
Abstract
Background
Patients with vestibular disorders frequently avoid specific environments and activities due to the fear of dizziness episodes. However, this fear avoidance belief and behavior may inhibit the compensatory mechanisms of the vestibular system, thereby impacting the rehabilitation process. The Vestibular Activities Avoidance Instrument-9 (VAAI-9) is a 9-item tool specifically designed to identify and measure the fear avoidance beliefs and behaviors associated with vestibular disorders.
Objective
To translate and culturally adapt the VAAI-9 into Chinese and to investigate its reliability and validity of the Chinese Version.
Methods
The Brislin translation model was strictly followed to conduct cross-cultural adaptation of the VAAI-9, which included translation, back translation, expert consultation, and preliminary investigation, ultimately resulting in the Chinese version of the VAAI-9 (VAAI-9-C). A total of 330 Chinese-speaking patients with dizziness or vestibular disorders were recruited through convenience sampling, and they were asked to complete the baseline questionnaire and the VAAI-9-C. The reliability of the instrument was evaluated through item analysis, internal consistency was measured by Cronbach’s alpha, and test-retest reliability was assessed by the intraclass correlation coefficient (ICC) and the minimal detectable change (MDC95). Content validity was determined by expert evaluation results, including the item-level content validity index (I-CVI) and scale-level content validity index (S-CVI). Structural validity was assessed through exploratory factor analysis (EFA) and confirmatory factor analysis (CFA).
Results
During the cross-cultural adaptation process, minor revisions were made to the content expression to ensure semantic equivalence. The correlation coefficients between each item and the total score of VAAI-9-C ranged from 0.745 to 0.794. Cronbach’s alpha was 0.911 and ICC was 0.886 for the VAAI-9-C total scale. The MDC95 was 8.78 points. The I-CVI for each item of the VAAI-9-C ranged from 0.9 to 1.0, and the S-CVI was 0.98. Exploratory factor analysis revealed three common factors and explained 88% of the total variance. Confirmatory factor analysis indicated that χ2/df = 1.317, incremental fit index (IFI) = 0.995, Tucker-Lewis index (TLI) = 0.992, comparative fit index (CFI) = 0.995, root mean square error of approximation (RMSEA) = 0.038, and standardized root mean square residual (SRMR) = 0.024, demonstrating a good model fit.
Conclusions
The VAAI-9-C demonstrates strong reliability and validity, making it an effective tool for evaluating fear avoidance beliefs and behaviors in the Chinese-speaking population with dizziness.
Introduction
The vestibular system is essential for maintaining postural balance and motor control. However, pathological damage to peripheral or central vestibular structures can lead to vestibular dysfunction, which is characterized by dizziness and various related secondary symptoms. 1 Epidemiological studies indicate that approximately 30% of adults have experienced transient or persistent episodes of dizziness or lightheadedness,2,3 with the prevalence and recurrence closely linked to advancing age. 4 In China, the incidence of dizziness is estimated to be between 5% and 8%, 5 and it continues to rise due to urbanization and changes in lifestyle among the population. This upward trend in dizziness incidence is significant, and its chronic nature, characterized by recurring episodes, severely impacts patients’ quality of life, presenting a pressing public health challenge.
Patients with dizziness frequently present symptoms such as falls and unstable gait, often accompanied by psychological disorders, including anxiety and depression. 6 They are predisposed to developing fear avoidance behavior, characterized by the avoidance of activities associated with dizziness due to a fear that physical movement may trigger dizziness episodes or other adverse outcomes. This behavior can inhibit the vestibular system’s compensatory mechanisms, thereby delaying recovery process.7,8 Recent studies have increasingly highlighted the role of psychological and behavioral factors in patients with dizziness. Kim et al. 9 found that patients with vestibular disorders had significantly higher prevalence rates of anxiety (31.4%) and depression (28.3%) compared to healthy controls (8.3% and 4.7%, respectively), and were more likely to experience functional impairment. Furthermore, fear avoidance beliefs and behaviors have been shown to predict activity limitations and participation restrictions in individuals with vestibular disorders.10,11 However, there are currently limited research tools available in clinical practice to assess fear avoidance behavior and other behavioral and psychological factors in patients with dizziness.
In 2018, Alshebber et al. 12 developed the Vestibular Activities Avoidance Instrument (VAAI), which effectively measures fear avoidance behaviors, as well as anxiety and depression, in patients with dizziness. However, the lengthy items and significant response burden on patients limit its clinical practicality. Consequently, the original version was revised and simplified to create a 9-item version. 10 This version has been culturally validated in the United States 11 and the Netherlands, 13 demonstrating good internal consistency. Van Laer et al. 14 found that participants with vestibular disorders exhibited higher levels of fear avoidance beliefs, perceived disability, anxiety and depression, as well as lower balance confidence, and demonstrated the cross-cultural validity of the VAAI-9. The VAAI-9 not only accurately quantifies the fear avoidance beliefs and behaviors of patients with dizziness but also predicts activity limitations and disability levels after 3 months. However, to date, the VAAI-9 has not been applied or validated in China, a country characterized by a large population and a high prevalence of dizziness.
Consequently, a Chinese version of the VAAI-9 is essential for effectively identifying and measuring the fear avoidance beliefs and behaviors of patients with dizziness concerning specific vestibular activities. This version will facilitate the early identification of patients at high risk of disability and enhance their long-term prognosis. The aim of this study is to culturally adapt and psychometrically validate the Chinese version of the VAAI-9 through a rigorous translation and cross-cultural validation process.
Methods
Participants
This study utilized convenience sampling to recruit participants from the ENT Departments of two tertiary A hospitals (the highest-level hospitals in China’s three-tier healthcare system) in Shandong Province, China. The inclusion criteria: (1) Age greater than 18 years; (2) Native Chinese speakers; (3) Clinically confirmed diagnosis of vertigo according to the “Guidelines for Emergency Diagnosis and Treatment of Vertigo (2021)” 15 ; (4) Clinically stable condition. The exclusion criteria: (1) Use of dizziness-inducing medications within 3 months prior to enrollment; (2) Active malignancies or severe organ dysfunction; (3) Cognitive or linguistic barriers preventing valid questionnaire responses. This study received approval from the relevant ethics committee (Approval Number: R202409020343). Written informed consent was obtained from all participants prior to enrollment.
Sample size
In this study, 30 participants were selected for a questionnaire survey during the pilot phase. In the psychometric evaluation phase, following the principle of having 5 to 10 times the number of samples, 16 with a minimum of 200 for confirmatory factor analysis, 17 and accounting for 10% of invalid questionnaires, a total of 340 questionnaires were distributed for the survey (excluding participants from the pilot phase). Of these, 330 valid responses were retained after eliminating the invalid responses. In accordance with international methodological recommendation standards, the 330 questionnaires were randomly divided into two parts in a 1:2 ratio. Specifically, 110 questionnaires were assigned for exploratory factor analysis, while 220 were designated for confirmatory factor analysis.
Instruments
Baseline questionnaire
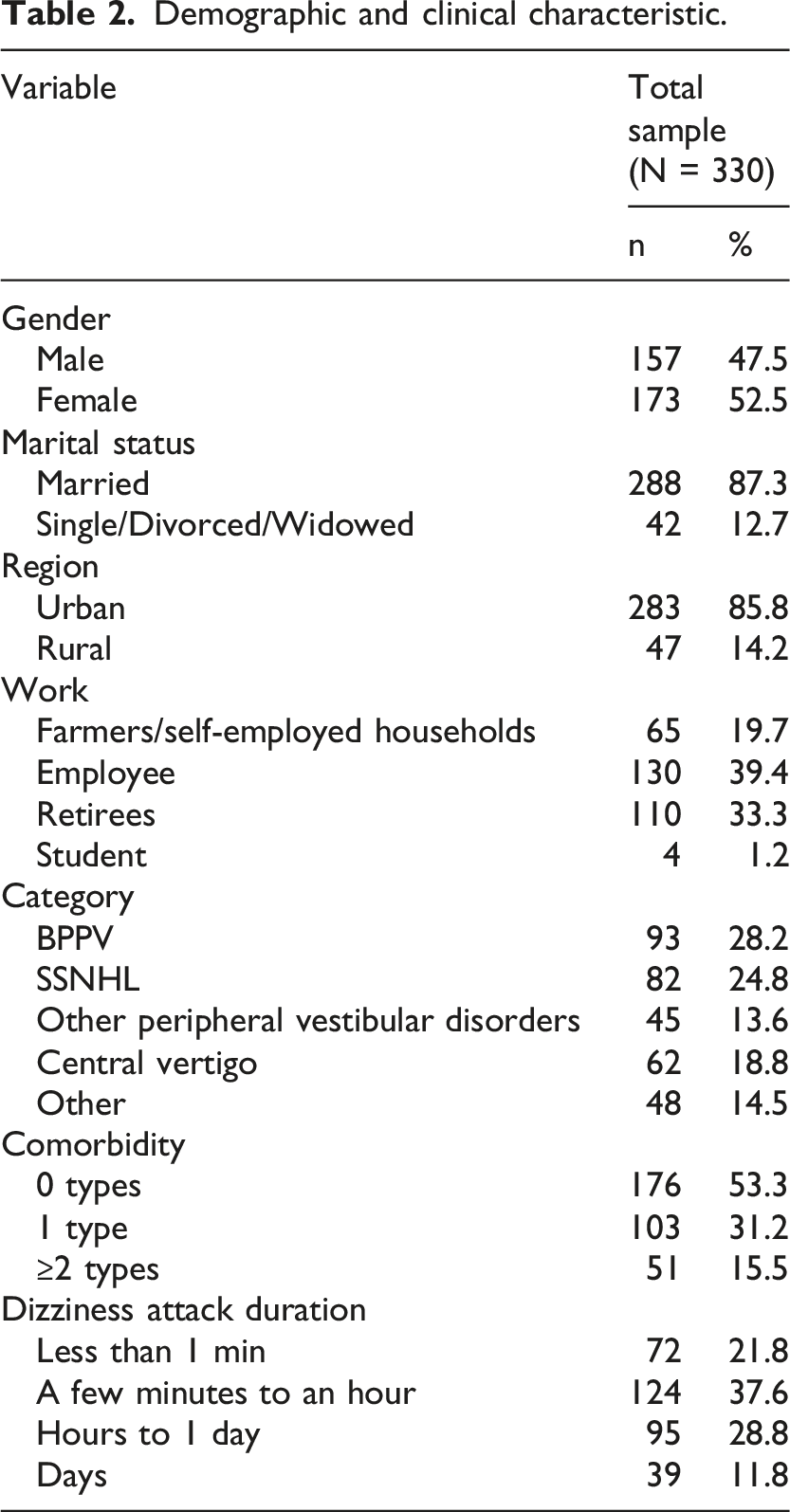
Demographic characteristics including age, gender, marital status, region and work, and clinical characteristics including disease diagnosis, number of comorbidities, and dizziness attack duration.
VAAI-9-C
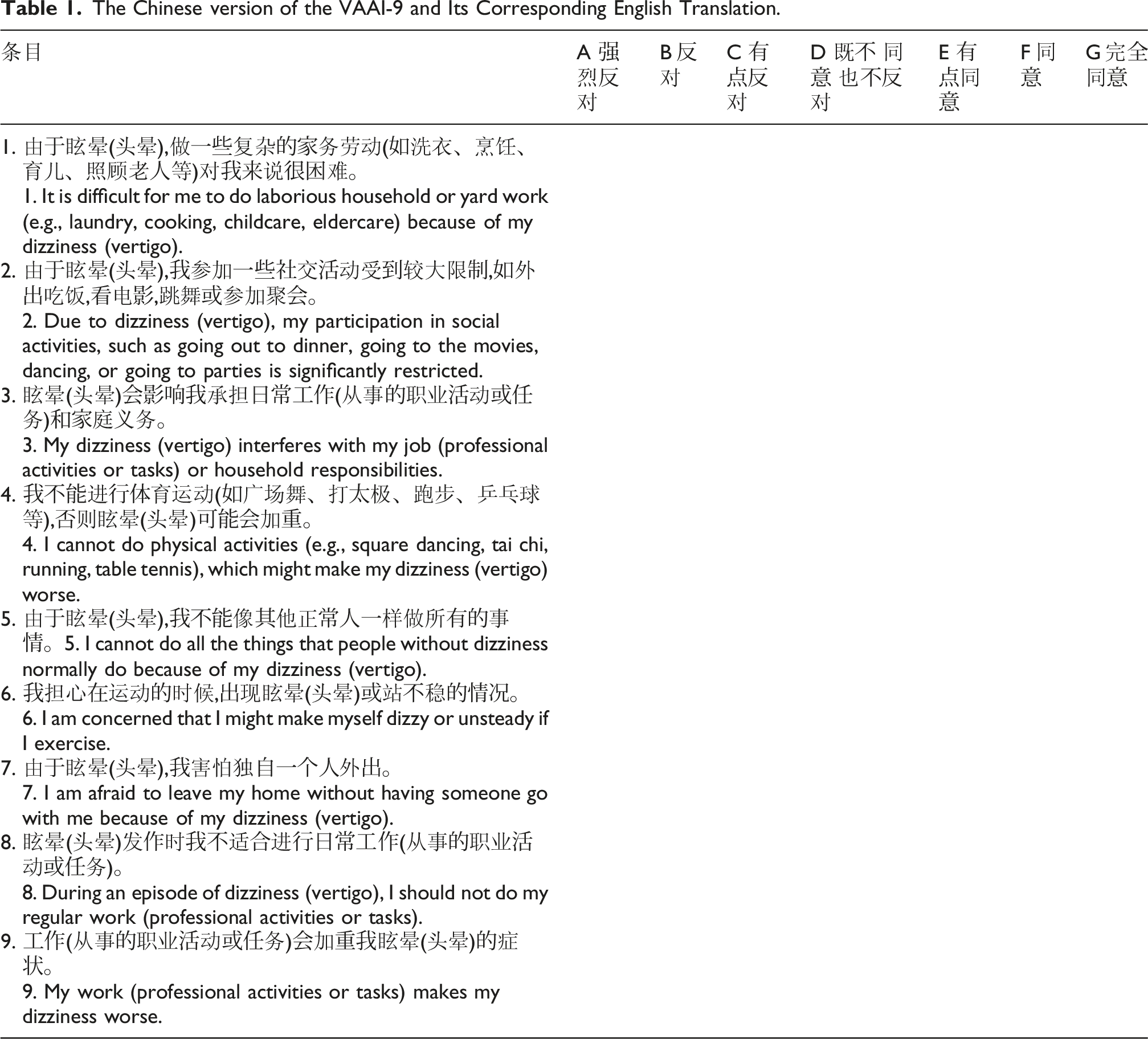
The Chinese version of VAAI-9 consists of 9 items designed to measure fear, avoidance beliefs, behaviors, and their impact on the disability levels of patients with dizziness. 10 The measurement range spans from “strongly disagree” (0 points) to “completely agree” (6 points). The total score is the sum of the scores for each item on the scale, ranging from 0 to 54 with higher scores indicating a greater level of fear and avoidance because of dizziness.
Procedure
This study was conducted in two phases. Phase 1: Translation and cross-cultural adaptation of VAAI-9, March 2024 to August 2024. Phase 2: Psychometric Assessments and Statistical Analysis of VAAI-9-C, September 2024 to August 2025.
Phase 1: Translation and cross-cultural adaptation
The developer was contacted via email to obtain permission to translate and use the VAAI-9. The Chinese version of the VAAI-9 was developed following Brislin’s translation model, 18 with additional refinements based on Beaton et al.’s cross-cultural adaptation guidelines. 19 This phase mainly consisted of three steps: (1) Scale Translation; (2) Expert Committee Review and Cultural Adaptation; and (3) Pilot Pre-testing.
Two bilingual native Chinese translators independently translated the original English version of the VAAI-9 into Chinese. A researcher compared and synthesized these translations to produce a preliminary Chinese version. Then, a linguist proficient in English and an otolaryngologist with a bicultural background served as translators to back-translate the synthesized version into English, without knowledge of the original scale. Another researcher subsequently compared and synthesized the back-translated version with the original scale.
An expert panel, consisting of three otolaryngologists, two clinical psychologists, and five rehabilitation nurses, reviewed the Chinese version of the VAAI-9, evaluating the clarity, relevance, and significance of the scale items. Based on the Chinese social and cultural background, the wording of the items was appropriately adjusted to ensure content, semantic and conceptual equivalence with the original scale.
A pilot study involving 30 participants who were not included in the sample for the psychometric evaluation phase was conducted to assess the comprehensibility and feasibility of the Chinese version of the VAAI-9. Participants completed the questionnaire while providing real-time verbal feedback on item clarity, appropriateness of wording, and overall usability. In response to the feedback received, the panel discussed and revised the final Chinese version of the VAAI-9.
Phase 2: Psychometric properties and statistical analysis
A multicenter cross-sectional study was conducted with 330 participants who completed the baseline questionnaire and the VAAI-9-C. The psychometric properties assessed included item analysis, reliability analysis, and validity analysis. Statistical analyses were conducted using IBM SPSS (version 26.0) and IBM AMOS (version 24.0). Continuous data were expressed as mean ± standard deviation, while categorical data were reported as frequencies. Findings were considered statistically significant when the p-value was less than 0.05.
Item analysis
The critical ratio (CR) method and the correlation coefficient method were employed to screen the items of the Chinese version of the VAAI-9. The critical ratio for each item was calculated by performing an independent samples t-test between a high-scoring group (top 27% by total score) and a low-scoring group (bottom 27%), with the resulting t-value serving as the critical ratio. CR above 3.00, Pearson correlation coefficient (r) above 0.40, and statistical significance for both metrics indicate that the scale items exhibit good discriminative validity and item-total consistency. 20 Items that met all specified criteria (CR >3.00, r > 0.40, p < 0.05) were retained, with non-compliant items subject to Delphi-based modification or removal.
Reliability analysis
Reliability analysis was conducted to assess the stability and consistency of the scale, which included internal consistency and test-retest reliability. Cronbach’s alpha coefficient above 0.80 indicates high internal consistency, while a value between 0.60 and 0.70 is considered acceptable. 21 At the same time, the “Cronbach’s Alpha if Item Deleted” was calculated to observe whether any items would reduce the overall reliability. To assess test-retest reliability, 30 randomly selected participants completed the VAAI-9-C again after a 2-week interval. This interval was chosen to minimize recall bias while maintaining the assumption of clinical stability, in accordance with methodological recommendations from previous studies. 22 The test-retest reliability was assessed using the intraclass correlation coefficient (ICC). The ICC value above 0.75 indicates good test-retest reliability. 23 The Minimal Detectable Change (MDC95) was calculated to determine the smallest change beyond measurement error, using the formula: MDC95 = 1.96 × SD × √[2×(1−ICC)], where SD is the standard deviation of the baseline scores.
Validity analysis
Validity analysis was conducted to assess the validity of the scale, which included content validity and structural validity. The expert panel involved in the cross-cultural adaptation was invited to rate the relevance of the items using a four-point Likert scale. The content validity of the scale was considered satisfactory when the I-CVI ≥ 0.78 and the S-CVI ≥ 0.90. 24
The suitability of the data for factor analysis was initially assessed using the Kaiser–Meyer–Olkin (KMO) measure and Bartlett’s test of sphericity. 25 Once adequate factorability was confirmed (KMO > 0.60 and Bartlett’s test significant at p < 0.05), EFA was conducted on a randomly selected subsample of 110 participants. The underlying factor structure of the VAAI-9-C was explored using principal component analysis (PCA) with varimax rotation. PCA was employed to reduce dimensionality while retaining maximal variance, and varimax rotation was applied to simplify factor loadings and enhance interpretability. Factors with eigenvalues greater than 1 were retained. Items with factor loadings < 0.40 or exhibiting cross-loadings (defined as the difference between primary and secondary loadings being less than 0.20) were sequentially removed. 21 The final factor analysis demonstrated strong structural validity, as indicated by a cumulative variance explained exceeding 50% and all retained items exhibiting primary factor loadings greater than 0.70.
CFA was conducted on the remaining 220 participants using maximum likelihood estimation. The model demonstrated an acceptable fit based on the following criteria: χ2/df ratio between 1 and 3, incremental fit index (IFI) ≥ 0.90, Tucker-Lewis index (TLI) ≥ 0.90, comparative fit index (CFI) ≥ 0.90, root mean square error of approximation (RMSEA) ≤ 0.08, and standardized root mean square residual (SRMR) ≤ 0.08. 26
Results
Content validation
The Chinese version of the VAAI-9 and Its Corresponding English Translation.
Participant characteristics
Demographic and clinical characteristic.
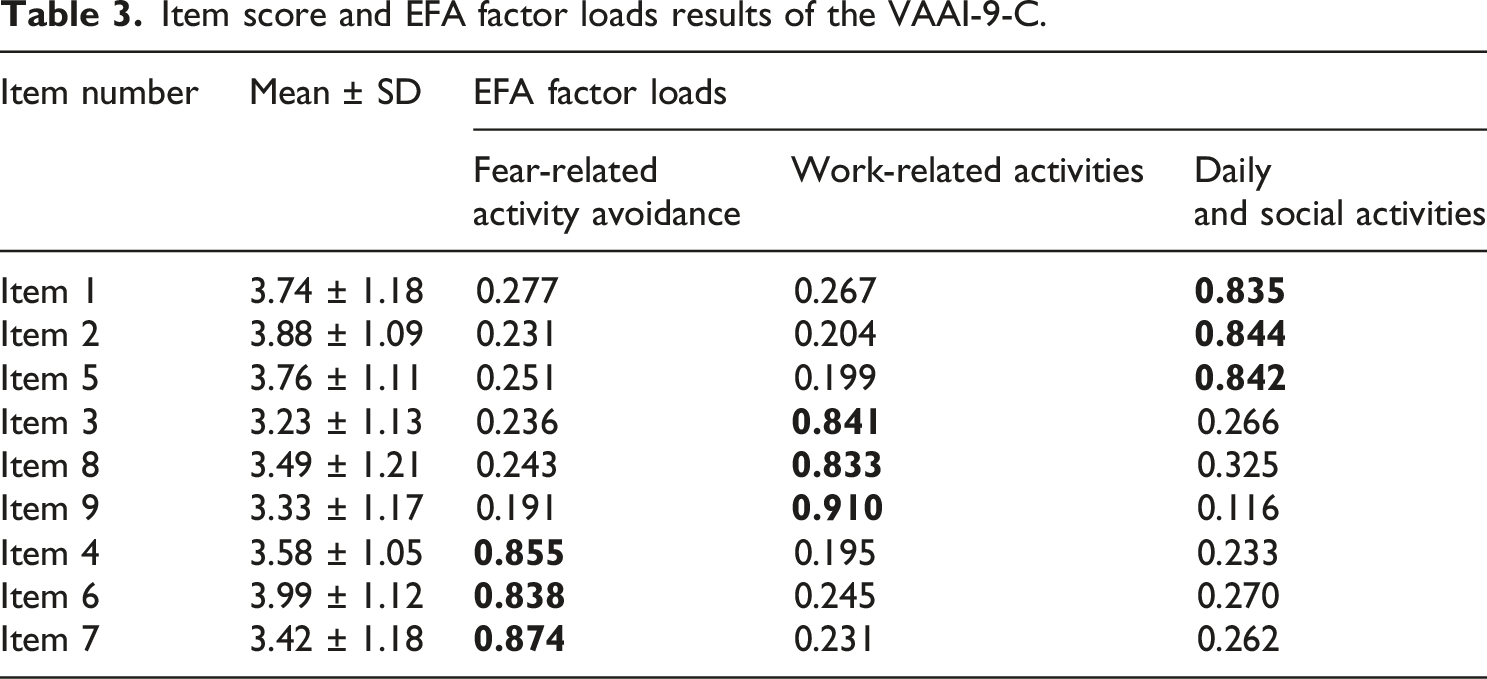
Item score and EFA factor loads results of the VAAI-9-C.
Item analysis
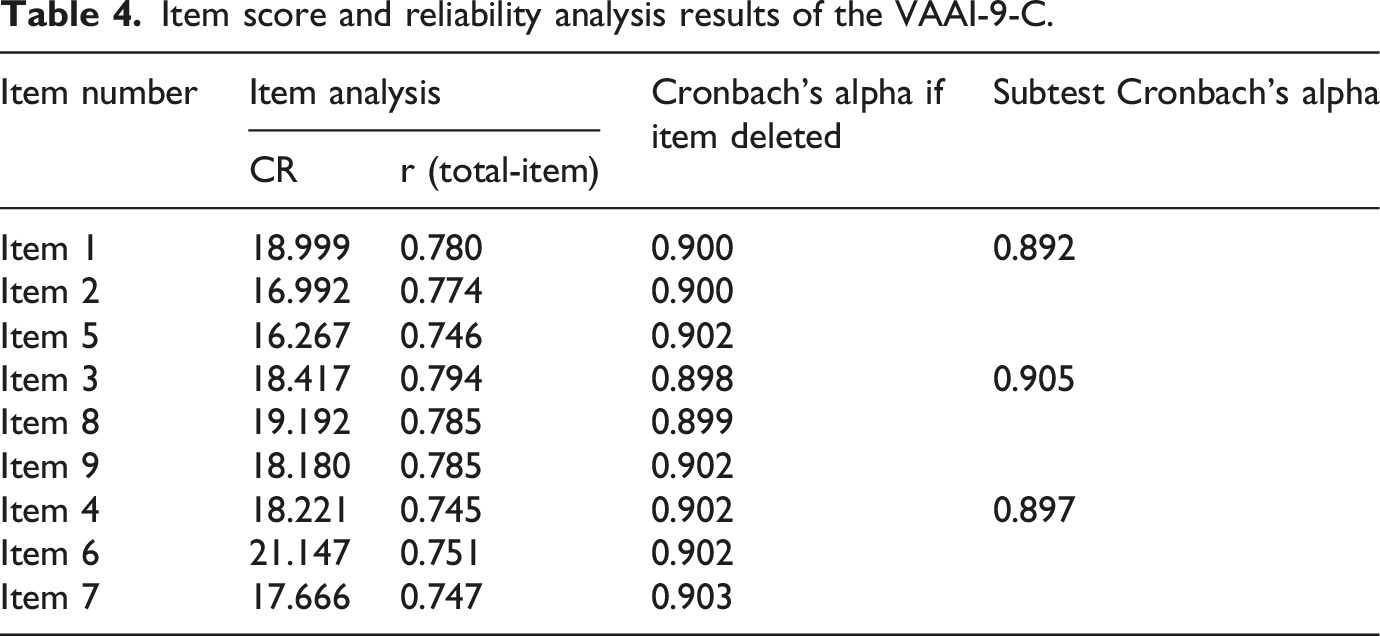
Item score and reliability analysis results of the VAAI-9-C.
Reliability analysis
The Cronbach’s α coefficient for the total scale of the VAAI-9-C was 0.911, indicating that the scale has good internal consistency. The Cronbach’s α coefficients for the three factors—Daily and Social Activities, Work-related Activities, and Fear-related Activity Avoidance—were 0.892, 0.905, and 0.897, respectively. The detailed statistical results are shown in Table 4. The removal of any item did not significantly increase the Cronbach’s α coefficient, indicating that there are no redundant items in the scale. The ICC was 0.886 (p < 0.01), indicating excellent test-retest reliability. Based on the SD (9.38) and the ICC, the MDC95 for the VAAI-9-C was calculated as 8.78 points, representing the minimum score change required to indicate a true change in fear avoidance beliefs beyond measurement error.
Validity analysis
The Chinese VAAI-9-C demonstrated excellent content validity, with I-CVIs ranging from 0.90 to 1.00 and the S-CVI of 0.98, as evaluated by an expert panel.
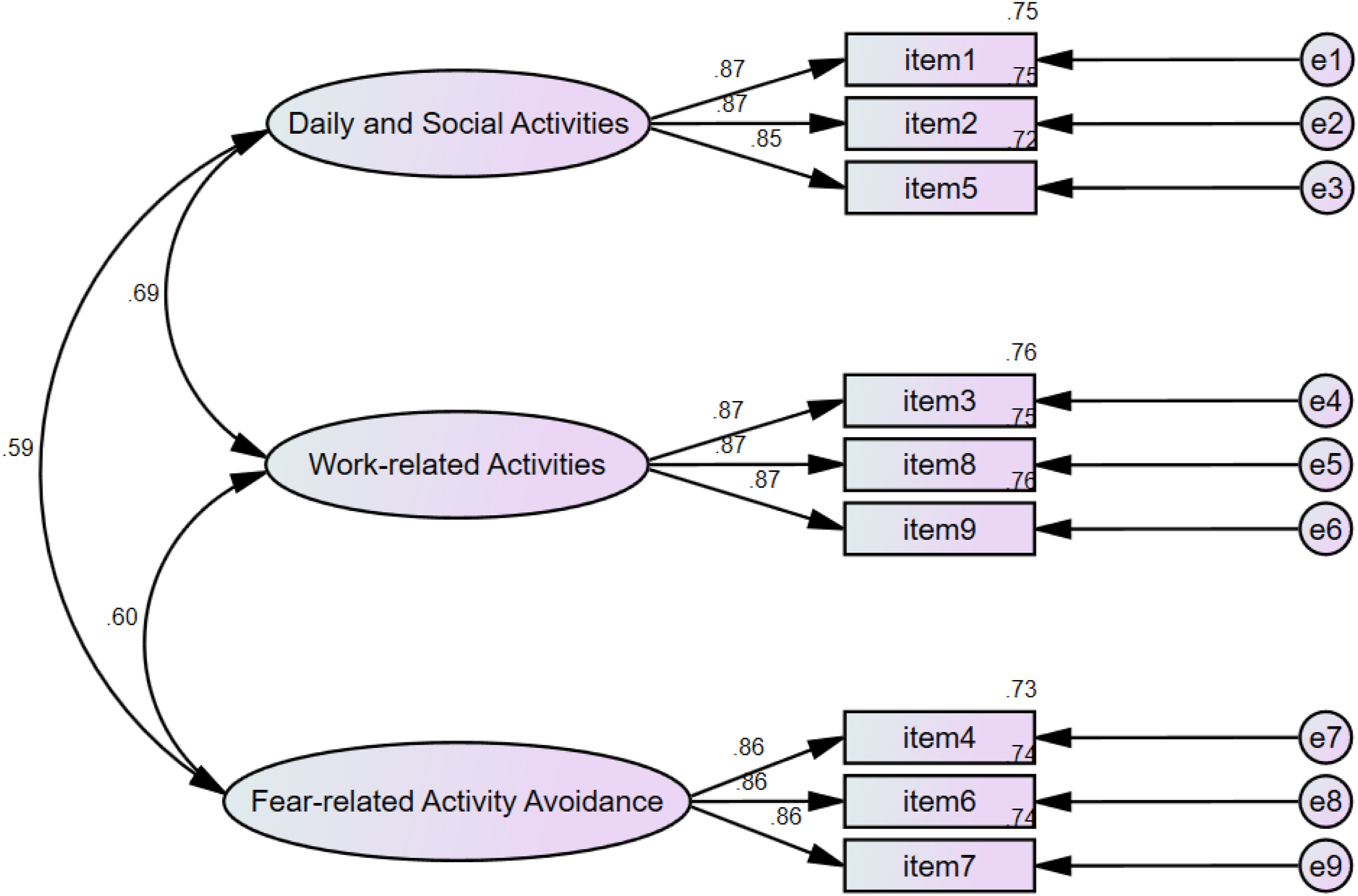
The KMO measure of sampling adequacy was 0.860 (>0.60), and Bartlett’s test of sphericity was significant (χ2 = 729.036, df = 36, p < 0.001), demonstrating adequate sample suitability. Compared with the original scale, principal component analysis in this study extracted three common factors with eigenvalues >1, consistent with the scree plot inflection point (Figure 1). Taking into account the conceptual framework of the VAAI-9 and the empirical loading pattern observed in the present sample, the three factors were retained and labeled as “Daily and Social Activities,” “Work-related Activities,” and “Fear-related Activity Avoidance.” The factor loadings of each item after orthogonal rotation are presented in Table 3. The cumulative variance contribution rate was 84.219% (>50%). CFA using maximum likelihood estimation (n = 220) yielded a strong model fit: χ2 = 31.604 (df = 24), χ2/df = 1.317, IFI = 0.995, TLI = 0.992, CFI = 0.995, RMSEA = 0.038, and SRMR = 0.024, all meeting the recommended thresholds, the path diagram is shown in Figure 2. Scree plot for exploratory factor analysis of the VAAI-9-C. Path diagram of the VAAI-9-C.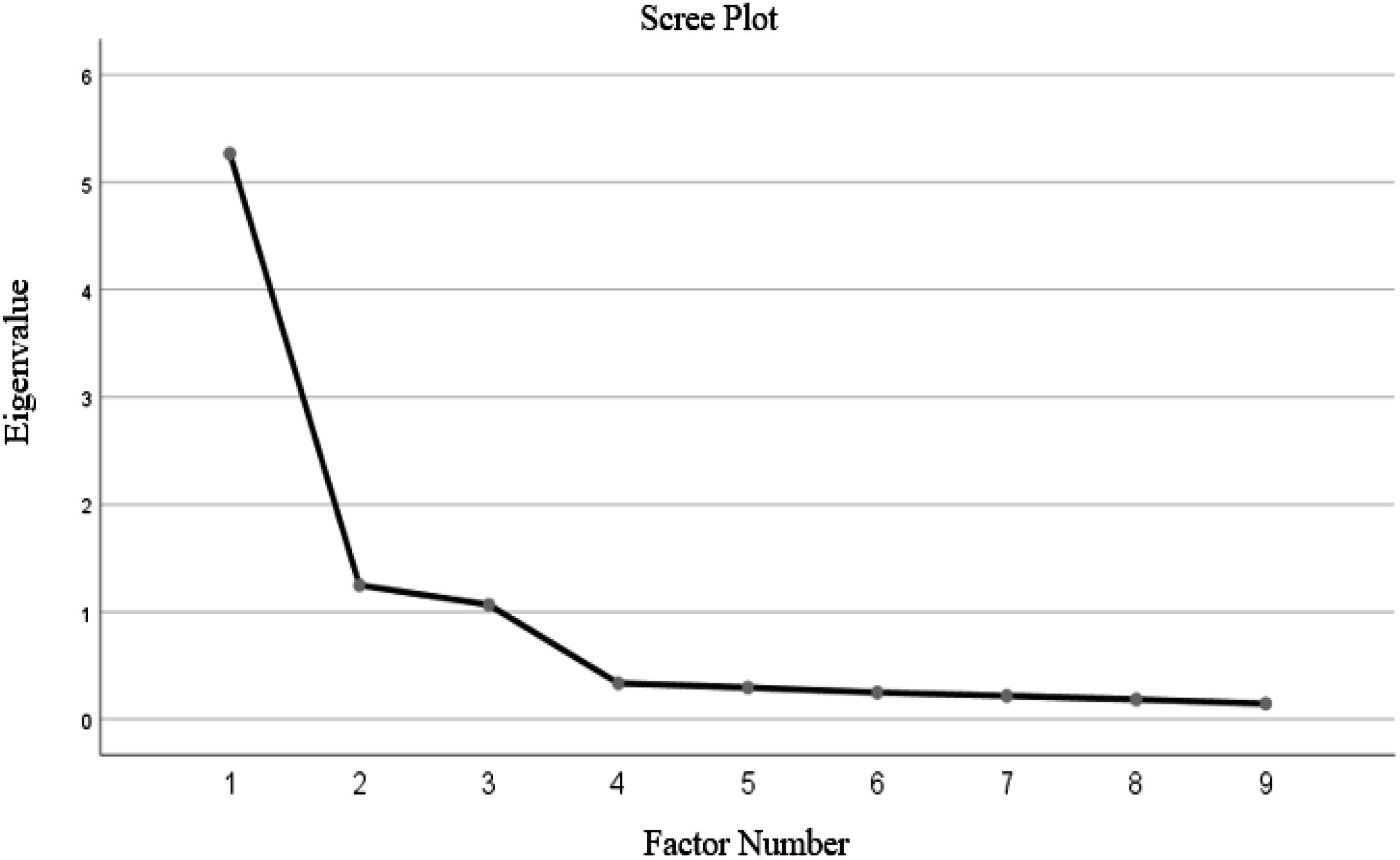
Discussion
Fear avoidance behavior is increasingly acknowledged as a pivotal factor contributing to activity limitations and restricted participation in patients with vestibular disorders or dizziness. This study involved the successful translation of the original English version of the VAAI-9 into Chinese. To ensure the scale’s validity across various languages and cultural contexts, Items 1, 2, 4, and 8 were culturally adapted during the cross-cultural refinement phase to align with the local Chinese context. A comprehensive psychometric evaluation was subsequently conducted within a population of patients experiencing dizziness in eastern China. The findings indicate that the VAAI-9-C features clear and comprehensible items with sound psychometric properties, establishing it as a reliable and valid instrument for assessing fear avoidance beliefs and behaviors among Chinese-speaking patients with dizziness.
Item analysis demonstrated good discriminative ability for each VAAI-9-C item, effectively distinguishing between individuals with different levels of fear avoidance beliefs. Regarding reliability, the overall Cronbach’s α of the VAAI-9-C was 0.911, comparable to the 0.92 reported for the original English version 11 and superior to the 0.846 for the Dutch version, 13 demonstrating that the scale exhibits excellent internal consistency across various language and cultural contexts. Furthermore, Cronbach’s α coefficients for the three factors yielded values of 0.892, 0.905, and 0.897, indicating that each factor provides balanced and precise measurement performance. The VAAI-9-C showed excellent test-retest reliability, with an ICC of 0.886, closely aligning with the 0.92 reported for the Dutch version. 13 The MDC95 was calculated as 8.78 points, nearly identical to the 8.9 points reported by Vereeck et al., 13 supporting cross-cultural consistency in detecting true clinical change. Methodologically, the present study employed a 2-week retest interval. This design effectively mitigated potential short-term memory effects and further substantiated the scale’s temporal stability. 20 In contrast, the Dutch study utilized a substantially shorter interval (mean 1.6 days), which may partly account for the minor discrepancy in MDC values. VAAI-9-C also demonstrated satisfactory content and structural validity, reflecting the intended constructs and maintaining high semantic, conceptual, and content equivalence with the original scale. The KMO measure in this study was 0.860 (>0.8), slightly lower than the 0.95 reported in the original study, which may be attributable to differences in sample characteristics and cultural adaptation of certain items. Nevertheless, the KMO value remained within an acceptable range, supporting the reliability and appropriateness of the data for factor analysis.
Importantly, this study extracted a total of three common factors through exploratory factor analysis, which differs from the unidimensional structure of the original scale. The three factors were labeled Daily and Social Activities, Work-related Activities, and Fear-related Activity Avoidance. The first factor included items related to household chores, social activities, and general daily functioning. Although these items may represent conceptually distinct domains, pilot cognitive interviews indicated that participants generally perceived them as related types of dizziness-related activity limitations, providing qualitative support for the coherence of this empirically derived grouping. Therefore, this factor should be interpreted as reflecting general restrictions in daily life rather than implying complete equivalence between household and social activities. The second factor consisted of items related to work or occupational responsibilities, representing a distinct aspect of functional limitation. The third factor included items related to physical activity, fear of becoming dizzy or unsteady, and leaving home alone. Activities such as square dancing and tai chi may involve multiple aspects beyond exercise, including social interaction. Therefore, this factor was labeled “Fear-related Activity Avoidance” to reflect multiple possible underlying mechanisms, including fear of symptom exacerbation, imbalance concerns, reduced confidence, or social concerns.
This structural difference may be explained by several factors. First, different factor structures may emerge in specific cultural and linguistic contexts, possibly reflecting variation in how individuals perceive and categorize dizziness-related experiences. Then, Van Laer et al. 14 validated the convergent validity of a unidimensional model in a cross-cultural sample but did not rule out the possibility of multidimensionality in certain populations. To examine the adequacy of the three-factor solution and to rule out over-extraction, an additional EFA was conducted forcing extraction of a single factor. The single-factor model accounted for 58.528% of the total variance, which was substantially lower than the 84.219% explained by the three-factor solution. This substantial increase in explained variance indicates that the three-factor solution captures the underlying structure of the VAAI-9-C more comprehensively and is scientifically justified.
Based on the aforementioned research evidence, it is recommended that the VAAI-9-C be utilized as a standardized assessment tool for evaluating fear avoidance beliefs and behaviors in patients with dizziness in China. Research11,12,27 has demonstrated that dizziness not only impacts patients’ daily activities and quality of life but, as the condition progresses, may also result in severe physical impairments and even disability. These adverse outcomes are often closely related to various psychological and behavioral factors, particularly the significant correlation between fear avoidance levels and the severity of dizziness symptoms. 14 Additionally, psychological factors such as anxiety and depression can further influence disease progression through psychosomatic mechanisms, as documented in patients with vestibular disorders. 9 Clinically, the VAAI-9-C facilitates quantitative assessment through three factors, assisting healthcare professionals in effectively measuring fear avoidance levels in patients with dizziness regarding specific vestibular activities. It enables the early identification of patients at high risk for disability and promotes the development of personalized intervention plans to improve long-term patient outcomes. Additionally, the items in the VAAI-9-C are concise and clear, making them easy to understand while accurately quantifying fear avoidance beliefs and behaviors without increasing patients’ response burden, thereby demonstrating good reliability and practicality. In summary, these features position the VAAI-9-C as an important tool for linking assessment, diagnosis, and intervention, with the potential to optimize comprehensive management of patients with dizziness.
Limitations
This study has several limitations. In terms of sample representativeness, the study only included ENT patients from two tertiary A hospitals in Shandong Province due to objective constraints, limiting the ability of the sample to adequately reflect the characteristics of patients across different regions and tiers of hospitals in China. Additionally, the included subjects have a relatively high proportion of urban population, resulting in insufficient representation of rural patients. Furthermore, information about the time from dizziness onset was not fully collected, which may limit the generalizability of the findings across patients with different disease durations or chronicity. Regarding psychometric properties, the limited study duration prevented the conduct of responsiveness testing of the VAAI-9-C. To address these limitations, future research should conduct multicenter collaborative studies nationwide, incorporating healthcare institutions of various tiers and employing a stratified sampling strategy based on the latest census data to ensure a scientifically appropriate urban-rural ratio. Furthermore, longitudinal cohort studies should be designed to refine responsiveness test, evaluating the sensitivity of the VAAI-9-C to vestibular rehabilitation interventions.
Another limitation is that the present study directly validated the VAAI-C-9 without concurrently administering the original 81-item VAAI. Thus, the structural association between the 81-item and 9-item versions was not directly examined in the current Chinese-speaking sample. Vereeck et al. 13 validated the Dutch version of the VAAI-9 alongside the VAAI-81 and reported a high correlation between the two versions (ICC = 0.95 for VAAI-81 and ICC = 0.92 for VAAI-9), supporting that the 9-item short form can represent the broader construct measured by the 81-item version in a non-English context. However, whether the VAAI-9-C fully captures the construct coverage of the VAAI-81-C in Chinese patients with dizziness remains to be confirmed. Future studies are encouraged to administer both the 81-item and 9-item versions simultaneously in a subsample (e.g., n = 100–150), and to report correlation coefficients and agreement (e.g., ICC or Bland–Altman analysis) to clarify the extent to which the short form generalizes the structure of the original scale in the Chinese context.
Conclusions
The VAAI-9-C demonstrates strong reliability and validity, making it an effective tool for evaluating fear avoidance beliefs and behaviors in Chinese-speaking population with dizziness. It provides healthcare professionals with a basis for accurately identifying patients’ fear avoidance behaviors and developing personalized intervention strategies.
Footnotes
Acknowledgments section
We are profoundly grateful to Dr Dunlap for authorizing the translation and clinical use of the VAAI-9. Deep appreciation goes to the expert panel members for their professional guidance and constructive suggestions during the cross-cultural adaptation process of the scale. Special recognition is given to the nursing teams of the ENT Departments for their invaluable support and coordination in clinical data collection.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and received approval from the Institutional Review Board of Shandong First Medical University (Approval No. R202409020343).
Consent to participate
Written informed consent was obtained from all participants included in the study. Participants were advised of their right to withdraw at any time without consequences to their medical care.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Research Fund of Shandong Provincial Research Hospital Association (Grant No. 2022005).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during this study are not publicly available due to patient confidentiality protections mandated by China’s Personal Information Protection Law. However, they may be obtained from the corresponding author upon reasonable request, in accordance with institutional data sharing protocols.