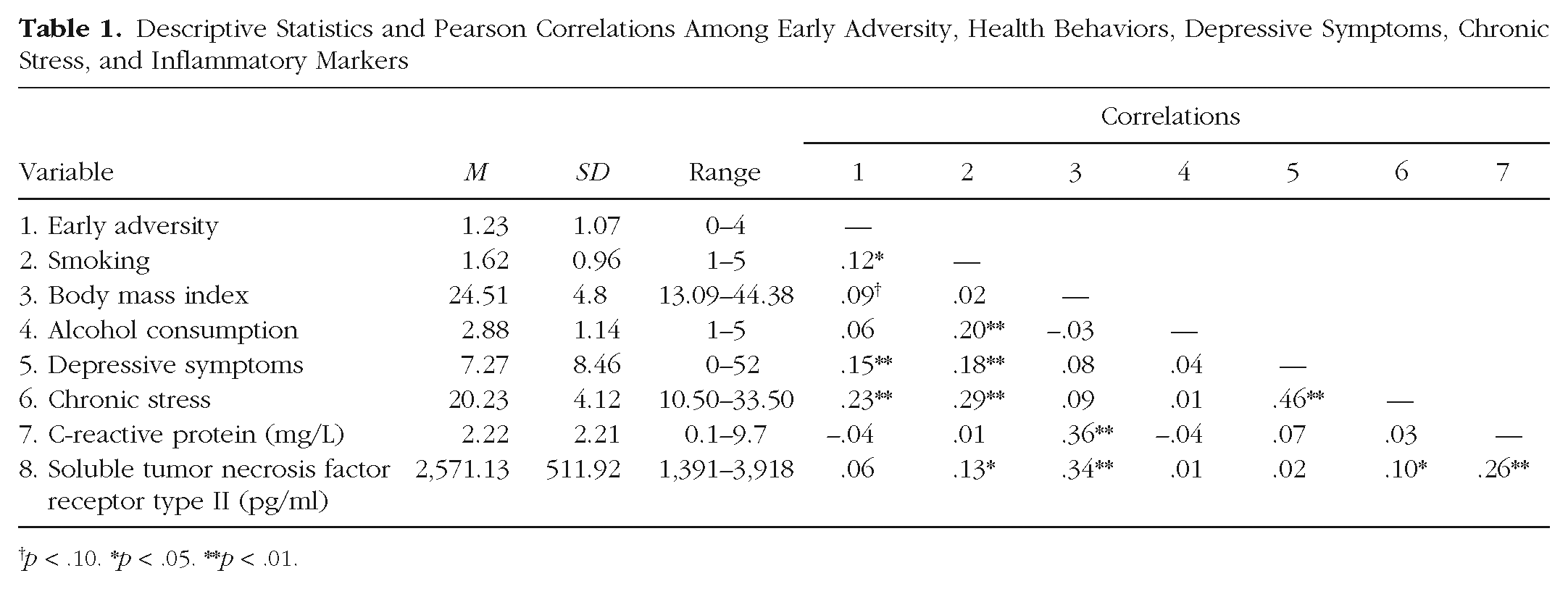
p < .10. *p < .05. **p < .01.
Path model analyses were used to test the indirect effects of early adversity by the age of 5 years on CRP and sTNF-RII levels at age 25, through smoking behavior and BMI at age 21. Standardized coefficients for all direct paths are displayed in Figure 1. This model provided an overall good fit to the data, χ2(3, N = 389) = 3.25, p = .36, CFI = .99, RMSEA = .02 (90% confidence interval, or CI = [.00, .09]), SRMR = .02. Cumulative experiences of early adversity by age 5 predicted elevated cigarette smoking, and were marginally significant in predicting elevated BMI, in young adulthood. Higher BMI, in turn, predicted higher levels of CRP and sTNF-RII, and more cigarette smoking predicted higher levels of sTNF-RII but not CRP. Early adverse experiences had significant indirect effects on each of the inflammatory markers through the proposed health behaviors (sTNF-RII: β = 0.05, p < .05; CRP: β = 0.04, p < .05). 1
When youths’ depressive symptoms at age 20 were included as a third path from early adversity to the inflammatory markers, the model showed similar fit, χ2(5, N = 389) = 15.02, p = .01, CFI = .94, RMSEA = .07 (90% CI = [.03, .12]), SRMR = .04, and identical patterns of significance. Early adversity strongly predicted depressive symptoms at age 20, in addition to cigarette use and BMI. However, depressive symptoms did not have a relationship with inflammatory markers in young adulthood over and above the effects of smoking and BMI.
Finally, when early adversity and chronic stress in the 6 months prior to age 20 were both included as predictors of BMI and smoking behavior, recent stress was more strongly predictive of the health behaviors. The best-fitting model (see Fig. 2) indicated that early adversity led to higher rates of recent stress, which in turn predicted BMI and smoking behavior, χ2(5, N = 389) = 7.55, p = .37, CFI = .99, RMSEA = .01 (90% CI = [.00, .07]), SRMR = .02. All other paths in the model showed identical patterns of significance to those in the original model.
Discussion
The current study tested the role of maladaptive health behaviors in the link between early adversity and disrupted inflammatory processes. Results indicated that early adversity predicted elevated cigarette use and BMI, but not alcohol consumption, in young adulthood. Further exploration suggested that these effects of early adversity on health behavior were partially accounted for by the relationship between early adversity and chronic stress in young adulthood. Higher BMI, in turn, predicted higher levels of sTNF-RII and CRP, and cigarette smoking predicted higher levels of sTNF-RII. Although early adverse experiences were a strong predictor of later depressive symptoms, depressive symptoms had negligible effects on inflammatory markers over and above the effects of health behaviors.
Past research on the effects of early adversity on inflammation has tended to control for health behaviors as confounds and only recently has begun to examine the role of maladaptive health behaviors in these effects. Moreover, few studies have used longitudinal designs to account for the continuity of stress and depressive symptoms in maladaptive health outcomes related to early adversity. Our results highlight negative health behaviors, particularly smoking and high BMI, as important pathways by which continuing life stress “gets under the skin” to contribute to long-term risk for physical illness. These findings are an important complement to studies examining the biological and cognitive impact of early adversity, because they identify potentially modifiable health-related behaviors that predict inflammation during critical developmental periods such as adolescence and early adulthood.
Contrary to predictions, these results showed that early adversity was not associated with alcohol consumption. This may be because we were not predicting clinical levels of alcohol use and did not directly assess maltreatment, in contrast to most previous research. It is also noteworthy that, in contrast to some previous studies (e.g., Danese et al., 2007), our data revealed no direct association between early adversity and inflammatory markers. It is possible that the cascade of biological effects that follows exposure to adversity might not yet have had time to result in chronic inflammation because of the relatively young age of our sample. Consistent with this hypothesis, results from several previous studies have shown effects of early adversity on stimulated cytokine production but not on chronic inflammation (e.g., Miller et al., 2009).
Several limitations of the current study should be acknowledged. First, our measure of early adversity did not include some stressors that have been linked to later health (e.g., abuse). In addition, we examined an index of cumulative early risk, but future research would benefit from examining specific early adversities or clusters of adversity. Second, BMI is a marker of several health behaviors, including diet and exercise. Future research is therefore needed to investigate the specific health behaviors that account for the relationship between BMI and inflammation. Finally, although our final sample did not differ from the original sample on a number of variables, participants with higher BMI and males were more likely than participants with lower BMI and females to drop out before the final assessment.
Despite these limitations, these results address important questions about the psychological and biological mechanisms by which early adversity confers risk for poor physical health. Our findings highlight negative health behaviors as a potentially modifiable pathway by which early adversity leads to inflammation. Research in this area has important implications for understanding the psychobiological processes that mediate the long-term pathogenic effects of early life stress and could inform the development of clinical interventions to offset the physical-health consequences of these stressors.
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This work was supported by the National Health and Medical Research Council; Mater Misericordiae Mother’s Hospital; National Institute of Mental Health (NIMH) Grant R01 MH52239; NIMH Training Grant MH15750; the University of California, Los Angeles (UCLA), Norman Cousins Center for Psychoneuroimmunology; the UCLA Older Americans Independence Center; and National Institute on Aging Grant P30-AG028748.