
Abstract
BACKGROUND:
Suppression Head Impulse Paradigm (SHIMP), a novel variant of the Head Impulse Test has been introduced. At the same time, the Head Impulse Test was renamed to the Head Impulse Paradigm (HIMP). Contrary to HIMP saccades, SHIMP saccades are a sign of vestibular function.
OBJECTIVE:
1) To compare SHIMP and HIMP feasibility, vestibular-ocular reflex (VOR) gain value and the saccadic pattern in healthy adolescents. 2) To compare SHIMP and HIMP feasibility in the hands of an experienced and an inexperienced HIMP examiner.
METHOD:
A total of 29 adolescents from Skåde Municipal School, Denmark were tested with HIMP and then with SHIMP.
RESULTS:
Neither covert nor overt saccades were observed in the HIMP, whereas SHIMP saccades were observed in all SHIMP reports. SHIMP gain values were statistically lower than HIMP gain values. A statistically significant difference was observed between the two examiners’ right SHIMP gain values, but not for the left SHIMP gain values or the HIMP gain values.
CONCLUSIONS:
We found that HIMP and SHIMP tests are feasible in healthy adolescents for experienced as well as inexperienced examiners. However, one must be aware of potential pitfalls in the execution and interpretation of both tests. This is a well-known fact for the HIMP test, but additional considerations are needed to obtain reliable results from the SHIMP test.
Introduction
Vertigo and symptoms of dizziness in children and adolescents are not an uncommon phenomenon, but epidemiological studies in this group are limited. A recent study reported a prevalence of dizziness and vestibular problems of 5.3% in children and adolescents [7].
The oto-neurological spectrum of differential diagnoses in children and adolescents with dizziness differs from that of adults. Even so, it is important to efficiently reach a definitive diagnosis in order to provide appropriate therapeutic management and avoid that the condition becomes chronic.
Diagnostic tests in children and adolescents have traditionally consisted of rotary-chair and caloric testing, which for some children have proven difficult to perform [5]. The newer video Head Impulse Test (vHIT) has gained acceptance worldwide as a fast and reliable test for evaluating the vestibular-ocular reflex (VOR) in adults [4]. Video goggles are used in the vHIT to accurately monitor head and eye movements in order to calculate a VOR gain value and visualise covert and overt catch-up saccades due to a deficient VOR. Recently, the vHIT has also been recommended as an acceptable and effective test in children and adolescents [5, 15].
In 2016, a novel variant of the Head Impulse Test, coined the Suppression Head Impulse Paradigm (SHIMP) was developed by Halmagyi and Curthoys’ research group. At the same time, the Head Impulse Test was renamed the Head Impulse Paradigm (HIMP) [6, 14]. When performing SHIMP, the test subject is asked to focus on a laser dot instead of a fixed point on the wall in front of the person being tested. The laser dot on the wall is projected from the video goggles and as a consequence moves with the imposed head movement, the head impulse. The VOR in healthy subjects causes the eyes to rotate in the opposite direction of an applied fast, brief and unpredictable head impulse and thereby the eyes are driven off the target (the laser dot). In order to reacquire the target, a corrective movement, an anticompensatory SHIMP saccade, is seen at the end of the head impulse. SHIMP gain value may prove to be more reliable since it is not distorted by the presence of covert saccades, and the SHIMP saccades offer additional important information because they are a sign of vestibular function [16].
This study had two aims. The first was to compare SHIMP and HIMP feasibility, VOR gain value and the saccadic pattern in a group of healthy adolescents. The second was to compare the feasibility of the SHIMP and HIMP testing using a commercially available system in the hands of an experienced and an inexperienced HIMP examiner.
Methods
Participants
The study population consisted of 33 pupils (27 boys) aged 13–16 years from Skåde municipal primary and lower secondary school, Denmark. All pupils were attending an 8-week voluntary science class concerning the human balance system offered by the school in collaboration with the Department of Clinical Medicine, Aarhus University. During the 8 weeks, the participants underwent several tests for assessment of balance, including the HIMP and the SHIMP, presented in this paper.
All participants were considered healthy with no previous medical history regarding vestibular disorders and with presumed normally functioning middle and inner ear and age-appropriate verbal IQ. There were no exclusion criteria. All participants were tested in February 2017.
Written consent was obtained from all participants and their parents. The study was conducted in concordance with the Declaration of Helsinki. The results of the study are reported in agreement with the STROBE statement [17].
The head impulse paradigm and the suppression head impulse paradigm
The vestibular function of the horizontal semicircular canal was measured using video goggles (ICS Impulse, Otometrics, Denmark). One experienced and one inexperienced HIMP examiner carried out the tests. The experienced HIMP examiner had previously performed more than 4,500 individual HIMP examinations. Prior to the collection of data, both examiners were instructed in how to carry out the HIMP and SHIMP by an Otometrics representative.
Testing procedure
The participant was seated in a normal chair placed one metre from a wall. The video goggles were put on and the strap pulled tight to minimize any horizontal slippage. Prior to calibrating the goggles, the examiner made sure that the pupil was in the region of interest (ROI) on the screen. Calibration was done according the ISC Impulse software.
All participants were tested with HIMP prior to SHIMP. During HIMP, a dot was placed on the wall in front of the participant in his or her line of sight. The participant was asked to focus on the dot during the test. Brief and unpredictable head impulses were imposed manually to each side to stimulate the horizontal semicircular canals, taking care not to touch the strap from the frenzel and to avoid bouncing of the head at the end of an impulse. On average, 15 impulses were collected for each side.
Immediately after the HIMP test was finished, the SHIMP test was carried out. The dot on the wall was removed, and instead the participant was asked to focus on the red laser dot that was projected on the wall from the goggles. As during the HIMP test, brief and unpredictable head impulses were imposed to each side. On average, ten impulses were collected for each side.
Evaluation of results
After the data acquisition, all individual tests were reviewed for erroneous eye movement measurements by the two examiners. Erroneous measurements were removed manually from the test results [9]. This also included what has previously been described as early saccades in SHIMP [12]. Test results with 5 or fewer remaining impulses were also excluded from the study. The gain value for both HIMP and SHIMP was calculated as the area under the curve, from the beginning of the head impulse to the head velocity again reached 0°/s. The gain values reported by the system were used in the analysis. The system also reported mean peak-head velocity.
Analysis of data
The mean gain value between the examiners and between the right and left horizontal semicircular canal was compared using non-paired t-test. A paired t-test was performed to compare the HIMP and SHIMP gain value. All HIMP and SHIMP data followed a normal distribution assessed using histograms and qq-plots. The agreement between HIMP and SHIMP gain value was assessed using Bland-Altman plots [3].
Results
In total, 33 adolescents were tested of whom four were excluded due to an insufficient number of impulses remaining after the evaluation process. Of the 29 remaining participants, 18 adolescents with a mean age of 14.1 years (range 13.0–15.3 years) were tested by the inexperienced tester, and 11 adolescents with a mean age of 15.0 years (range: 14.0–16.2 years) were tested by the experienced examiner.
All adolescents had a normal vestibular function according to both their HIMP and SHIMP results [10].
HIMP
The mean gain value for the inexperienced examiner was 1.06 (95% confidence interval (CI): 1.02–1.09) for the right side and 0.97 (95% CI: 0.94–1.01) for the left side. The mean gain values for the experienced examiner were 1.03 (95% CI: 0.99–1.07) for the right side and 0.95 (95% CI: 0.91–0.99) for the left side. See Fig. 1.
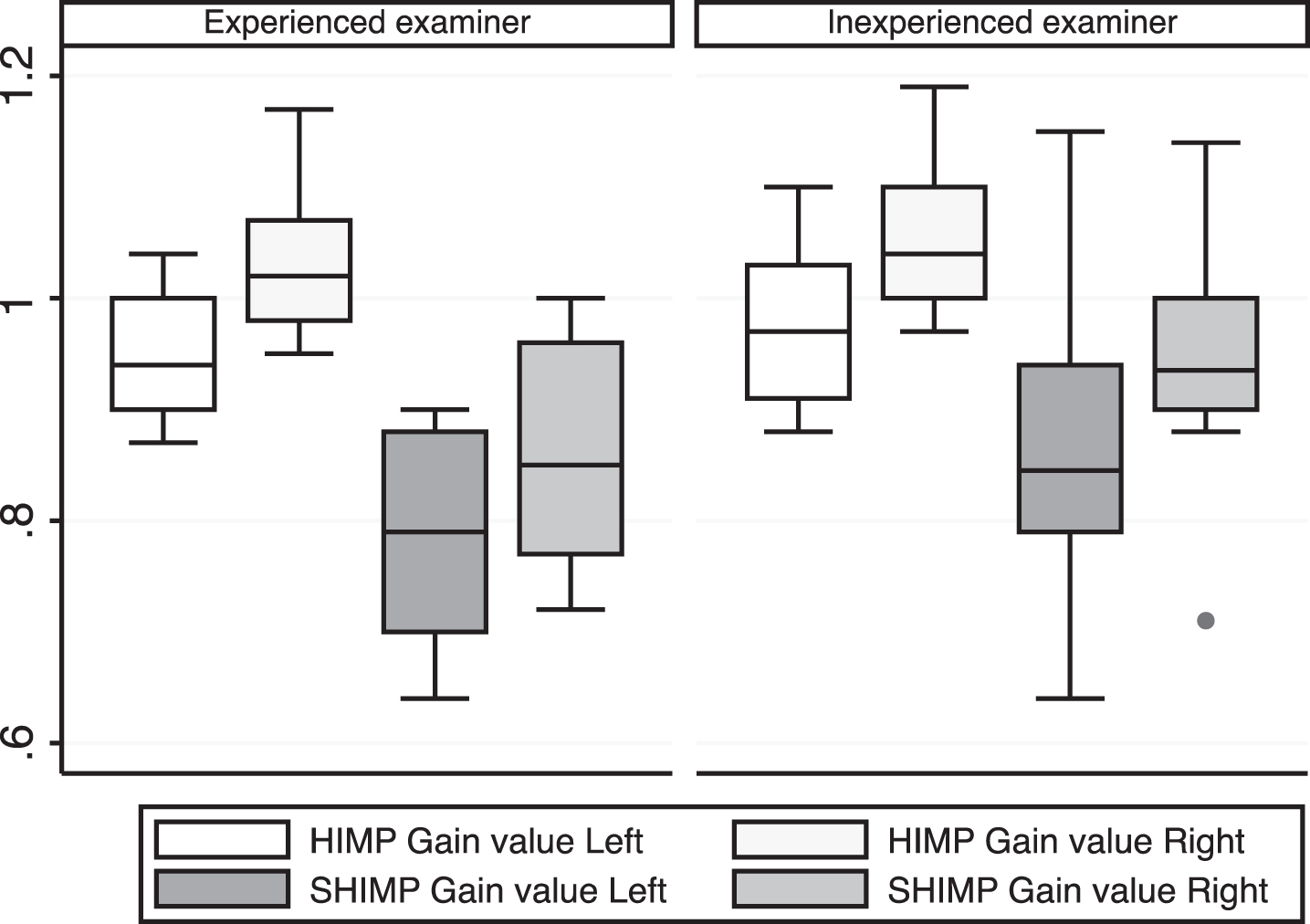
HIMP and SHIMP gain-values. Box plots of left and right side HIMP and SHIMP gain values for both the experienced and inexperienced examiner, with the box representing the quartiles of the distributions, and the whiskers extending to the rest of the distributions with the exception of one outlier value.
We observed a statistically significant difference between the left and right side for both the experienced and the inexperienced examiner (p < 0.05). We observed no statistically significant difference in the mean gain values between the two examiners.
No covert or overt saccades were observed in any of the HIMP results. See Fig. 2 for a typical report of a HIMP test. The mean peak head velocity for the right and left side were 154 (min–max: 141–204°/s) and 162°/s (min–max: 136–178°/s), respectively, for the inexperienced examiner and 190°/s (min–max: 156–204°/s) and 184°/s (min–max: 166–226°/s), respectively, for the experienced examiner.
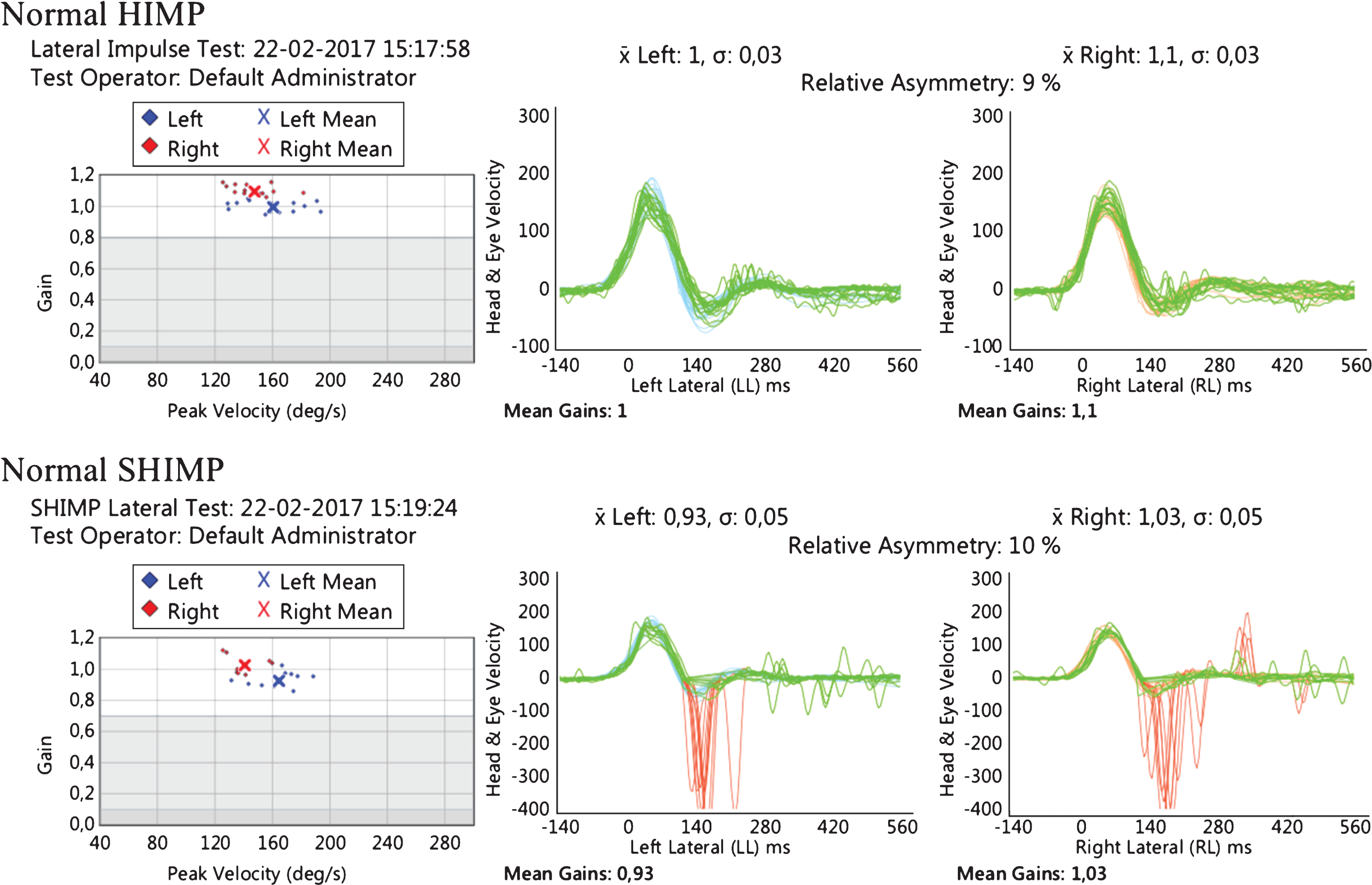
Example of HIMP and SHIMP results. A normal HIMP and SHIMP report.
The mean gain value was 0.95 (95% CI: 0.90–1.00) and 0.87 (95% CI: 0.80–0.94) for the right and left side, respectively, for the inexperienced examiner, and 0.86 (95% CI: 0.79–0.93) and 0.78 (95% CI: 0.72–0.84), respectively, for the experienced examiner (Fig. 1). We observed a statistically significant difference between the left and right side for both the experienced and the inexperienced examiner.
On the right side, the gain values were significantly different (p < 0.05) between the two examiners, whereas no significant difference was seen on the left side.
A large SHIMP saccade was observed at the end of the head impulse in all the reports (Fig. 2).
The mean peak head velocity for the inexperienced examiner was 155°/s (min-max: 136–188°/s) for the left side and 147°/s (min-max: 134–177°/s) for the right side.
For the experienced examiner, the mean peak velocity was 166°/s (min-max: 143–209°/s) for the left side and 180°/s (min-max: 150–204°/s) for the right side.
Differences and average gain values from HIMP and SHIMP are displayed in a Bland-Altman plot (Fig. 3).
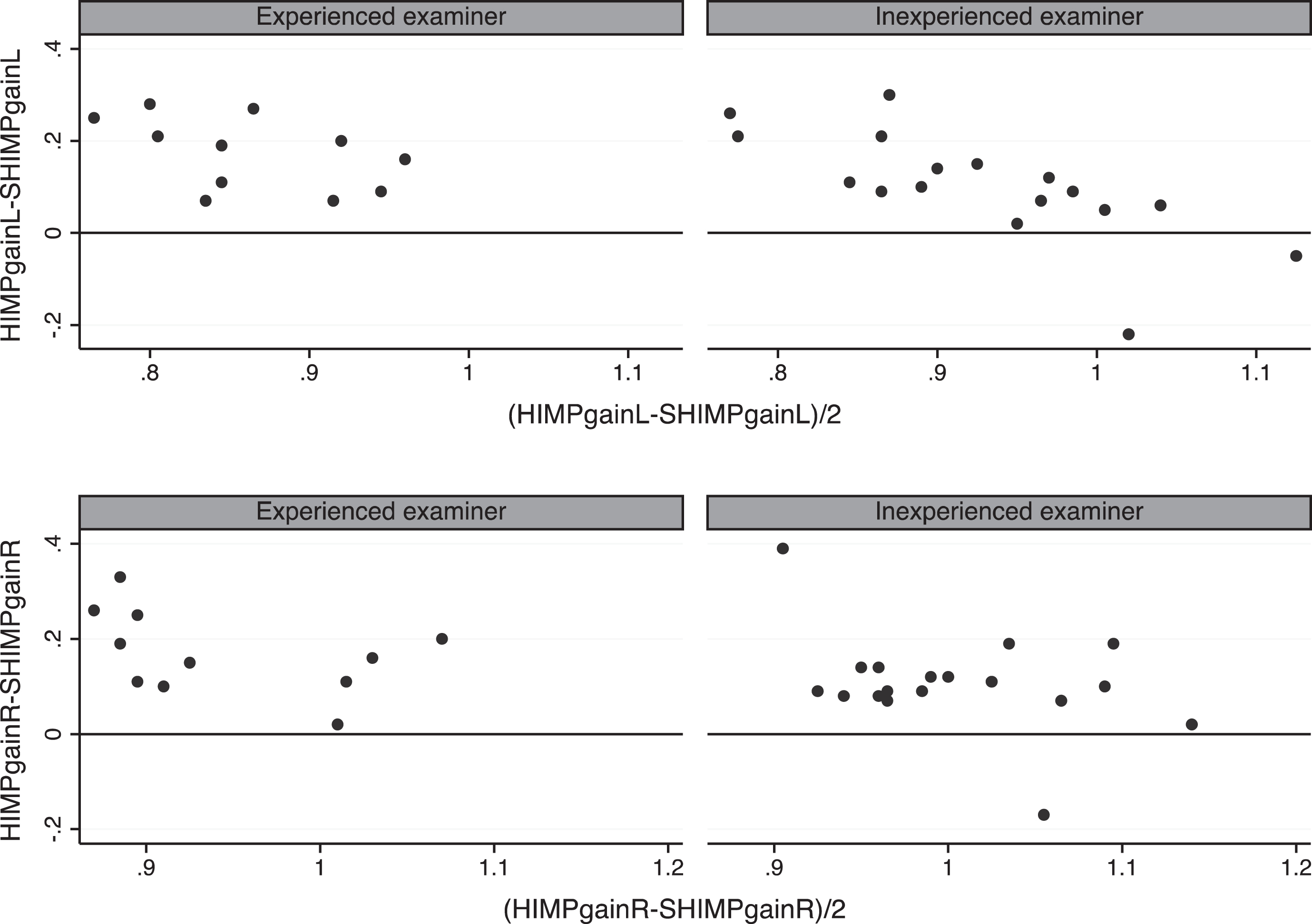
Bland-Altman plot showing agreement between HIMP and SHIMP gain-values. Bland-Altman plots showing the agreement between HIMP and SHIMP gain values for the left (upper charts) and right (lower charts) side for both the experienced and inexperienced examiner. The plots show the difference against the average for each HIMP and SHIMP gain value.
The present study found the HIMP and SHIMP tests to be feasible in adolescents. No covert or overt saccades were found in the HIMP, and all subjects performed a SHIMP saccade in the SHIMP test. Left gain values were lower than right gain values in both HIMP and SHIMP testing gain value. The SHIMP gain values were statistically lower than the HIMP gain values. We observed no statistically significant difference between the two examiners’ HIMP gain values or left SHIMP gain values. However, a statistically significant difference between right SHIMP gain values was found. Especially in the SHIMP test, the confidence intervals for both examiners were wider, particularly for the inexperienced examiner.
We used a commercially available system which was easy to use for both the experienced and the inexperienced examiner in a healthy adolescent population.
Limitations of HIMP testing
Ensuring a tight fit of the goggles is important to minimise slippage and errors in the recordings. A tight fit appeared to be well tolerated in the adolescent test group. For some pupils, the goggles were too large; however, this was overcome by pulling the strap tighter and seemed to pose no problem. The frame and structure of the ISC impulse goggle is not particularly flexible, but a small padding is inserted. Since this study was conducted, the padding has become available in different sizes, making the fit of the goggle even better. This may prove to be important for testing of children with smaller head circumferences.
The software system conducts a quality check on every given head impulse before the impulse is either approved or rejected. In recent literature, it was stated that the head velocity must be above 150°/s [4]. Our equipment accepts head impulse velocity as low as 120°/s, a potential pitfall for the inexperienced examiner. However, getting the head impulse velocity above 150°/s does not seem to pose a problem as the examiner becomes more experienced.
Both examiners got more head impulses rejected by the software system when performing the SHIMP test than when performing the HIMP test. It seems crucial to keep the angle of the head impulse small in the SHIMP test. Four of our test reports performed by the experienced HIMP examiner showed what appeared to be covert saccades in the SHIMP. We found that this could be explained only by anticipation of the direction for the next given head impulse, see Fig. 4. We hypothesise that there is a high risk of anticipation if the examiner does not always slowly return to the starting point with the subject looking straight ahead before applying the next head impulse. This is in line with the paper by Rey-Martinez el al. [11].

Test report example. Test report with results from the HIMP and SHIMP tests. Normal HIMP test with gain-values close to 1 and no saccades. In the SHIMP there is early saccades that occur before the end of the head impulse. We hypothesize that these saccades occur due to anticipation of the direction of the next head impulse.
This could possibly also explain why four of the tests performed by the experienced examiner ended up having too many artefacts and did not enter the analysis.
After removing obvious artefact impulses from the result of each test, the gain values presented from the system were used in the analysis. Gain values reported in other reports are often calculated after being run though own special software for the calculation of gain value [8, 14]. However, this is impractical in an everyday clinical setting. For that reason, we are report the results on the SHIMP as provided by the Otometrics software system.
Surprisingly, the results of the HIMP test did not differ between the two examiners. During the editing for erroneous eye measurements we found that the inexperienced examiner produced more bounce, but we did not notice a difference between the gain values or the range. In conclusion, the software for the HIMP test reliably rejected or accepted the applied head impulses. It is also worth noting that the software system accepted head impulse velocity values as low as 120°/s, and head velocity has previously been described to influence the gain value in both HIMP and SHIMP [12]. The mean head impulse velocity was lower for the inexperienced examiner.
The mean HIMP gain values are in agreement with previous reports on healthy individuals in this age group [6, 18]. However, one must always be careful when comparing gain values as they can be calculated in different ways. The Otometrics system provides a gain value which is calculated as the ratio between the area under the curve from the eye and head movement. Other systems may, for instance, provide regression gains or instant gain values at different times during the head impulse [2]. We found a significantly lower left gain value in both HIMP and SHIMP tests. Previous research has also reported lower left HIMP gain values. This variation may be attributable to physiologic differences in the eye movements [10] or to the fact that both examiners were right-handed [1].
The present study is the first to describe SHIMP data from healthy adolescents. In agreement with SHIMP reports in healthy adults [8, 14], all our healthy adolescents produced large SHIMP saccades. As previously mentioned, there is no standardised method for calculating gain value, but the presence of covert saccades in HIMP poses a problem for the calculation of gain values. In SHIMP, calculation of gain is not distorted by covert saccades, which may prove to provide a more reliable gain value [16]. MacDougall et al. predicted that the gain value would be the same in the two paradigms, but found the SHIMP gain value to be slightly lower and speculated if this was due to the de-saccade algorithm [8]. Rey-Martinez also reported this disparity even after controlling for known confounders [11, 12]. Furthermore, in our study the gain value in the SHIMP test was lower than the HIMP gain value. There was a wide range of SHIMP gain values in this study, especially for the inexperienced examiner. Even an experienced HIMP examiner needs practise and awareness of the limitations when preforming the SHIMP.
Shen et al. found that the ability to generate SHIMP saccades mirrored the degree of complaints from patients with vestibular deficits, and therefore hypothesised that training patients to make SHIMP saccades could improve their functional outcome and reduce the number of complaints [14]. Hopefully, future studies will elucidate this hypothesis.
We performed both SHIMP and HIMP tests with minimal extra time consumption. This was primarily owed to the goggle calibration being applicable to both tests, and the SHIMP test being very intuitive for the participants. Possibly, the SHIMP may in time replace the HIMP and this potential needs to be explored. However, at present, the two tests complement each other. This is partly owed to the fact that it is not possible to test the vertical semicircular canals with SHIMP, but it has future potential.
The HIMP and SHIMP test are easily performed in healthy adolescents. No corrective saccades were present in the HIMP test, but large SHIMP saccades were seen in the SHIMP test. The SHIMP gain values were lower than the HIMP gain values.
An awareness of the limitations when preforming the head impulses is important for both the experienced and the inexperienced examiner. In our study, SHIMP testing proved to require additional practise even for the experienced HIMP examiner. This may be due to the fact that neither of the examiners was aware of the described considerations needed when performing a head impulse for the SHMIP test. Further research should be undertaken to investigate the proposed superior reliability of SHIMP gain value in patients with vestibular deficits and its clinical appliance in monitoring of progress in vestibular rehabilitation.
Funding
The study has received no funding, and the authors have no financial interests to disclose.
Footnotes
Acknowledgments
We kindly thank Ian Curthoys for commenting on some of our HIMP and SHIMP reports.