
Abstract
People with attention-deficit/hyperactivity disorder (ADHD) have difficulties sustaining their attention on external tasks. Such attentional lapses have often been characterized as the simple opposite of external sustained attention, but the different types of attentional lapses, and the subjective experiences to which they correspond, remain unspecified. In this study, we showed that unmedicated children (ages 6–12) with ADHD, when probed during a standard go/no-go task, reported more mind blanking (a mental state characterized by the absence of reportable content) than did control participants. This increase in mind blanking happened at the expense of both focused and wandering thoughts. We also found that methylphenidate reverted the level of mind blanking to baseline (i.e., the level of mind blanking reported by control children without ADHD). However, this restoration led to mind wandering more than to focused attention. In a second experiment, we extended these findings to adults who had subclinical ADHD. These results suggest that executive functions impaired in ADHD are required not only to sustain external attention but also to maintain an internal train of thought.
Keywords
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by inattention, impulsivity, and hyperactivity (American Psychiatric Association, 2013; Barkley, 1997, 2014). Some researchers have suggested that inattention and poorer task performance in ADHD correspond to episodes of mind wandering (Franklin et al., 2014; Seli, Smallwood, Cheyne, & Smilek, 2015; Shaw & Giambra, 1993). Indeed, mind wandering is associated with behaviors present in ADHD, such as impulsivity (Cheyne, Solman, Carriere, & Smilek, 2009), poor sustained attention leading to lower academic performance (Randall, Oswald, & Beier, 2014; Seli, Cheyne, & Smilek, 2013), hyperactive behaviors (Seli et al., 2013), elevated response variability (Bastian & Sackur, 2013; Seli et al., 2013), and failures of executive control (Kane & McVay, 2012). However, recent studies have demonstrated that mind wandering is positively correlated with patience (Smallwood, Ruby, & Singer, 2013), controlled processing (Gorgolewski et al., 2014), and premeditation (Smallwood, Nind, & O’Connor, 2009), all of which are absent in people with ADHD. Moreover, episodes of mind wandering hamper processing of external stimuli, a phenomenon referred to as perceptual decoupling (Barron, Riby, Greer, & Smallwood, 2011; Smallwood, Beach, Schooler, & Handy, 2008), whereas ADHD is associated with greater environmental distraction (Barkley, 1997). Thus, it remains unclear whether inattention to focal tasks in ADHD corresponds to mind wandering. Most past researchers have characterized external sustained attention and mind wandering as simple opposites, but we devised a richer classification of mental states to elaborate on this simple opposition and shed light on this controversy. Thus equipped, we directly probe the types of attentional lapses, as subjectively experienced, in a population of children with ADHD and young healthy adults.
Mind wandering is more than inattention to focal tasks (Smallwood & Schooler, 2006): It designates spontaneous self-generated thoughts that are independent of both the task and the environment (Christoff, Irving, Fox, Spreng, & Andrews-Hanna, 2016; Smallwood, 2013; Smallwood & Schooler, 2006). In the current study, we will use this precise definition: Mind wandering has rich content (as opposed to blank thoughts; Ward & Wegener, 2013), is independent from the environment (as opposed to being a distraction), and is unrelated to the task at hand (as opposed to being task-related interferences). In keeping with these notions, it has been suggested (Smallwood, 2013) that mind wandering could share some cognitive mechanisms with task focus because executive resources could be necessary to sustain an internal train of thought (mind wandering), just as they are necessary for external thoughts (on-task focus). Therefore, a deficit in executive functions, as found in ADHD (Barkley, 1997), should entail deficits in both mind wandering and sustained attention on focal tasks.
To test this hypothesis, we engaged children and young adults in a thought-sampling experiment (Hurlburt & Heavey, 2001) during the Sustained Attention to Response Task (SART; Robertson, Manly, Andrade, Baddeley, & Yiend, 1997). In our version of the SART, randomly distributed thought probes required participants to classify their thoughts into five categories on the basis of their content—(a) on-task focus, in which attention was focused on the task; (b) mind wandering, which refers to spontaneous thoughts unrelated to the task or stimulus; (c) distraction, which involves environment-dependent thoughts; (d) task-related interference, which refers to reflexive thoughts about the task but no focus on the task itself; and (e) mind blanking, which refers to no reportable mental content. These categories were derived by crossing the two dimensions of task relatedness (high task-relatedness: on-task focus and task-related interference; low task-relatedness: mind wandering and distraction) and stimulus dependency (high stimulus dependency: on-task focus and distraction; low stimulus dependency: mind wandering and task-related interference), whereas mind blanking was contentless. Note that mind blanking includes reports of blank thoughts and failures to report existing contents (i.e., failures of metacognition). The recent finding of a metacognitive deficit in ADHD (Antshel & Nastasi, 2008; Knouse, Bagwell, Barkley, & Murphy, 2005), and the well-known association between frontal executive and metacognitive deficits (Shimamura, 1994), concerning self-awareness in particular (Fuster, 1997), suggest that attentional lapses in ADHD may correspond to lower awareness of mental content and thus to episodes of mind blanking.
In a first experiment, we tested two groups of children with an ADHD diagnosis: one group that had never received psychotropic medication and a second group that was treated with methylphenidate, the standard treatment (i.e., the most efficient and prescribed treatment) for ADHD (Barkley, 2014). We compared them with two control groups: a clinical group composed of patients with other psychiatric disorders and a group of children with neurotypical development. In a second experiment, we used the Diagnostic Interview for ADHD in adults (Diagnostisch Interview Voor ADHD; Kooij & Francken, 2010), or DIVA, to test nonclinical young adults (i.e., those who have a high level of symptoms but whose lives are not affected enough to require treatment) and explore how ADHD symptoms relate to mind wandering and mind blanking in the nonclinical population because the disorder may be viewed as a continuum (Overbey, Snell, & Callis, 2011).
In sum, we aimed to characterize the subjective aspects of inattentive episodes in ADHD. We predicted that people who are hypothesized to have less executive control (e.g., children with ADHD and adults who score high on the DIVA questionnaire) should have decreases in sustained trains of thought (i.e., the on-task-focus and mind-wandering categories). In addition, given the metacognitive deficit, ADHD symptoms might lead to increased reports of mind blanking.
Study 1
Method
Participants
The children included in the study were 6 to 12 years old, had no comorbid neurological or genetic syndrome, and had intellectual ability scores of 70 or higher, as measured by the Verbal Comprehension Index (VCI) and Perceptual Reasoning Index (PRI) of the fourth edition of the Wechsler Intelligence Scale for Children (WISC-IV; Wechsler, 2003). Psychiatric comorbidities were assessed with the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS; Kaufman, Birmaher, Brent, Rao, & Ryan, 1996). Parents provided informed consent. This research was approved by the local ethics committee. We continued recruiting for each of the four groups until we achieved 20 matched participants per group.
For all the children, a psychiatrist verified or excluded the diagnosis of ADHD by clinical assessment. Two groups of children with ADHD were formed: One group contained children that had never received any methylphenidate (N-ADHD; n = 20, 4 girls; mean age = 8.9 years, SD = 2.07), and the other group contained children who had been taking an extended-release form of methylphenidate (0.5–1 mg/kg a day) for more than 1 month (treated ADHD, or T-ADHD; n = 20, 6 girls; mean age = 8.9 years, SD = 1.68). (For the comorbidities of the patients with ADHD, see Table S2 in the Supplemental Material available online.) Two control groups were formed: One group contained healthy children (H-control; n = 20, 8 girls; mean age = 8.5 years, SD = 1.47), recruited via announcements in the Department of Cognitive Sciences of the École Normale Supérieure (Paris, France), and the other group contained children with psychiatric conditions other than ADHD (clinical control participants, or C-control; n = 20, 4 girls; mean age = 9.8 years, SD = 2.0; see Table S1 in the Supplemental Material).
Three groups of patients (N-ADHD, T-ADHD, and C-control) were recruited from among inpatients and outpatients of the pediatric psychiatry unit of the Hôpital Robert-Debré (Paris, France). As expected, scores on the ADHD Rating Scale (ADHD-RS; DuPaul, Power, Anastopoulos, & Reid, 1998) completed by the caregivers were higher for the N-ADHD group (M = 35.2, SD = 8.86) and the T-ADHD group (M = 31.6, SD = 8.18) than for either the C-control group (M = 22.11, SD = 1.34), t(33.8) = 3.97, p < .05 and t(32.3) = 2.96, p < .05, or the H-control group (M = 11.6, SD = 5.98), t(33.3) = 9.87, p < .05 and t(34.8) = 8.82, p < .05.
Table 1 provides detailed demographic and clinical information for the four groups. The groups were matched in age, F(3, 76) = 2.09, p > .1; sex ratio, F(1, 3) = 2.76, p > .250; and IQ on the PRI, F(3, 60) = 0.49, p > .250. Although the four groups’ scores on the VCI were significantly different, F(3, 60) = 4.34, p < .05, the scores of the two ADHD groups did not differ significantly, t(27.6) = 1, p > .250, and the scores of the two non-ADHD groups did not differ significantly, t(25) = −0.64, p > .250. However, the VCI scores were lower in the ADHD groups than in the non-ADHD groups—N-ADHD versus C-control: t(23.8) = −1.44, p = .16; T-ADHD versus C-control: t(28.7) = −2.18, p < .05; N-ADHD versus H-control: t(28.2) = −2.5, p < .05; and T-ADHD versus H-control: t(29.7) = −3.15, p < .05.
Demographic and Clinical Information for Participants in Study 1
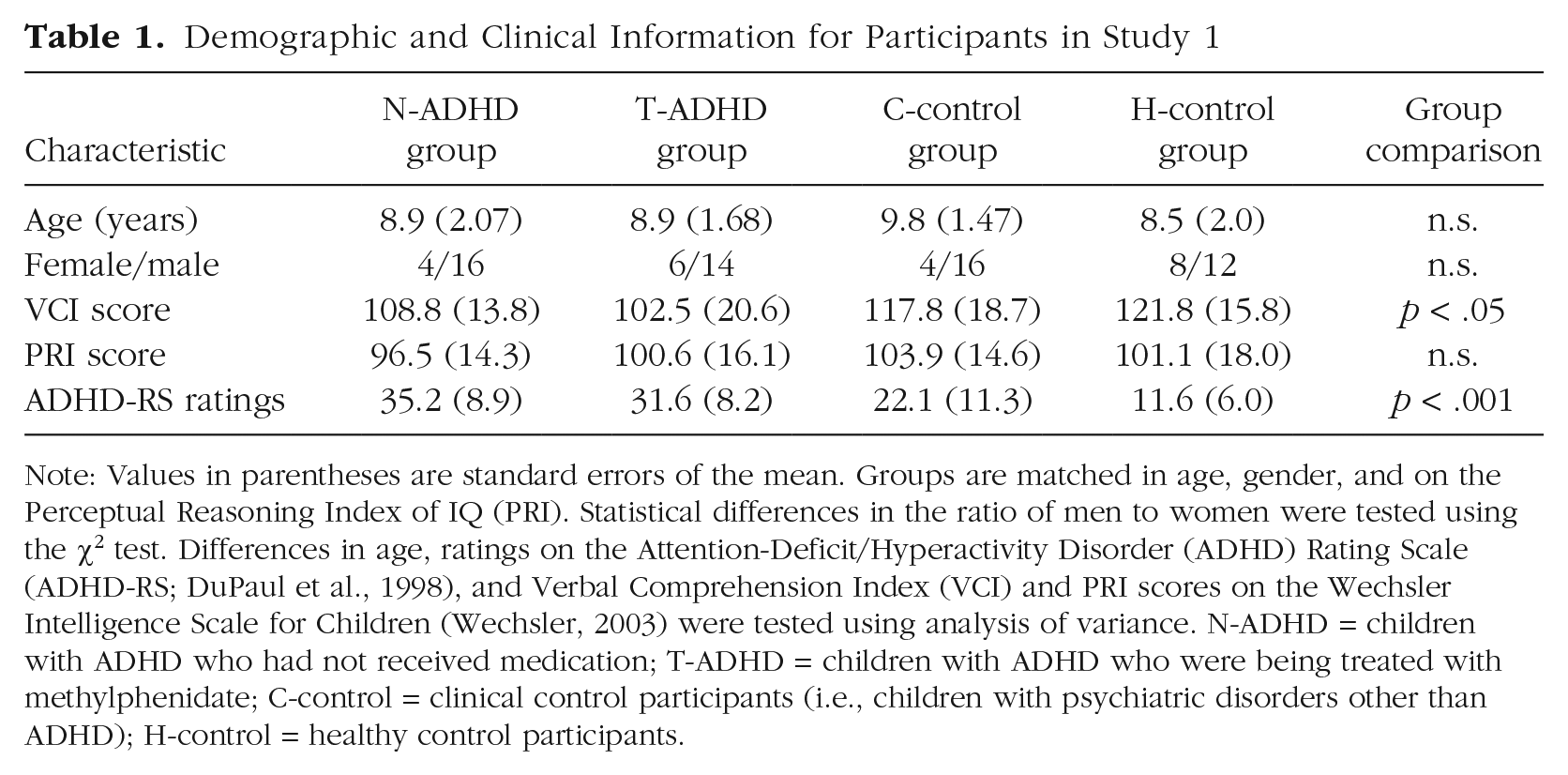
Note: Values in parentheses are standard errors of the mean. Groups are matched in age, gender, and on the Perceptual Reasoning Index of IQ (PRI). Statistical differences in the ratio of men to women were tested using the χ2 test. Differences in age, ratings on the Attention-Deficit/Hyperactivity Disorder (ADHD) Rating Scale (ADHD-RS; DuPaul et al., 1998), and Verbal Comprehension Index (VCI) and PRI scores on the Wechsler Intelligence Scale for Children (Wechsler, 2003) were tested using analysis of variance. N-ADHD = children with ADHD who had not received medication; T-ADHD = children with ADHD who were being treated with methylphenidate; C-control = clinical control participants (i.e., children with psychiatric disorders other than ADHD); H-control = healthy control participants.
Task
We used an adaptation of the SART (Robertson et al., 1997) that had embedded thought probes (Christoff, Gordon, Smallwood, Smith, & Schooler, 2009). The SART is a go/no-go task with very few (< 10%) no-go trials. A digit between 0 and 9 was presented on a computer screen for 500 ms, and the children were required to press the space bar for each digit, but to withhold their response when the digit was 3 (no-go target). We alternated between fast blocks (digits appeared every 1 s) and slow blocks (digits appeared every 2 s). There were 248 trials (go and no-go) in fast blocks and 124 trials in slow blocks.
Thought probes
Each block was randomly interrupted by eight thought probes: First, a screen with a question mark required the children to describe orally their thoughts at the moment of the interruption. A second screen asked them to classify their thoughts into one of five categories: on-task focus, task-related interference, distraction, mind wandering, and mind blanking. Categories were represented with line drawings of a teddy bear experiencing each type of mental content (see Appendix 1). Then, the children pointed at the drawing best representing their own mental state, and the experimenter finally validated the report by pressing the corresponding button. The experimenter was thus able to check for inconsistency between the children’s oral report and category choice. One child in the C-control group was excluded because of such an inconsistency.
Procedure
The instructions first presented the task and the categories of mental contents with the help of the drawings of a teddy bear (see Appendix 1). The explanations of the categories were as follows:
To perform the task, attention must be focused on the screen and on the correct response, to the exclusion of any other thought. However, staying focused all the time is impossible: Very often we start to think about something else and we are not in the task anymore. First, we might have some thoughts about our performance, meaning that we are not completely focused—this is thinking about the task; second, we might be distracted by a noise, or anything else in the surroundings—this is distraction; third, we might start thinking about something completely independent from the task and from the surroundings—this is mind wandering. Finally, it is also possible that we might not be focused on the task but we do not think about something in particular and our mind seems empty—this is mind blanking.
For each category, several examples were given while the experimenter pointed to the relevant drawing. Then, the experimenter asked the child to give an example of a situation he or she had already experienced to verify that each mental state was understood. Children then were presented with a training session of 55 go trials, 5 no-go trials, and three thought probes. The testing session comprised four blocks (two slow blocks and two fast blocks, alternating, with order counterbalanced across participants), for a total of 32 mental reports. The entire session lasted approximately 1 hr.
All assessments were conducted in a quiet area of the child and adolescent psychiatry department (Hôpital Robert-Debré, Paris, France). Children were tested in silence, in the presence of the experimenter. Experimenters’ comments were kept to a minimum during the task. The medicated children with ADHD were tested while the drug was active. The three clinical groups completed the clinical scales—IQ (PRI of WISC-IV; Wechsler, 2003) and ratings on the ADHD-RS (DuPaul et al., 1998)—and the experimental task on different days, but the healthy control participants did the scales and the task on the same day.
Results
We performed data analysis using the lme4 package (mixed modeling; Bates, Maechler, Bolker, & Walker, 2014) and the retimes package (fitting of exponentially modified Gaussian distributions of response times; Massidda, 2013) for the R software environment (Version 3.2.5; R Core Development Team, 2016). We performed mixed regression models with participants as a random factor and experimental conditions as fixed factors. Main effects of group (and their respective interactions) were assessed by model comparison—χ2 likelihood-ratio tests—between two logistic regressions, one full model with group or interaction as a fixed effect and one null model without this fixed effect. When group proved to be a significant factor, post hoc differences between groups were further detailed with the same method or by Wald tests with restricted contrasts. The α level was set at .05 for all analyses.
Performance on the SART
Accuracy was higher for go trials (95.8%, SD = 0.4) than for no-go trials (41.9%, SD = 1.6; see Table 2). A logistic regression on accuracy (48,779 observations of 80 participants), with factors of trial type (go, no-go), block pace (fast, slow), and group (N-ADHD, T-ADHD, C-control, H-control) confirmed the main effect of trial type, β = −3.93, SD = 0.14, z = −27.15, p < .001, yet revealed no main effect of group (p > .250) or block (p > .250), no interaction between group and trial type (p > .250), and no interaction between group and block (p > .250). In other words, performance in go and no-go trials was similar across groups, as was performance in fast and slow blocks.
Results From Study 1: Accuracy, Response Time, and Anticipations for Each Group Separately and for All Groups

Note: Values in parentheses are standard errors of the mean. N-ADHD = children with attention-deficit/hyperactivity disorder (ADHD) who had not received medication; T-ADHD = children with ADHD who were being treated with methylphenidate; C-control = clinical control participants (i.e., children with psychiatric disorders other than ADHD); H-control = healthy control participants.
Anticipations are trials with response times of less than 100 ms.
Yet a significant Block Pace × Trial Type interaction, χ2(1) = 66.8, β = −0.79, SD = 0.10, z = −8.13, p < .001 (see Fig. S1a in the Supplemental Material), provided evidence that block pace modulated performance across trial types: Slower pace increased task performance in go trials, β = 0.35, SD = 0.09, z = 3.93, p < .001, but decreased performance in no-go trials, β = −0.44, SD = 0.09, z = −5.05, p < .001. These effects imply that faster blocks may have been too challenging for children: A slower pace allowed them to press the response key more often, thereby increasing their performance for go trials while decreasing their performance on no-go trials.
In turn, the Block Pace × Trial Type interaction was qualified by an interaction with group (i.e., a Block Pace × Trial Type × Group interaction), χ2(3) = 11.91, p < .008. More precisely, whereas the T-ADHD, C-control, and H-control groups were similar to one another (all ps > .16), they differed from the N-ADHD group (all ps < .05), for whom there was no significant Block Pace × Trial Type modulation, β = −0.97, SD = 0.12, z = −8.48, p < .001 (computed across the T-ADHD, C-control and H-control groups), a modulation that was absent in the N-ADHD group (p > .1). Thus, despite similar overall performance, the N-ADHD group responded less often in go trials and committed fewer errors in no-go trials in slow blocks than in fast blocks.
Response times
There was no effect of group on response times in correct go trials, as assessed by analyses of variance on the mean, standard deviation, and coefficient of variation (SD/mean; all ps > .250; all interactions with block type, ps > .250). In addition, we tested the variability in response times in correct go trials using exponentially modified Gaussian distributions. There was no effect of group for any of the components of these distributions (all ps > .05). Finally, we used a Poisson regression for count data to test whether the number of anticipations (i.e., RTs < 100 ms; Cheyne et al., 2009) differed between groups, and we found no effect (p > .05).
Subjective reports
Overall, the children reported being on task in 49.6% (SD = 2.4) of the thought probes. The values for the other categories were as follows—task-related interference: 19.3%, SD = 1.5; mind blanking: 11.6%, SD = 1.3; distraction: 10.4%, SD = 1.1; and mind wandering: 9.1%, SD = 1.2. To statistically test the between-groups differences, we used mixed-effects logistic regressions predicting the likelihood of each of the five possible categories would be reported. Participant was a random factor, and group and block pace were fixed factors.
The N-ADHD group reported about twice as much mind blanking (19.2%, SD = 3.3) as the other three groups (Fig. 1a)—T-ADHD: 11.0%, SD = 2.3; β = −0.72, SD = 0.34, z = −2.11, p < .05; C-control: 8.1%, SD = 2.19; β = −0.99, SD = 0.35, z = −2.78, p < .01; H-control: 8.0%, SD = 1.56; β = −1.02, SD = 0.34, z = −2.96, p < .005. In contrast, the T-ADHD group reported more mind wandering (15.0%, SD = 3.4) than the other three groups did (Fig. 1b)—N-ADHD: 6.1%, SD = 1.5; β = −1.01, SD = 0.39, z = −2.60, p < .01; C-control: 7.0%, SD = 1.2; β = −0.84, SD = 0.39, z = −2.15, p < .05; H-control: 8.3%, SD = 2.28; β = −0.75, SD = 0.38, z = −1.97, p < .05. Beyond these differences, all the groups reported similar values for on-task focus, χ2(3) = 3.94, p > .250 (Fig. 1c); task-related interference, χ2(3) = 0.33, p > .9 (Fig. 1d); and distractions, χ2(3) = 2.13, p > .250 (Fig. 1e). Block pace had no significant effect on any of the responses to the thought probes (all ps > .250) and did not interact with group in any of the analyses (all ps > .2).

Results from Studies 1 and 2. The graphs on the left show the mean percentages of (a) mind blanking, (b) mind wandering, (c) on-task focus, (d) task-related interference, and (e) distraction. For Study 1, results are shown for the healthy control group (H-control), the clinical control group (C-control), children with attention-deficit/hyperactivity disorder (ADHD) who had not received medication (N-ADHD), and children with ADHD who had received medication (T-ADHD); for Study 2, results are shown for the ADHD group and the control group. The graphs on the right show the mean percentages of (f) mind wandering and on-task focus combined and (g) task-related interference and distraction combined for the same groups. Asterisks indicate significant pairwise differences between groups (*p < .05, **p < .01). Error bars represent ±1 SE.
To test the hypothesis that on-task and mind-wandering states constitute sustained trains of thought that require executive resources, we also tested whether the likelihood of reporting either on-task or mind-wandering states varied between groups. Indeed, the N-ADHD group reported significantly fewer instances of on-task focus and mind wandering (49.4%, SD = 4.1) than did the T-ADHD group (62.4%, SD = 3.0) or the H-control group (64.1%, SD = 4.4)—N-ADHD versus T-ADHD: β = 0.53, SD = 0.25, z = 2.08, p < .05; N-ADHD versus H-control: β = 0.67, SD = 0.25, z = 2.70, p < .01 (Fig. 1f). The difference between the N-ADHD group and the C-control group (59.1%, SD = 4.3) was not significant, p > .1.
By contrast, when we analyzed results from states that are not supposed to require executive resources (task-related interference and distraction), we found no difference between groups (N-ADHD: 31.4%, SD = 2.8; T-ADHD: 26.7%, SD = 3.2; C-control: 32.7%, SD = 4.3; H-control: 28%, SD = 3.7), χ2(3) = 1.81, p > .6 (Fig. 1g). This suggests that increased reports of mind blanking in the N-ADHD group might have occurred at the expense of on-task and mind-wandering episodes.
Discussion
We found that, in the absence of any strong between-groups difference in performance on the SART, the N-ADHD group experienced more mind blanking than any of the other three groups. This increased mind blanking was associated with a decrease in on-task and mind-wandering states. We also found that although methylphenidate restored mind blanking in recipients so that it occurred to the same degree as in control participants, it did not improve on-task focus; instead, it increased mind wandering. Methylphenidate, a psychostimulant, is aimed at improving focus (Barkley, 2014). Our results showed that it may not always be a benefit for on-task focus but that it may benefit mind wandering. These results agree with the decoupling hypothesis (Smallwood, 2013) in which mind wandering, as well as on-task focus, necessitate executive resources.
Study 2
In Study 2, we used the same task and thought categories to determine whether the findings of Study 1 would extend to a population of nonclinical young adults.
Method
Participants
Forty participants (22 women; mean age = 23.8 years, SD = 3.6) were recruited from the listings of the Laboratoire de Sciences Cognitives et Psycholinguistique (Paris, France). Table 3 presents detailed demographic and clinical information for these participants. The size of the sample was determined in accordance with a seminal study of mind blanking in adults (Ward & Wegner, 2013), in which the mean sample size across four experiments was 45. All participants spoke fluent French and had normal or corrected-to-normal vision. No participant reported any lifetime psychiatric disorders. We used self-reports from the DIVA (Kooij & Francken, 2010) to identify ADHD symptoms. In accordance with the DIVA guidelines, participants with a score of 5 or higher on a scale from 1 to 9 for either inattention or hyperactivity were assigned to the ADHD profile group (ADHD; n = 15, 5 women; mean age = 22.5 years, SD = 3.7), and the other participants constituted the control group (n = 25, 17 women; mean age = 24.6 years, SD = 3.4). There was no significant difference in age, t(27.34) = 1.78, p > .08, but the ratio of men to women was significantly higher in the ADHD group than in the control group, χ2(1) = 4.55, p < .05, as is found in clinical populations.
Demographic and Clinical Characteristics of the Adult Participants in Study 2
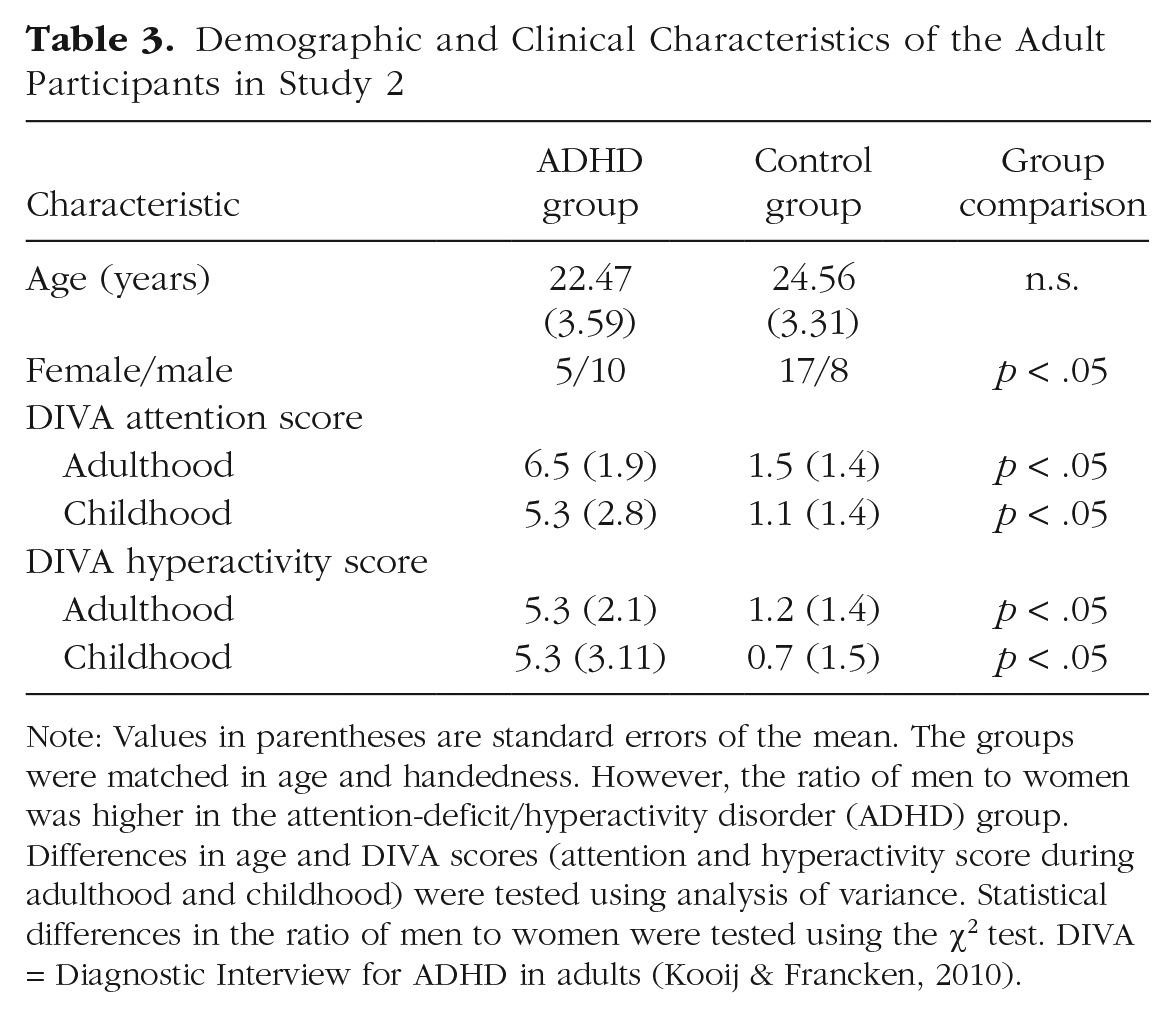
Note: Values in parentheses are standard errors of the mean. The groups were matched in age and handedness. However, the ratio of men to women was higher in the attention-deficit/hyperactivity disorder (ADHD) group. Differences in age and DIVA scores (attention and hyperactivity score during adulthood and childhood) were tested using analysis of variance. Statistical differences in the ratio of men to women were tested using the χ2 test. DIVA = Diagnostic Interview for ADHD in adults (Kooij & Francken, 2010).
Procedure
In contrast to Study 1, the testing occurred in a quiet room in the absence of the experimenter. The order of the test and the questionnaire were counterbalanced between participants. Participants were told that this test was a control for a study of children, which explained the use of the teddy-bear pictures.
Results
Statistical analyses were identical to those in in Study 1.
Performance on the SART
Accuracy was higher on go trials (99.2%, SD = 0.2) than on no-go trials (55.7%, SD = 1.9; see Table 4). A logistic regression on accuracy (29,760 observations of 40 participants), with factors of trial type (go, no-go), block pace (fast, slow), and group (ADHD, control), confirmed the main effects of trial type, β = −5.39, SD = 0.22, z = −24.71, p < .001, and group, β = 0.52, SD = 0.20, z = 2.54, p < .05. However, the regression revealed no main effect of block pace, p > .1; no interaction between group and trial type, χ2(3) = 2.33, p > .1; and no interaction between group and block pace, χ2(1) = 0.82, p > .250. As in Study 1, we found a significant Block Pace × Trial Type interaction, χ2(1) = 4.91, β = −0.48, SD = 0.21, z = −2.24, p < .05 (see Fig. S1b in the Supplemental Material): Slower pace increased performance in go trials, β = 0.55, SD = 0.21, z = 2.62, p < .01, but had no significant effect in no-go trials, p > .250.
Results From Study 2: Accuracy, Response Time, and Anticipations for the Two Groups Separately and Combined
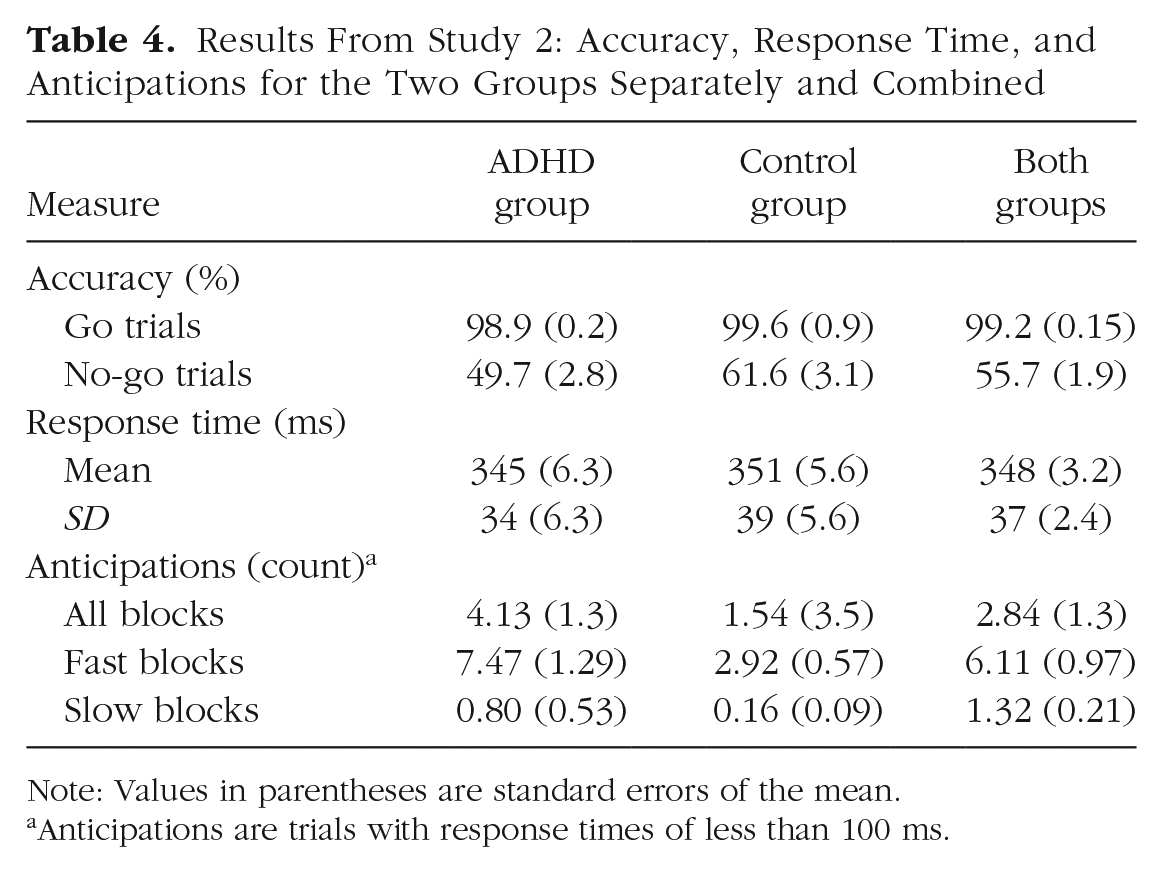
Note: Values in parentheses are standard errors of the mean.
Anticipations are trials with response times of less than 100 ms.
In turn, the Block Pace × Trial Type interaction was qualified by an interaction with group (i.e., a Block Pace × Trial Type × Group interaction), χ2(1) = 4.68, β = 0.91, SD = 0.40, z = 2.25, p < .05. Indeed, the Block Pace × Trial Type interaction was not significant in the control group (p > .250) but was specific to the ADHD group, β = −0.86, SD = 0.41, z = −2.08, p < .05, within which slowing pace improved performance in go trials, β = 0.75, SD = 0.28, z = 2.67, p < .01, but had no effect in no-go trials, β = −0.14, SD = 0.18, z = −0.78, p > .250. In Study 1, all the groups had similar performance profiles except the N-ADHD group, in which there was no Block Pace × Trial Type modulation; by contrast, for the adults in Study 2, ADHD had lower overall performance but displayed a Block Pace × Trial Type modulation that was absent in the control group.
Response times
As in Study 1, there was no effect of group on response times in correct go trials, as assessed by analyses of variance on the mean, the standard deviation, and the coefficient of variation (SD/mean; p > .250, p > .250, and p > .1, respectively; ps > .2 for all interactions with possible block). Fitting of exponentially modified Gaussian distributions at the individual level revealed no significant effect of group, or interaction of block pace with group, on the mean, the variance, or the exponential component (ps > .08). Finally, the ADHD group had more anticipations (8.23, SD = 2.6; Cheyne et al., 2009) than did the control group (3.08, SD = 0.6). We used a Poisson regression for count data to test the statistical significance of this effect. We found that the effect was significant, β = 0.69, SD = 0.35, z = 2.01, p < .05 (see Table 4). The number of anticipations decreased with slower pace, β = −4.46, SD = 1.11, z = −4.01, p < .001, but pace did not interact with group, χ2(1) = 0.09, p > .7.
Subjective reports
Overall, adults reported being on task in 33.8% (SD = 2.6) of the thought probes. The values for the other categories were as follows—task-related interference: 27.5%, SD = 1.8; mind blanking: 19.4%, SD = 1.6; distraction: 7.8%, SD = 1.2; and mind wandering: 21.5%, SD = 2.5. To statistically test the between-groups differences, we used mixed-effects logistic regressions on the likelihood that each of the five possible categories would be reported. In this analysis, participant was a random factor, and group and block pace were fixed factors.
The ADHD group reported about twice as much mind blanking (14.4%, SD = 3.0) as the control group (6.4%, SD = 1.5), β = −1.03, SD = 0.4, z = −2.69, p < .01 (Fig. 1a). Beyond this difference, both groups reported similar values for mind wandering, χ2(1) = 0.26, p > .250 (Fig. 1b); on-task focus, χ2(1) = 0.66, p > .250 (Fig. 1c); task-related interference, χ2(1) = 0.02, p > .250 (Fig. 1d, left); and distractions, χ2(1) = 0.1, p > .9 (Fig. 1e). The interaction of block pace and group was not significant for any of the subjective reports (all ps > .250), but, consistent with previous findings and the view that MW requires executive resources, results for slow blocks, compared with fast blocks, showed an increased likelihood of reporting mind wandering (25.2%, SD = 3.0, vs. 17.8%, SD = 2.4), β = 0.49, SD = 0.1, z = 3.4, p < .001, an effect we did not find in the children, presumably because the slow blocks were already fast for them.
Finally, to test the hypothesis that on-task and mind-wandering states constitute sustained trains of thought that require executive resources, we compared the likelihood of reporting either on-task or mind-wandering states across groups. Indeed, the ADHD group reported significantly fewer instances of on-task focus and mind wandering (50.0%, SD = 2.3) than did the control group (58.5%, SD = 2.3), β = 0.35, SD = 0.2, z = 2.27, p < .05 (Fig. 1f). The two groups reported a similar number of instances of task-related interference and distractions, χ2(1) = 0.01, p > .250 (Fig. 1g). This suggests that, as in Study 1, increased reports of mind blanking in the ADHD group occurred at the expense of on-task and mind-wandering episodes.
General Discussion
Our study presents three main findings and one methodological novelty. First, both clinical and subclinical ADHD increased mind blanking but not mind wandering (understood as content-rich, self-generated, sustained trains of thought). Second, in both studies, this increase in mind blanking was balanced by fewer instances of on-task and mind-wandering states, whereas the frequency of other thoughts (i.e., task-related-interferences and distractions) remained similar. These results agree with the notion that a common mechanism underlies both on-task and mind-wandering states (Smallwood, 2013). Third, in patients with ADHD, methylphenidate increased mind wandering, a finding consistent with the theoretical framework that we have presented. We should stress here that our three main results were found in the absence of any strong differences between groups on the objective behavioral performance in the SART. Finally, this study appears to be the first to use experience sampling with children, and we demonstrated that children’s reports were highly consistent with those of adults.
The higher rate of mind blanking reported by patients with ADHD contrasts with previous studies showing an increase in reports of mind wandering (Franklin et al., 2014; Seli et al., 2015; Shaw & Giambra, 1993). Yet this positive association between mind wandering and ADHD in previous studies necessitated distinctions between “deliberate” and “spontaneous” mind wandering (Seli et al., 2015) and between “aware” and “unaware” mind wandering (Franklin et al., 2014), because only these sorts of mind wandering were associated with ADHD symptoms. The previous studies did not include a mind-blanking category. This underlines the importance of the classification used to describe subjective experiences. Indeed, had our classification implied a forced choice between mind wandering and on-task focus, episodes reported as mind blanking might have been described as mind wandering by default. Thus, our classification is theoretically motivated and seems reconcilable with previous classifications. In addition, its categories rely on experienced content instead of asking for metajudgments aiming at mind-wandering subtypes. We thus believe that this classification is simpler because it directly maps onto first-order verbal reports and is likely to be easier for children. Further research is needed, however, to systematically assay the validity of extant mind-wandering classifications and to decide in particular whether metajudgments help refine classifications based on first-order contents.
Our second main result was that the increase in mind blanking was compensated for by a conjoint decrease of on-task focus and mind wandering. This result is consistent with the view that mind wandering and on-task focus share common cognitive mechanisms that are based on the recruitment of executive functions (Christoff et al., 2009, 2016; Smallwood, Brown, Baird, & Schooler, 2012). The result is also consistent with the known association of executive deficits and metacognitive disabilities (Antshel & Nastasi, 2008; Knouse et al., 2005; Shimamura, 1994); we found that the ability to report mental content is impaired with the executive-functions deficit of ADHD.
The involvement of executive functions in mind wandering may also be essential to interpreting our third finding, that methylphenidate increased reports of mind wandering. Methylphenidate is aimed at improving sustained attention (Barkley, 2014). Here, we showed that it also fostered the unfolding of rich self-generated thoughts, which suggests that sustained attention on external focal tasks depends not only on executive control but also possibly on other factors. One such factor could be motivation, which is known to be weaker in ADHD (Volkow et al., 2011), whereas stronger motivation reduces mind wandering independently of executive control (Mrazek et al., 2012). Indeed, methylphenidate may buttress sustained trains of thought without any impact on the motivation to perform a tedious task such as the SART. If so, in patients with ADHD who are medicated, restored executive resources may be applied to emerging internal representations, converting them into full-fledged mind wandering or facilitating their access to awareness. Further studies are needed to weigh the respective contributions of motivation and executive resources in the maintenance of an external focus. We should note here that previous studies about mind wandering in ADHD (Franklin et al., 2014; Seli et al., 2015; Shaw & Giambra, 1993) did not mention whether participants were medicated, which opens the possibility that elevated reports of mind wandering were due to undocumented treatment.
Our results are consistent with the hypothesis that executive recruitment is common to self-generated (mind wandering) and externally maintained (on-task) trains of thought (Smallwood, 2013). They are also consistent with the neural evidence that deliberate mind wandering correlates with increased functional connectivity between executive-control regions and the default network (Golchert et al., 2017), but ADHD patients show decreased connectivity between these two networks (Castellanos et al., 2008). However, our results do not provide further evidence on the cognitive nature of these mechanisms, in part because the use of thought probes makes it difficult to disentangle processes initiating a thought episode from those controlling its maintenance: Probing is inadequate to distinguish duration and frequency of mind-wandering episodes (Bastian & Sackur, 2013). Thus, the deficit of executive functions associated with ADHD (Barkley, 1997) could decrease the number of reports of sustained trains of thought (i.e., mind wandering and on-task focus) according to at least two different mechanisms, in addition to its impact on metacognition. First, fewer executive resources might generate fewer episodes of sustained thoughts. Second, it could be that onsets of sustained trains of thought occur normally but with shorter durations. They would be consequently less likely to be caught by probes.
In addition, a number of nonexclusive cognitive mechanisms could account for the increase of mind blanking with ADHD symptoms. First, mind blanking could reflect deficiencies in metacognition. This view would be consistent with some studies suggesting metacognitive deficits in ADHD (Antshel & Nastasi, 2008; Knouse et al., 2005). Alternatively, mind-blanking reports might be introspectively accurate reports of blank states (Ward & Wegner, 2013), a situation that occurs in extreme forms in the syndrome of auto-activation deficit (Leu-Semenescu et al., 2013). Finally, blank reports could reflect mixed or confused states occurring at the transition between episodes in the stream of consciousness (James, 1890). This view would be consistent with the notion that ADHD patients may experience many short episodes of inchoate mind wandering that fail to be sustained. Further studies should attempt to weigh the relative contributions of these different mechanisms.
The present study suggests that mind wandering is not responsible for increased attentional lapses in ADHD. We suggest instead that patients with ADHD have difficulties sustaining trains of thought in general, be they internally or externally oriented. The consequence of these difficulties is an increased amount of mind blanking, which could correspond to metacognitive deficits, among other potential mechanisms. Methylphenidate medication reverts mind-blanking frequency to baseline but surprisingly increases mind wandering rather than on-task focus. All these results point to a shared mechanism underlying on-task focus and mind wandering, potentially a mechanism based on executive control (Smallwood, 2013). They also call for a closer inspection of the role of other factors, such as motivation, that may be crucial to the proper orienting of attention in ADHD.
Footnotes
Acknowledgements
We thank Jonathan Smallwood for his insightful input at various stages of the study and Isabelle Brunet for her help in data acquisition for the adult study. We also thank very warmly the children and the families who participated in the project.
Action Editor
John Jonides served as action editor for this article.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This work was supported by Agence Nationale de la Recherche Grants ANR-10-IDEX-0001-02 (to Paris Sciences et Lettres Research University) and ANR-10-LABX-0087 (to l’Institut d’Etude de la Cognition).
Open Practices
All data and materials have been made publicly available via the Open Science Framework and can be accessed at https://osf.io/8wtae/. The complete Open Practices Disclosure for this article can be found at http://journals.sagepub.com/doi/suppl/10.1177/0956797617708234. This article has received badges for Open Data and Open Materials. More information about the Open Practices badges can be found at ![]() .
.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.