
Abstract
People sick with infectious illnesses face negative social outcomes, like exclusion, and may take steps to conceal their illnesses from others. In 10 studies of past, current, and projected illness, we examined the prevalence and predictors of infection concealment in adult samples of U.S. university students, health-care employees, and online crowdsourced workers (total N = 4,110). About 75% reported concealing illness in interpersonal interactions, possibly placing others in harm’s way. Concealment motives were largely social (e.g., wanting to attend events like parties) and achievement oriented (e.g., completing work objectives). Disease characteristics, including potential harm and illness immediacy, also influenced concealment decisions. People imagining harmful (vs. mild) infections concealed illness less frequently, whereas participants who were actually sick concealed frequently regardless of illness harm, suggesting state-specific biases underlying concealment decisions. Disease concealment appears to be a widely prevalent behavior by which concealers trade off risks to others in favor of their own goals, creating potentially important public-health consequences.
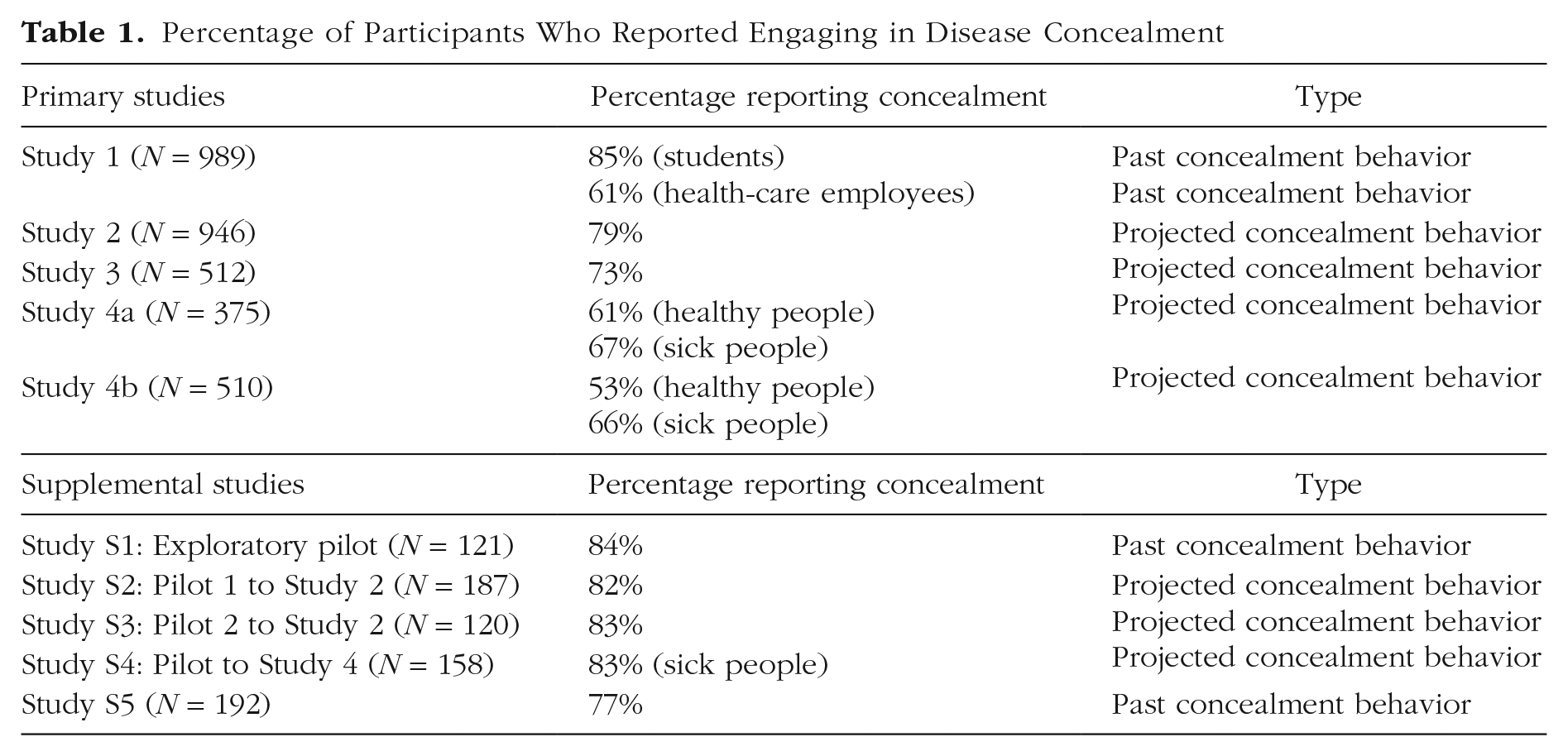
Have you ever hidden the fact that you were sick with a contagious illness from people around you? Perhaps you stifled a cough during a work meeting or neglected to mention your scratchy throat on a first date. Maybe you even assured others your stuffy nose was merely due to allergies. If you admitted to any such concealment behaviors, you certainly are not alone—in the following studies, around 75% of U.S. adult participants reported concealing infectious illness from others (Table 1). But just because concealment is common does not mean it is costless: Masking signs of illness can facilitate interpersonal disease transmission. One survey reported that 82% of workers in the United Kingdom believed they had become sick because a coworker came into the office not feeling well (Calnan, 2014). Anecdotes about concealment during the COVID-19 pandemic include people covering up symptoms to board flights and government officials hiding COVID-positive tests for political gain (Gabriel, 2020; Whitley, 2020). Despite such occurrences, the psychological underpinnings of when and why people conceal contagious illnesses have received little empirical attention.
Percentage of Participants Who Reported Engaging in Disease Concealment
Motivations for Disease Concealment
Why might people want to hide sickness from others? Work on the psychology of disease management highlights a motivational trade-off between avoiding infectious illness and affiliating with others (Sacco et al., 2014; Sawada et al., 2018). Healthy people tend to act disgusted by individuals showing signs of contagious illness and may avoid and even forcefully isolate them (Ackerman et al., 2018; Murray & Schaller, 2016; Oaten et al., 2011; Regenbogen et al., 2017). Thus, from the perspective of people navigating social interactions while sick, the costs of their illness are social as well as physical.
These social costs could facilitate concealment behaviors. Consider an example from the animal kingdom. While in isolation, infected zebra finches exhibit sickness behaviors, which help conserve energy and prioritize illness recovery. However, these sickness behaviors are muted when finches reside in social colonies, potentially because appearing unhealthy while in a group could threaten the pursuit of social goals like mating (Lopes et al., 2012). Humans may be similarly motivated to hide signs of illness to preclude negative interpersonal reactions while pursuing other goals. Building from this perspective, we examine the prevalence of human disease concealment in social settings and highlight psychological predictors of concealment.
Sickness Characteristics Influencing Disease Concealment
At least two characteristics make infectious-disease concealment unique: factors associated with the sickness itself and factors associated with the individual.
Sicknesses vary in duration and in the potential harm afforded to others. Illness harm can be represented by two dimensions: transmission risk (ease of disease spread) and symptom severity (the physical impairments a disease causes). Generally, transmissible and severe illnesses are more harmful than illnesses that spread less easily and have mild symptoms. These dimensions also closely map onto general models of risk assessment: People commonly make decisions on the basis of their perceptions of event likelihood and the potential event impact (e.g., Breakwell, 2014). People may choose to conceal less when they view their illnesses as more likely to cause interpersonal harm, if one presumes a general aversion to harming others (e.g., Crockett et al., 2014). We predict that, if decision-makers are sensitive to this interpersonal danger, they may use perceptions of illness harm as inputs into the concealment-decision process. On top of illness harm, longer-lasting illnesses imply more chances of repeated interpersonal interactions in which disease can be spread. People are generally less deceptive when they expect multiple interactions with the same person (Ben-Ner & Hu, 2021), and thus concealment may be less likely for longer-lasting illnesses. Alternatively, people may be relatively more likely to conceal longer-lasting illnesses because repeated interactions heighten self-presentational concerns (Baumeister, 1982) and because the potential for more indirect social costs increases (e.g., missing out on multiple events as opposed to just one).
The primary sickness factor associated with the individual involves illness immediacy—whether decision-makers are currently sick or not. Someone forecasting the possibility of concealing a future infectious illness may not attend to, or consider important, the same information as someone currently gripped by disease. Research indicates that actively experiencing a state can stimulate different psychological processes and consequences versus perceiving that state more remotely (e.g., Kivetz et al., 2006; Trope & Liberman, 2010). For instance, smokers planning to quit often underestimate the misery and difficulty of sticking to this conviction during active cravings (Loewenstein, 2005). In the context of disease concealment, currently sick people may find that the salience of physical symptoms and goal-tradeoff pressures (e.g., to continue engaging in social activities) encourage concealing illnesses more than when merely imagining their future decisions.
Statement of Relevance
People often experience negative reactions toward others who seem sick with contagious illnesses. To elude such outcomes, sick people may take steps to conceal their illnesses. Indeed, across health-care employees, university students, and general adult samples, we found that a large majority of people report having concealed an active infectious illness. People reported boarding flights, treating patients, and going on dates while hiding signs of sickness. Interestingly, when illnesses were most severe, people currently sick reported concealing even more than people who merely imagined being sick, suggesting a potentially serious public-health problem: Sick people may be relatively unmindful about the possible harm they could do by interacting with others. As most people in our samples reported concealing for social reasons (i.e., to avoid missing activities or upsetting others), novel approaches may be needed to mitigate this harmful concealment behavior.
Other Approaches to Concealment
Beyond infection status, at least two robust literatures in social psychology have focused on the concealment of other kinds of personal information. First, the literature on secret-keeping has identified numerous categories of social information (ranging from sexual infidelity to financial hardship) that people withhold from others, how frequently people hold these secrets, and the psychological consequences of doing so (e.g., Slepian et al., 2017). Second, the literature on concealable stigmatized identities focuses on when people conceal aspects of their identities they believe will be judged negatively, such as sexual orientation (Newheiser & Barreto, 2014; Quinn & Chaudoir, 2009). These two perspectives help inform some aspects of infectious-disease concealment. Considering that the process of secret-keeping begins with the intention to hide information from others (Slepian, 2022), both intentions and acts of actual concealment represent forms of infectious-disease concealment. With respect to the content of concealment, drawing on the stigmatized-identity literature, we should expect that people will conceal infectious illnesses to the extent that those illnesses trigger negative assessments. For instance, research on concealable stigmatized identities has shown that certain diseases viewed as morally objectionable (e.g., HIV, COVID-19) create identity threat and heightened motivation for concealment in those infected (Earnshaw et al., 2020; Lee et al., 2002).
But we also expect that disease concealment is distinct from both general secret-keeping and identity-relevant concealment in at least two focal ways. First, the information that disease concealers are hiding involves the potential transmission of pathogenic material. Consider that, of 38 categories of secrets previously identified (Slepian et al., 2017), none affords direct physical harm to the person from whom information is being concealed. Any harm that occurs from these other forms of concealment is indirect (e.g., emotional harm caused by an extramarital affair), and is, notably, only realized when the information is revealed. In contrast, infectious-disease concealment involves direct, physical harm in interpersonal interactions regardless of the success of that concealment.
Second, though hiding a secret romantic affair or marginalized sexual identity may help concealers avoid moral judgment and mistreatment, people sick with common illnesses are not typically blamed or stigmatized just for having those illnesses. Indeed, in a taxonomy detailing 93 different kinds of stigma (Pachankis et al., 2018), only one (sexually transmitted diseases) represented an infectious illness, with that category of illness often being judged on moral grounds (Young et al., 2007). Further, because many infectious illnesses are ordinary in the sense that all people suffer from them, sometimes frequently (e.g., the common cold; DerSarkissian, 2022), it is unlikely that such infections will lead to long-lasting reputational damage.
Thus, existing theories of concealment may miss important contexts and characteristics linked to infectious disease. To help make this case, we measure transmission of physical harm in Study 2, Study 4a, and Study 4b, and identity and stigma concerns in Study 4a and Study 4b, to examine whether infectious-disease characteristics predict concealment over and above other concerns.
Current Research
We first descriptively examine the general prevalence of infectious-disease concealment in two settings where disease spread is salient and reporting illness is encouraged, if not mandated: universities and health-care systems (Study 1). Our experiments then targeted sickness-related factors, including illness harm (Study 2) and duration (Study 3). Finally, we employed novel sampling techniques to recruit participants actually sick with infectious illnesses and compare their decisions to those of healthy participants, while also examining factors (e.g., stigma) known to influence concealment of identity-focused information (Studies 4a and 4b). Together, these studies pursue two primary goals: to document the prevalence of infectious-disease concealment and to address two factors relevant to the context of disease concealment—those pertaining to the sickness, and those pertaining to the individual. Across studies, samples included U.S. participants varying on age, socioeconomic status, gender, ethnicity, and professional background (e.g., health-care employees; see Table S2 in the Supplemental Material available online for full demographics). All studies were powered to detect small effect sizes ( f = 0.08–0.18), given a lack of prior research on infectious-disease concealment.
Open Practices Statement
Pilot studies, materials, data, code, and preregistrations can be found on the Open Science Framework (https://osf.io/r9cug/), and additional details are available in the Supplemental Material. Exclusion criteria are reported in the Supplemental Material and the preregistrations.
Study 1: Disease Concealment in the Face of Illness Reporting Policies
Method
This study (and all others in this article) were approved by the Institutional Review Board of Health Sciences and Behavioral Sciences at the University of Michigan to ensure adequate protections of participants. Through email, we invited 5,000 students and 6,802 health-care employees at a midwestern U.S. university to participate in exchange for entry into a gift-card raffle, and 1,473 respondents participated between December 16, 2021, and January 14, 2022. After excluding people who did not report being sick at all during any point of the pandemic or who had no in-person interaction with students or coworkers, our final sample included 989 participants (505 students and 399 health-care employees).
Participants first reported how many days they had felt sick with symptoms of an infectious illness since March 2020 (around the start of the COVID-19 pandemic in the United States). Then participants indicated how frequently they had resorted to three types of concealment strategies to cover up signs of their sickness, using a 7-point scale ranging from 1 (never) to 7 (all the time). The strategies included (a) participants actively covering up symptoms from others (commission), (b) coming to campus or work in person without telling others they were feeling sick (omission), (c) coming to campus or work in person feeling sick without filling out daily symptom-screeners that were mandatory for all individuals using campus facilities (e.g., the university’s symptom-screening app). Finally, in an open-ended format, participants wrote why they covered up the fact that they were sick from others around them. These open-ended responses were coded independently by two groups of research assistants; see the Supplemental Material for details.
Results
Seven hundred sixteen (72.3%) participants reported hiding an infectious illness through commission (actively covering up signs of illness), omission (not disclosing sickness to others), or ignoring a mandatory app-based symptom checker. This included 85% (428 of 505) of students and 61% (243 of 399) of health-care employees. Only 5 participants openly reported concealing COVID-19.
Participants explained the motivations underlying their concealment decisions in a variety of ways. Thematic qualitative coding revealed that participants frequently concealed illness because their illness would conflict with their other social goals (e.g., going on a date); very infrequently they cited pressure from institutional policies (e.g., lack of paid time off) as a motivation for concealment (Table 2). This latter finding may be due to the presence of policies supporting sick leave (though such policies are likely to vary by work division and instructor), but it does suggest that disease concealment stems from a variety of motives. Further, despite institutional strategies to encourage illness disclosure, disease concealment appears to be widespread in both settings.
Motivations for Concealment (Study 1)

Note: Responses were not mutually exclusive.
Study 2: Illness Harm (Symptom Severity and Transmission Risk)
Method
We recruited 947 participants through Prolific Academic on August 1, 2023. After applying preregistered exclusion criteria, our final convenience sample was 946 participants.
The study used a 3 (Symptom Severity) × 3 (Transmission Risk) between-subjects design. We randomly assigned participants to one of nine conditions in which they imagined being sick while in a social situation with a few strangers. The sickness they imagined being sick with varied in both symptom severity and transmission risk. Symptoms were designated as mildly severe (e.g., having trouble concentrating on work and school), moderately severe (e.g., needing to take days off of work and school), or very severe (e.g., not being able to study or work at all). Transmission risk was designated as low, medium, or high. Participants were told not to imagine COVID-19 as, unlike most common infections, COVID-19 infection may be judged a moral failing and therefore concealed because of anticipated stigmatization (Henderson & Schnall, 2021). A self-reported attention check suggests that 85% of participants (801 of 946) followed these instructions. Adding this attention check as a covariate did not significantly change the primary results (see the Supplemental Material). Therefore, we report analyses conducted on the full sample of 946 participants.
Participants rated how likely they would be to (a) hide, (b) conceal, and (c) cover up their disease in the situation on a 7-point scale (1 = extremely unlikely, 7 = extremely likely). The average of the responses on the three items was used as an index of the likelihood of concealment (across vignettes, αs = .97).
Results
Consistent with predictions, a 3 × 3 analysis of variance revealed a main effect of symptom severity, F(2, 937) = 8.10, p < .001, f = 0.13, 95% confidence interval (CI) = [0.06, 0.19]: Participants were significantly more likely to report concealing illness when symptom severity was low (M = 3.69, SD = 1.95) than when severity was moderate (M = 3.24, SD = 1.89), t(631) = 2.96, p = .006, f = 0.12, 95% CI = [0.15, 0.75] or high (M = 3.09, SD = 2.03), t(623) = 3.77, p < .001, f = 0.15, 95% CI = [0.29, 0.91]. There was no main effect of transmission risk, F(2, 937) = 1.62, p = .199, f = 0.06, 95% CI = [0.00, 0.12], counter to predictions (but see Studies S2 and S3 in the Supplemental Material). However, an interaction between symptom severity and transmission risk, F(4, 937) = 2.89, p = .021, f = 0.11, 95% CI = [0.01, 0.16], indicated that low (vs. high) symptom severity caused higher concealment likelihoods at low levels of transmission risk, t(204) = 2.66, p = .025, f = 0.19, 95% CI = [0.19,1.27], and medium levels of transmission risk, t(206) = 4.23, p < .001, f = 0.29, 95% CI = [0.62, 1.69], but not at high levels of transmission risk, t(207) = −0.26, p = .79, f = −0.02, 95% CI = [−0.61, 0.47]. Together, these patterns indicate that people reported being less likely to conceal when symptom severity increased and when transmission risk was very high. Two pilot studies showed comparable effects (with some differences due to use of within-subjects designs). These findings suggest that people prioritize the potential for negative interpersonal consequences in their concealment decisions, at least when they are imagining illnesses.
Study 3: Illness Duration
Method
We recruited 603 participants from Prolific Academic on August 3, 2023. After applying our preregistered exclusion criteria, we obtained a final sample of 512. Participants were told to imagine attending a recurring social event that happens about once a week (e.g., weekly classes, volunteering) where they would encounter several other people whom they did not know very well but who were regular attendees. We randomly assigned participants to imagine having an illness with either a short duration (3–5 days) or a long duration (12–14 days). Illness harm was held constant across the conditions, with the illness described as being moderately transmissible and as having mild symptom severity. Participants were reminded that they would be sick either for a single interaction (for the short-duration illness) or for multiple interactions (for the long-duration illness). Then they filled out the same three-item concealment measures used in Study 2 (α = .98) for the first social interaction. As in Study 2, participants were asked not to imagine being sick with COVID-19, and 93% of participants (474 of 512) self-reported that they followed these instructions; treating this attention check as a covariate did not change the primary results (see the Supplemental Material). We report analyses conducted on the full sample of 512 participants.
Results
Contrary to our competing preregistered hypotheses (longer illness duration makes concealment more likely vs. longer illness duration makes concealment less likely), people did not differ in their concealment of short-duration illnesses (M = 3.36, SD = 2.10) versus long-duration illnesses (M = 3.40, SD = 2.12), t(495) = 0.19, p = .85, f = 0.01, 95% CI = [−0.33, 0.40]. That is, anticipated illness duration did not influence prospective concealment decisions. We return to possible reasons for this in the Discussion section.
Studies 4a and 4b: Concealment in Currently Healthy (vs. Sick) People
Our final area of investigation targeted the illness state of the decision-maker. The immediacy of illness—whether someone is currently sick or not—may alter which factors are prioritized in the decision process. In Studies 4a and 4b, we therefore recruited both sick people (reporting on their actual, current illness) and healthy people (reporting on an imagined illness, as in Studies 2 and 3) and compared their concealment intentions as a function of illness harm. This approach allowed us to extend this paradigm to individuals who may have been actively contemplating infectious-disease concealment in their own lives. If both groups reported concealment patterns similar to those in Study 2, this would suggest that concealment is prevalent primarily for less harmful illnesses. Alternatively, concealing sickness may be easier said than done, with the assessments of the costs (e.g., infecting others) and benefits (e.g., pursuit of social goals) associated with concealment depending on whether someone is actually sick or is merely imagining being sick. To test whether infectious-disease concealment is distinguishable from other forms of concealment, we also included measures from past studies of concealable stigmatized identities.
Studies 4a and 4b used identical methods and followed largely similar preregistration criteria. We combined these studies to improve statistical power and address journal word limits (study was included as a covariate in the analyses). For individual study preregistration details and separate analyses of each study, please see the Supplemental Material.
Method
These studies used a 2 (illness status: sick, healthy) × 5 (symptom severity: not at all severe – extremely severe) between-subjects design. We recruited 375 participants (184 sick, 191 healthy) from November 10, 2021 to November 11, 2021 (Study 4a) and 525 participants (261 sick, 264 healthy) from December 20, 2021 to December 28, 2021 (Study 4b) via CloudResearch.
We excluded participants who did not match the illness status of the survey (i.e., those who reported being sick in the survey for healthy participants and those who reported being healthy in the survey for sick participants); we also excluded those who were presently sick with COVID-19, those who completed the survey in less than 1 min or more than 45 min, those who wrote nonsensical responses to free-response questions, and those who failed two quality-check questions. We also excluded sick participants who reported significantly different symptoms at the beginning and end of the survey and healthy participants who reported significantly different symptom severity compared to their assigned severity condition. This led to a final sample of 852 participants (424 healthy, 428 sick).
Two separate surveys were advertised to workers. Each included a prescreening element to assess current illness. In the sick survey, the survey was terminated for participants who reported no such sickness or who failed to respond. Participants who indicated that they felt sick with an illness that could be infectious, or who were unsure whether their sickness was infectious, reported their symptoms and the type of infectious illness (e.g., respiratory illness, skin infection, gastrointestinal issue).
In the healthy survey, the survey was terminated for participants who reported an infectious illness or who failed to respond. Participants who were unsure whether or not they were sick with an infectious illness were excluded from the final analyses. Next, healthy survey participants imagined they were feeling sick with an infectious illness as they responded to the same set of questions used in the sick survey.
Illness harm
Illness harm represents a standardized composite of symptom severity and transmission risk. Participants who reported being currently sick indicated symptom severity on a scale ranging from 1 (not at all severe) to 5 (extremely severe). Healthy participants were randomly assigned to one of five severity conditions that approximated the distribution of the sickness-severity measure recorded from the first 100 actually sick participants (to allow for this calculation, the first 100 participants in the sick survey were recruited before we launched the healthy survey). This resulted in 71% overlapping distributions of severity across illness conditions (see Fig. S5b in the Supplemental Material). As a manipulation check, participants in the healthy condition were asked to report their assigned symptom-severity level again, and participants in both conditions described the symptoms of their actual or imagined illness.
For transmission risk, participants were asked to think about their current (or imagined) illness and respond to the following three items (α = .94): (a) “How contagious do you think your illness is?” (1 = not contagious at all, 7 = extremely contagious); (b) “If you came into close contact with another person, how likely do you think it is that they would contract your illness?” (1 = not likely at all, 7 = extremely likely); (c) “How easy do you think it would be for your illness to be transmitted to others?” (1 = extremely difficult, 7 = extremely easy).
Stigmatized identities
Participants evaluated their illness on measures commonly associated with stigmatized identities (illness centrality, salience, and anticipated stigma; adopted from Quinn & Chaudoir, 2009). For illness centrality, participants responded to four items about how important their current (or imagined) illness is to their identity, using a 7-point scale (1 = strongly disagree, 7 = strongly agree; α = .86), and for illness salience, they answered one item about how often they think about their illness (1 = almost never, 7 = constantly). For anticipated stigma, they indicated how likely they would be to receive seven types of negative feedback if others around them knew about their illness (1 = definitely would not occur, 7 = definitely would occur; α = .91).
Concealment
Participants read a vignette (adapted from Ackerman et al., 2020) describing a situation in which the participant was not feeling well but was asked to go to an important in-person meeting with one other individual. The meeting required the participant and the other person to be in a room together for several hours by themselves. After reading the vignette, participants answered the following three questions: “How likely are you to hide[conceal][cover up] the fact that you are currently sick from the other employee?” (1 = extremely unlikely, 7 = extremely likely; α = .98). The vignette approach was chosen to ensure that both sick and healthy participants could respond to equivalent situations.
Results
Effects of illness status on concealment
Regressing concealment intentions on illness status and illness harm indicated that sick participants were more likely to conceal than healthy participants, b = 0.50, t(832) = 3.62, p < .001, an effect qualified by a significant illness-status and illness-harm interaction, b = 0.61, t(832) = 3.64, p < .001 (see Fig. 1). Replicating results from Study 2, healthy participants reported being more likely to conceal when the potential harm of their imagined illness was low than when it was high, b = −0.64, t(832) = −5.76, p < .001. However, a different pattern emerged for sick participants: They were equally likely to conceal their actual illness from others regardless of how harmful it was, b = −0.03, t(832) = −0.25, p = .80 (this sick-participant result was replicated in Study S4; see the Supplemental Material). Comparing both groups, at high levels of illness harm, currently sick participants reported concealing more than participants who merely imagined being sick, b = 1.00, t(832) = 5.08, p < .001.

Concealment likelihood by illness harm and illness status.
Stigma, salience, and centrality of infectious illness
The same pattern of disease concealment was observed even when controlling for factors related to stigma and identity. We entered anticipated stigma, identity centrality, and identity salience as individual covariates into the primary moderation model. In this new model, all of the illness-harm and illness-status effects remained: Sick people reported concealing illness more frequently than healthy people, and a comparable interaction between illness status and illness harm emerged (see the Supplemental Material for full results). People also reported being more likely to conceal illness if they felt stigmatization would result from their illness, b = 0.39, t(829) = 5.19, p < .001, and if they felt their illness was central to their identity, b = 0.25, t(829) = 3.37, p < .001. However, people (especially currently sick people) concealed illnesses even when accounting for these factors, suggesting that other characteristics, such as the motivations identified earlier (e.g., social goals, professional goals), continue to encourage concealment. Infectious illnesses also were perceived differently on several dimensions compared to stigmatized identities (see the Supplemental Material for details), highlighting the uniqueness of this domain of concealment.
General Discussion
Sickness is a common experience, but the present studies indicate it is an experience commonly hidden from others. Infectious-disease concealment is motivated by personal and social reasons and is particularly likely when the extent of potential harm to others is low. Such findings highlight the trade-offs people make between societally normative motives (e.g., honesty, not causing harm) and personally desirable motives (e.g., pursuing one’s goals, not worrying others). Perhaps most importantly, we observed a state-specific bias: Healthy people who imagined being sick reported lower concealment intentions than did people who were actually sick, especially when the illness was harmful. That is, when healthy, people may believe that they would not risk severe harm to others, but when sick, they appear relatively insensitive to this exact risk. This insensitivity is especially pernicious when we consider the contexts where concealment was reported, including health-care facilities, college classrooms, and workplace environments.
Could people simply refrain from concealing illness when it is difficult (e.g., when there are severe symptoms that are hard to mask, or when illnesses must be concealed frequently)? This possibility is inconsistent with the present findings. Sick participants, who should be especially sensitive to the relative difficulty of hiding mild versus severe symptoms, were more likely to conceal severe illnesses than were people imagining illness. Illness duration also did not change decisions; this latter finding was surprising, but it is consistent with some prior research on lying (DePaulo & Kashy, 1998) that showed that interaction frequency is a less reliable predictor of lying than factors such as relationship closeness. (We also found relationship closeness to be critical in disease-concealment decisions; see Study S5 in the Supplemental Material.)
Theoretical contributions
This work makes theoretical contributions to at least two broad literatures. First, research on the psychology of sick people (e.g., sickness behavior) has historically focused on intrapersonal processes such as the emotional experience of sickness (i.e., lassitude; Schrock et al., 2020) or changes in neural activity as a function of inflammation (Muscatell et al., 2016). In comparison, research on human pathogen management psychology, including models such as the behavioral immune system, primarily addresses preinfection processes (e.g., detecting and avoiding infection threats; Ackerman et al., 2018; Schaller & Park, 2011). The current studies are embedded within the (former) sickness-psychology space because they focus on decisions made by infected individuals, but they also bridge a gap between these two literatures by emphasizing the motivations and trade-offs at play in social interactions that include infected individuals and other noninfected individuals, thereby addressing calls for such intersectional research (e.g., Muscatell & Inagaki, 2021).
Thus, the disease-concealment paradigm may help advance theory connecting these two literatures. For example, the motivational trade-offs producing concealment suggest that people high in affiliative motives or social-exclusion concerns (Neel et al., 2016) may be particularly sensitive to the social costs of sickness and thus may conceal illness more often. Conversely, sickness signaling may also function deceptively as a support-seeking device; people may exaggerate symptoms to facilitate interpersonal care or achieve other goals. Both sickness exaggeration and concealment may act as costly signals (Steinkopf, 2017). For instance, exaggerators risk social exclusion because of others’ pathogen-avoidance mechanisms, whereas concealers risk social exclusion because of others’ cheater-detection mechanisms. We expect these deceptive signals to be flexibly employed on the basis of factors modulating potential costs and benefits, such as interactant closeness and motive strength (see also Lasselin et al., 2018; Shattuck et al., 2021; Steinkopf, 2017).
A second contribution is that these studies distinguish infectious-disease concealment from existing perspectives on withholding other forms of information in social interactions; these range from general secret-keeping (e.g., Slepian, 2022) to stigmatized identities (e.g., Chaudoir & Fisher, 2010) to interpersonal deception theory (e.g., Buller & Burgoon, 1996). None of these approaches focus on the possibility of directly harming others as a possible outcome of concealment, though they do suggest that indirect social harms may stem from associating with stigmatized individuals or morally laden content (e.g., cheating, illegal activity; Slepian et al., 2017). Although we found that people can anticipate stigma from being sick with common illnesses, there are multiple conceptual differences that separate disease concealment from the concealment of stigmatized identities. The concealable-stigma literature focuses primarily on self-aspects that are more permanent (i.e., identity) but that are less prevalent in populations than common diseases. For instance, not every American holds a stigmatized identity, but the average American adult suffers an average of two to four colds per year (DerSarkissian, 2022). These qualitative differences between identities and illnesses may produce different psychological experiences: Infectious illnesses seem to be salient, but not central, parts of our identities (see the Supplemental Material), whereas literature on concealable stigma highlights identities as central but not as salient (Quinn & Chaudoir, 2009). Together, disease concealment involves unique theoretical considerations that stand apart from other domains of concealment as a potentially dangerous decision that every person faces at some point.
Practical implications and future directions
Future work would greatly benefit from examining concealment in other cultural contexts and across time. Our studies focused on U.S. participants, but societies vary in how strictly people adhere to and enforce norms, potentially shaping how diseases are spread (e.g., Gelfand et al., 2021). People in tight cultures may be hesitant to hide illness if the punishment for being caught is harsh; the price to be paid might outweigh the possibility of obtaining goals through successful concealment. Norms may also be codified in regulations. Very few of the health-care employees we sampled (< 10%) explicitly mentioned regulations (e.g., restricted sick leave) as drivers of disease concealment. This may be because they enjoyed sufficient sick leave, but even in settings where absences are presumably allowed, a majority still reported concealing for other reasons. Further, our data collection spanned 3 years, and COVID-19 was a known entity for all participants. We took steps to account for the unique historical backdrop of the pandemic (e.g., measuring retrospective concealment across one’s life and prospective concealment in future situations, excluding COVID-19 infections in most studies), but it may be that proximity to the pandemic has shaped how people think about concealment. Longitudinal designs may also illuminate more about the experience of concealing illness from others (e.g., mind wandering and well-being; Slepian et al., 2017). For instance, we expect concealers to experience predecision worry and postdecision guilt. However, the target of such mechanisms may differ by concealment domain—guilt is likely to be experienced by disease concealers primarily if they learn that an interactant became sick, whereas guilt should be less tied to the act of concealment itself because of the uncertain nature of the threat. That is, as germs are invisible and transmission is not ensured, concealers may plausibly deny that they are dangers to others, thereby minimizing the sense that one’s concealment decision is a violation. Future work could attend to at least some of these possible influences, including how social and institutional pressures change as a function of ecological shocks (e.g., pandemics) and medical advances (e.g., vaccine availability).
Finally, these findings have broad public-health implications. Insofar as concealment facilitates illness transmission, it likely adds substantial economic and operational burdens to corporate, health-care, and educational systems (e.g., Hemp, 2004; Mogharab et al., 2022; Ridenhour et al., 2011). The diseases participants reported concealing here were largely respiratory (~80% in Studies 1–3), which are both common and financially taxing (the annual costs of the common cold have been estimated at approximately $25 billion; Bramley et al., 2002). In view of the fact that 40% of the students in our Study 1 reported improper use of a daily symptom screener, effective self-disclosure of illnesses appears to require more than simply relying on goodwill. The development of future interventions may target factors identified here as key leverage points. For instance, the relative insensitivity to interpersonal harm shown by sick participants indicates that emphasizing the potentially injurious consequences of concealment may be insufficient. Instead, to the extent that sick people are thinking in concrete, self-focused ways, they may be more receptive to interventions targeting immediate punishments or alternate ways to achieve their social goals. Though the crafting of effective strategies to prevent infectious-disease concealment will first require more foundational research, we hope the current work provides initial insights useful for meeting this challenge.
Supplemental Material
sj-docx-1-pss-10.1177_09567976231221990 – Supplemental material for When and Why People Conceal Infectious Disease
Supplemental material, sj-docx-1-pss-10.1177_09567976231221990 for When and Why People Conceal Infectious Disease by Wilson N. Merrell, Soyeon Choi and Joshua M. Ackerman in Psychological Science
Footnotes
Transparency
Action Editor: Patricia J. Bauer
Editor: Patricia J. Bauer
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.