
Abstract
How do policymakers deal with the tension between choice and equity in healthcare? An analysis and critical examination of Swedish policymakers’ arguments when introducing legislated choice of primary care provider in 2010 shows that even when deciding on a reform with a potentially great impact on distribution of health resources, implications for equity were not systematically addressed. Effects with regards to current patterns of healthcare consumption in the population as well as existing inequalities in health outcomes were not adequately addressed. Neither was the primary are choice reform, which is based on the values of consumerism and individual choice, problematized in relation to current healthcare legislation such as the Health and Medical Services Act. Given that the values of equity and social solidarity have had such a prominent place in Swedish health policy and discourse in past decades, this is a surprising finding. In conclusion, we argue that because inequalities in health constitute one of the main challenges for public health today, the impact of healthcare reforms on equity should receive more attention in policymaking.
Introduction
In European healthcare, individual liberty in the form of patient choice of healthcare provider is becoming increasingly important, manifested in new and updated choice policies in many countries, not least the UK and Scandinavia (Bevan et al., 2010; Schlesinger, 2010). Besides empowering patients, choice reforms are used by policymakers trying to improve healthcare system performance. There is, however, a potential conflict between choice and equity, especially in collectivist systems (Barr et al., 2008; Oliver and Evans, 2005). Koivusalo et al. (2007) argue, for example, that the greater the freedom to choose healthcare provider, the greater the risk of inequalities – most at risk are those who have little capacity to choose and those who are particularly vulnerable. This conflict should present a challenge for policymakers making decisions on healthcare choice reforms (see Dixon and Le Grand, 2006). How important is individual choice in relation to equity and how may the best trade-off be reached? Discussing patient choice and equity in the British National Health Service (NHS), Fotaki (2010) argues that well-established causes of inequalities in health – related to, for example, social class and power – are not fully considered when choice reforms have been proposed, and neither are impacts on equity. In this article we investigate how policymakers introducing a patient choice reform in the primary care sector in Sweden in 2010 dealt with the same challenge, for example, the inherent tension between the values of choice and equity. The reform, which implies a fundamental restructuring of the primary care sector in Sweden (Anell, 2010), arguably constitutes the most far-reaching choice policy in Swedish healthcare so far.
By tradition, Swedish healthcare – and Swedish welfare more generally – is based on principles of universality and equity (Rothstein, 1998). In an international perspective, the Swedish welfare state’s ambitions to redistribute resources between different groups of citizens have been very far reaching. The Swedish politics of redistribution has aimed to reduce disparities in individuals’ ‘life chances’, that is, to increase equity, for example by equal access to education, equalization of income disparities in the wage worker collective – and very important in this case – the right to healthcare according to need, based on collective financing. The preamble to the Swedish Health and Medical Services Act (1982: 763) is in fact a formulation of equity. It is stated that ‘the goal of all healthcare services is good health and healthcare on equal terms for the entire population’ and that ‘the person with the greatest need for healthcare shall be given priority’.
Based on the central position of equity in Swedish healthcare, we consider Sweden to be a particularly interesting case to study for several reasons. First, equity has long been a central goal in Swedish healthcare. Perhaps more than in any other western country, the post-war Swedish healthcare system has been designed to ensure that all citizens receive healthcare on equal terms, regardless of ability to pay. To combat socioeconomic inequalities in health outcomes, as well as equal access, continues to be a key objective for Swedish governments. At the same time, Sweden was one of the first countries with an integrated system to embrace the principle of patient choice in the late 1980s. Since then, creating more opportunity for choice has been a central policy, particularly for right-wing parties. The reform discussed in this paper (the primary care choice reform) is thus the last step in a long political process to establish choice as a central value in the system. Hence, the potential conflict between choice and equity can be considered especially pronounced in the case of Sweden, where the long-standing commitment to equity is now challenged by the desire to enhance patient choice. Second, in terms of case selection, we consider Sweden a so-called ‘most-likely’ case. Given Sweden’s policy trajectory of heralding the value of equity, Sweden can be seen as the country where it is most likely that the principle of patient choice is problematized from an equity perspective.
Choice of primary care provider
This paper focuses on choice of primary care provider. The primary care sector is crucial for equity in healthcare as it is through this part of the system that people first get in contact with healthcare professionals. Hence, access to primary care determines the speed with which medical needs are addressed and whether adequate specialized healthcare is given in time for efficient treatment. Following the reform, the allocation of resources within the primary care sector in Sweden will follow the choices of individual patients, rather than the previous logic of geographic planning and local political priority-setting (see Anell, 2010).
As in most healthcare systems, there are differences in health between socioeconomic groups in Sweden. These differences have also increased in recent years (Socialstyrelsen, 2010). When the choice reform was prepared, some researchers (for example, Burström, 2009) pointed out the risk that equity problems might be intensified, for example, as a result of unevenly distributed interest in making choices, depending on age, health status and socioeconomic factors (see Hjelmgren and Anell, 2007). The overriding research question posed in this paper is how such risks were addressed by Swedish politicians as they introduced the primary care choice reform. To what extent was the inherent tension between equity and choice in healthcare discussed in the political debate concerning the reform? Were there differences between different political actors in this regard? And, if equity concerns were addressed, what type of equity was seen as most important to preserve?
The main finding of the paper is that the potential conflict between choice and equity was not adequately problematized by the government, despite the fact that many commentators pointed to it during the policymaking process. In the government bill presenting the reform, choice was not problematized in this regard. In the following parliamentary debate, the government maintained that it saw no such conflict, as increased choice would create more opportunities for access to primary care for all, including those with lower socioeconomic status. The opposition, represented by three opposition parties on the Left, argued that the reform would risk deepening existing inequalities. Second, the analysis showed that the debate was polarized and that arguments were put forward on an ideological basis rather than based on a thorough investigation of the potential effects on primary care utilization in Sweden. A third finding was that no political actor discussed the relation between the values underpinning the primary care choice reform (individual choice and consumerism) and the values of the current healthcare legislation in Sweden, which places a strong value on equity and need-based healthcare. These findings suggest that politicians sometimes stay away from discussing trade-offs between policy principles.
Methodologically, the empirical research presented in the article draws on ideology analysis (Freeden, 1998), in this case of arguments put forward by politicians as the reform was presented to the parliament. Arguably, passing laws is one of the most important instruments for governments wanting to change policies in the healthcare sector, and their motives behind introducing such changes merit close scrutiny if we want to understand how healthcare systems evolve over time. The study is hence limited to the parliamentary process whereby the primary care choice reform was presented and decided on; we do not cover, for example, debates in the media. This methodological choice is also motivated by the fact that, in the case of the primary care choice reform, media mostly covered debates in single county councils; the main discussion of it was confined to the parliamentary arena. The empirical analysis in the article treats the nature of the arguments put forward in this process by the main political actors in this arena, the political parties represented in the parliament. These arguments are found mainly in the political documents accompanying the reform (the government bill and the reservation to it signed jointly by the opposition parties) and the public debate held in parliament when the reform was formally presented to it. In our analysis, we present these arguments in two main categories; arguments for introducing patient choice, which are expressed by the government and MPs from the governing parties (the Moderates, the Liberal party, the Centre party and the Christian Democrats), and arguments against introducing patient choice, expressed by MPs from the parties in opposition (the Social democrats, the Left party and the Green party). As our research question is how the value of patient choice was regarded in relation to the value of equity in resource distribution, the analysis concerns only this part of the political debate. In order to give an overview of the arguments put forward in these different texts, we employ a framework of interpretation where we identify three main dimensions of equity: distribution according to need; equality of access; and equality of health. Following the presentation of the arguments as they were put forward in the political debate by the government and opposition parties, we also provide a critical analysis of the validity of these arguments by relating them to (a) scientific evidence with regards to the causal relations proposed and (b) their consistency in relation to existing healthcare legislation in Sweden. In this way we also assess at least some aspects of the quality of the arguments. Prior to the empirical analysis in the paper, we give a brief theoretical overview of the discussion on the concepts of choice and equity in healthcare and the relation between them, as well as a presentation of the contents of the reform and the policy process through which it was constructed.
Theoretical overview: the tension between equity and choice in universalistic healthcare systems
Barr et al. (2008) refer to choice and equity as fundamentally competing ideals, because choice is often associated with individualism and autonomy, while equity is associated with collectivism and justice. The core goal of communitarian states’ comprehensive welfare commitment is to enable all citizens to realize their own chosen life plans. Citizens are regarded as a collective group with certain values worth defending, for example, social equity (Rothstein, 1998). Fotaki (2010) and Oliver and Evans (2005) claim that individual choice (that is, the notion of individual difference) contravenes collectivist principles that are the foundation of the tax-based or universalistic healthcare systems, such as the British National Health Service (NHS) and the healthcare systems of the Nordic countries – principles implying that access to healthcare is to be based on need, rather than ability to pay, occupational affiliation or geographic location. Fotaki (2010) argues that patient choice policies and ideas about their outcomes originate from normative neoclassical economics (identical patients driven by the desire to maximize utility), which does not correspond to how choices are really made. For example, different patient groups value choice differently (Hjelmgren and Anell, 2007) and individuals’ conditions for making choices differ greatly (Dixon and Le Grand, 2006). Thus, enhanced individual choice runs the risk of benefiting some and harming others (Oliver and Evans, 2005). Several variables are likely to affect the choices people make, for example health-seeking behaviour, values, family and cultural beliefs, age, education, gender, effects of illness and last but not least, preferences, which are in part predetermined (Le Grand, 1991).
Libertarian principles for organizing welfare imply that the state may not restrict citizens’ freedom of choice or freedom to pursue their own life plans. Furthermore, the state should be neutral with regard to the choices citizens make and their potential mistakes (for example, choosing ‘the wrong’ provider). From a liberal viewpoint on equity – focusing on equal opportunities of choice or access rather than on equal outcomes – policymakers argue that choice improves equity by also extending choice to those who lack resources or voice (for example, Fotaki et al., 2008). Thus, all patients – not only the well off – are given the opportunity to choose. In response, it is suggested that the claim that increased individual choice will increase equity must be backed up by evidence concerning how it affects the causes of healthcare inequalities, otherwise inequities may even be exacerbated (for example, Goddard, 2009). Supported choice (Dixon and Le Grand, 2006) and empowerment of groups that are less well off (Burström, 2009) are possible measures to enhance equality of opportunity to choose.
Empirically, it has not been clearly established whether choice leads to decreased or increased equity in healthcare, or whether healthcare utilization patterns remain unchanged. A complicating factor when trying to gather evidence is that choice is a complex matter, as there are different types of choice, numbers of choice alternatives and levels of care. Robertson and Burge (2011) conclude that, within the NHS, there is mixed evidence concerning the effects of choice on equity (see also Fotaki et al., 2008). In their patient survey, however, Robertson and Burge find a social gradient in which patients (more educated and affluent) choose elective care at a non-local provider, which they suggest could result in inequitable access to high-quality care. Dixon et al. (2010) present similar results. In Sweden, there is still no conclusive evidence as to possible negative effects on equity, but several recent research reports point to the fact that there might be such effects. For example, a study by Glenngård et al. (2011) indicated that younger people, who are by definition more healthy and hence represent less economic risk to healthcare providers, are more likely to use the right to choose a care provider outside their area of residency. In 2012, the Swedish National Board of Health and Welfare presented a follow-up on the primary care choice reform where they concluded that without support for vulnerable groups, the reform is likely to lead to further socioeconomic inequalities in health (Socialstyrelsen, 2012).
Towards a theoretical framework for studying arguments about equity in healthcare
There is no universal theory of equity in healthcare, that is to say, about what should be equitable. Equity can be strived for with regards to, for example, resources, access, health services utilization and health outcomes. However, most scholars tend to agree on the centrality of three equity principles: distribution according to need (rather than ability to pay), equality in access to care services and equality in health outcomes (Culyer, 2001; Culyer and Wagstaff, 1993; Wagstaff and van Doorslaer, 2000). In the literature the concept of need has two dimensions: a horizontal dimension, implying that people in equal need should be treated the same; and a vertical dimension, implying that people with greater needs should be treated more favourably than those with lesser needs (see Culyer and Wagstaff, 1993). It has been argued that it is too simplistic to define need by ill health. A common suggestion is that need should instead be defined as the capacity to benefit from healthcare in terms of improved health. Need is thus different from preferences or wants, which may occur independent of the capacity to benefit.
Equality of access is the perhaps most common distributive principle used in health policy documents. It refers to the idea that ‘access to health services ought to be the same for those in equal need but different for people with different needs’ (Culyer and Wagstaff, 1993: 442). Access to treatment refers to opportunity, while receipt of treatment (utilization) refers to both opportunity and whether a person makes use of his/her opportunity (Wagstaff and van Doorslaer, 2000). Equality in health outcomes is a principle that links healthcare to ‘good health’, which in turn is necessary for an individual to ‘flourish’ or realize his/her life plans. An equitable distribution of healthcare is one that gives rise to equal distribution of health (Culyer and Wagstaff, 1993) or the opportunity for all individuals to achieve the same level of health (Wagstaff and van Doorslaer, 2000).
As we analyse the arguments put forward by politicians regarding the equity implications of the primary care choice reform below, we will utilize the three equity principles in order to structure the analysis. In this sense, the three equity principles identified in this section function as a framework of interpretation in the article that helps us provide a deeper analytical description of how the reform has been debated by political actors in Sweden and how these have used different types of arguments regarding equity in order to either critique or defend the reform.
The primary care choice reform in Sweden
Sweden has a long history of social democratic rule, interrupted in the postwar period only in 1976–1982 and 1991–1994. In 2006, there was a new shift in government as a centre-right four-party coalition led by the liberal-conservative party, the Moderates (Moderaterna), took office. The other coalition parties are the Centre party (Centrepartiet), the Liberal party (Folkpartiet) and the Christian Democrats (Kristdemokraterna). The change of government in 2006 has had a substantive impact on healthcare policy, foremost in the sense that policies in this area have become more market-oriented and consumerist in orientation. Hence, the primary care choice reform of 2010 is just the most recent in a series of market-oriented changes launched within the healthcare system by the liberal-conservative government. Generally, the government’s policies have been designed to strengthen the position of the patient in the role of healthcare consumer and to provide more plurality on the provision side by removing barriers of entry for private providers. This can be seen as reflective of a broader political agenda shared by all the coalition parties where welfare services are reformed along the lines of market-orientation, and welfare users are given more individual freedom to choose between different service providers within the framework of a publicly financed system. Aside from the ideological aspects of this reform agenda, attempts to strengthen the role of the patient within the Swedish system in recent years can be seen against the backdrop of earlier criticisms of the system – also from the political Left – as being weak in regards to values such as patient responsiveness and opportunities for individual choice (Or et al., 2010). The liberal-conservative government has, however, not questioned the centrality of the values of equity and solidaristic financing in the current healthcare system.
The question of patient choice has been debated within the Swedish healthcare system for at least 20 years. After the system was brought under direct political control in the 1970s, the choice of healthcare providers became highly limited. Instead, the system became organized on the basis of principles such as public planning and geographical distribution of healthcare services. Patients were typically directed to local health centres and hospitals on the basis of residence. In response to growing criticism due to the lack of choice and user responsiveness during the 1980s, a string of political initiatives in order to provide increased opportunities for choice were introduced in the 1990s and 2000s (Fredriksson and Winblad, 2008). As the Swedish healthcare system is governed foremost at a local level, by the relatively autonomous 21 county councils/regions, such initiatives have been voluntary rather than binding, so as to preserve the autonomy of the county councils. The 2010 primary care choice reform broke this pattern, as it made it mandatory for all county councils/regions to introduce choice of primary care providers as well as the principle that the choices of patients direct the allocation of resources within the system. The willingness to limit local autonomy in this regard can be said to reflect the stronger ideological commitment to the principle of choice on part of the centre-of-right parties that formed the 2006 governing coalition. The leftist parties, including the social democratic party have previously taken a more ambiguous approach to the principle of patient choice, as they acknowledge the potential conflict with regards to other values in the system, such as solidaristic financing and needs-based distribution (Blomqvist, 1996). This differing attitude with regards to the value of choice is reflected also among the local political leadership of the county councils, which are directly elected by the constituents. As shown by Fredriksson and Winblad (2008), Social Democratic county councils have generally more negative attitudes toward patient choice than do county councils governed by conservative and liberal parties.
The background to the 2010 primary care choice reform is thus a political desire to make the system more responsive to patient demands and to provide more opportunity for private healthcare providers to operate within the system. The process of legislating on the reform began in 2007, when the centre-right government appointed a single-member commission to develop a reform proposal. The final report of the commission was presented in April 2008 (SOU, 2008: 37). At this stage, as is customary in Swedish politics, a wide range of consultative bodies were invited to comment on the report and its proposed course of action. The general attitude among these bodies, which included county councils, professional groups and other government agencies, as well as patient groups, was a positive one, even if several organizations pointed out that the consequences for equity had been poorly investigated. In December of the same year, the government presented its bill (government bill 2008/09:74), which yielded four parliamentary bills. After that, a hearing was held by the Riksdag’s Social Committee, which subsequently approved the bill, although the three parties in opposition (the Social Democratic party, the Left party and the Green party) motioned through a joint so-called reservation that the Parliament reject it (2008/09:SoU9). During the Social Committee’s official hearing, several of the invited experts and practitioners raised equity concerns. The representative from the District Nurses Association, for example, said that ‘the choice reform has caused us to worry a great deal about resource-poor patients, those with multiple illnesses, the elderly, demented and mentally weak who are unable to make their case’. After a plenary debate held in the Parliament in February 2009 (2008/09:73), the reform was formally approved. In the debate, the opinions of the political parties were mainly presented by their subject area spokespersons. The legislative process is illustrated in Figure 1.
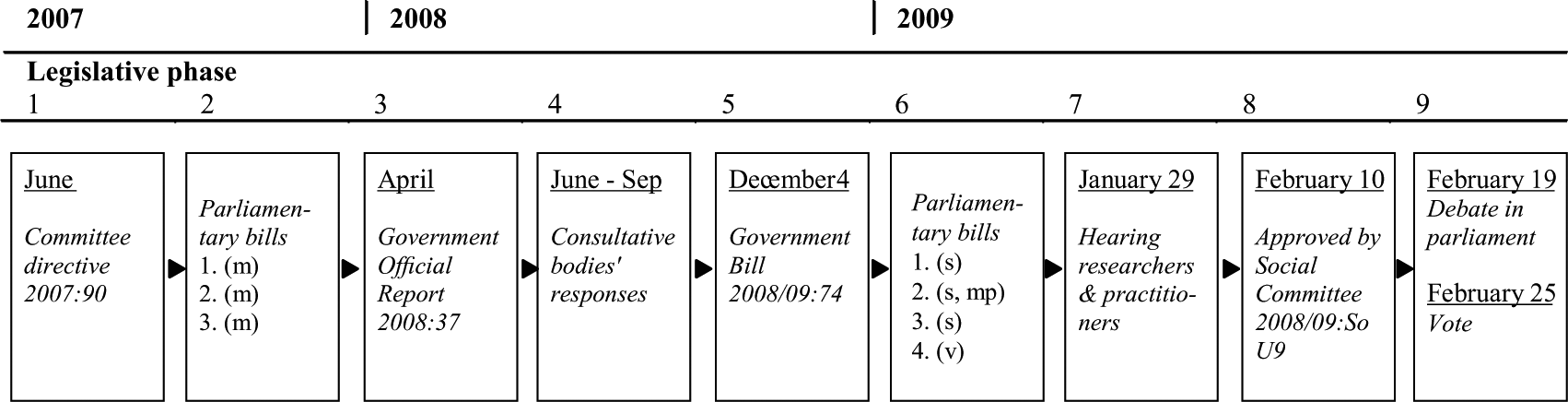
Overview of the pariamentary process.
The primary care choice reform implies that from 2010, county councils are obliged to offer patients a free choice of primary care provider and that private providers have the right to establish themselves and receive public funding on the same conditions as public providers. The reform gives county councils the freedom to decide on the concrete design of the choice model, for example, with regards to the size and structure of the reimbursement formula and rules for accreditation of providers. In this way, some of their autonomy is preserved. According to the government, the primary care choice reform had two main objectives: to empower patients by providing them with choice and second, to make it easier for private providers to establish a primary care practice with public reimbursement (government proposition 2008/09:74). The primary care choice reform implies that public reimbursement follows the individual patient’s choice of provider (a ‘money follows the patient’ principle) and that the rules for reimbursement are the same for private and public providers. This way of organizing primary care represents a major break with the traditional primary care model in Sweden, where the distribution of resources was largely decided through the county council’s budget work. Allocation based on individual choices also involves a change in the economic incentive structure, which is largely decided by the design of the reimbursement system. For example, a reimbursement model based on medical performance rather than capitation, or the number of patients listed, rewards many, short patient visits (see, for example, Belin and Kastberg, 2011). The principle of patient choice, where money follows the patient, has been discussed for the past 20 years in Sweden and been subject to political disagreement, both at the national and local level. The discussion has concerned, for example, cost-driving tendencies, difficulties for laymen assessing medical quality, the vulnerable position of the least well off, as well as effects of profit-maximizing behaviour (see, for example, Dahlgren, 1994). One concern that has been raised is whether physicians’ increased financial incentives to satisfy patient preferences may lead to adverse medical effects, such as unjustified prescription of antibiotics.
In the following section, we give a brief overview of the main arguments presented by the political parties regarding the relation between the values of choice and equity as these were understood in the context of the reform. As the political parties representing the government were united behind the reform and its goals as these were expressed in the government bill, we refer to them jointly as ‘the government’ when presenting arguments put forward. Similarly, with regard to the joint written reservation by the opposition parties on the left, we refer to arguments in this document as belonging jointly to ‘the opposition’. However, as we refer to arguments put forward in the parliamentary debate we identify the party affiliation of the speakers. It should be noted, however, that in the oral debate as well, there were no marked differences within the coalition parties or within the opposition parties. In this sense, the discussion on the relation between the values of choice and equity can be seen as having two main sides: that of the government, seeing no conflict between the two values as far as the reform was concerned, and that of the opposition, which saw the two values as conflicting in several ways.
After the debate is summarized, we move on to a more detailed review of the arguments put forward by the different political actors. Following the interpretative framework presented in the theoretical section of the article, we organize this presentation around the tree main dimensions of equity: need, access and health.
Arguments regarding the relation between choice and equity in the parliamentary debate on primary care choice reform
In general, with regard to the equity dimension of the primary care choice reform the parliamentary debate can be viewed as rather polarized. The government chose to not really address this issue, but instead to focus on the virtues of patient choice as a mechanism for resource distribution. To the extent that it was addressed, the government parties largely refuted the claim by the opposition that the enhanced opportunity of choice might result in a less equitable distribution of resources. First, the government bill presenting the reform did not discuss the potential impact of the reform on the distribution of resources within the healthcare system. Given that this aspect had been addressed by several organizations during the process of consultation and been discussed extensively by both experts and other actors when other choice reforms had been introduced previously in the Swedish healthcare system, both at the national and local level, this can be seen as surprising. Other possible consequences of the reform, such as the implications for the county councils’ financial situation, the preservation of local self-government, employment issues and even the question of gender equality between physicians, were, however, addressed. Similarly, the statement from the political majority of the Social Committee, representing the governing parties, lacked any explicit discussion about equity implications, despite the fact that this perspective had been addressed in the open hearing held by the Committee (see above). In the parliamentary debate, the government coalition parties focused on the perceived merits of the reform with regards to other values, such as the increased diversity of providers, the expected rise in healthcare quality, economic efficiency, the empowerment of patients and the general improvement in access to care, which they argued would benefit all groups, also those with weak socioeconomic status. In the plenary debate, the Minister of Health and Social Affairs – Christian Democrat Göran Hägglund – summarizes rather well which values the government associates with the choice reform: ‘Choice of primary care provider is about patient empowerment, quality, diversity of providers and access.’
The opposition parties raised the question of equity in several different ways, stressing foremost the risk that equal access to healthcare might be undermined by a pattern of establishment where private providers mainly choose to be located in areas inhabited by those who are better off, and that the demand for healthcare by those with a stronger voice might upset a pure needs-based model if care providers were exposed to stronger economic incentives to attract and hold on to listed patients. The opposition also commented on the lack of discussion on the possible equity implications in the bill, a fact that they saw as one of its major flaws. As remarked by the Left party’s spokesperson on healthcare issues during the parliamentary debate: ‘There is not a word about an analysis of consequences or evaluation of different groups’ possibilities of healthcare on equal terms.’
However, even if the government did not explicitly discuss equity implications of the reform in its bill, they did use arguments both in the bill and in the subsequent debate with an indirect bearing on equity, both with regards to need, access and health outcomes. We will now turn to the presentation of these arguments and the opposition parties’ response to them.
Arguments about equity understood as distribution according to need
The government parties used arguments relating both to distribution according to need and the concept of need itself. The core of their arguments was that when money follows the choices of patients, the system will automatically become more responsive to all patients’ needs. In the parliamentary debate, the Moderate party’s social policy spokesperson explained that ‘in this system, it is actually the patients who control resources, and then need is being met … you see reality as it is, and allow resources to follow reality.’ 1 The same spokesperson criticized the former system, where politicians ‘sit and try to draw maps’ in order to allocate resources. In a separate parliamentary bill from the Moderates, six Moderate party MPs argued that it is patients’ choices – and not political decisions – that should allocate resources in healthcare (parliamentary bill 07/08:So480). Hence, it is apparent that the governing parties see needs as best assessed by patients themselves and not by politicians. The healthcare spokesperson of the Liberal party gave this view: ‘For me the individual’s right to choose doctor and healthcare provider takes precedence over Social Democratic county council politicians’ desire to make decisions above people’s heads.’ 2
The opposition parties openly criticized the view that need is best expressed by patients themselves through their choices. The healthcare spokesperson of the Green party argued that population need is best decided by the politically elected county councils and that resources within the system should be distributed by them: ‘we must give the county councils possibilities to allocate resources through democratic decisions made by our elected representatives’. 3 All opposition parties also expressed the fear that market-based allocation of resources created by the primary care choice system would threaten the central principle of needs-based allocation of resources in the Swedish healthcare system and lead to a demand-driven system, as patients’ preferences would steer the allocation of resources. This risk was seen as especially salient given that the reform could be expected to generate an increased establishment of profit-maximizing companies in the primary care system, which could lead to an over-establishment of providers in areas where health needs were not the greatest. A social democratic MP, also the Vice Chairman of the Social Committee, argued that the reform would ‘give private providers the right to be established where it is profitable and the right to send the bill to taxpayers, whether there is a need for healthcare or not’. 4 The opposition hence saw a risk of so-called ‘cream-skimming’ or that the number of providers would vary with how costly or profitable it is to produce primary care in areas with different socioeconomic conditions, as a result of the reform, which in and of itself was regarded as a way to undermine a needs-based distribution of resources. 5
The concept of ‘need’ was used in a different way by the Minster of Health and Social Affairs, Göran Hägglund (Christian Democrat), when he clarified that it was the government’s view that ‘it is the patients’ personal needs and preferences that will determine which physicians provide them with primary healthcare’. The Minister further argued that different people have different needs, using the examples that ‘some want the doctor to be close to home, others like having the doctor near the workplace’ and that ‘patients will be able to choose a doctor with special knowledge of a specific disease, or who speaks a specific language’. The concept of need used in this way is thus more associated with patient preferences and increased customer satisfaction than medical need as such. In the plenary debate, the Minister stated this position clearly: ‘I think [choice of provider] leads to healthcare that is more tailored to the individual patient’s wishes, to greater customer satisfaction, to better development of healthcare, and to making it more responsive to the needs we have as citizens.’ The Chairman of the Social Committee, a Centre party MP, used the concept in a similar way when stating that ‘it is important that people across the country – based on their different needs and expectations – be able to decide who will be their healthcare provider’. 6
Arguments about equity of access
When it comes to the equity dimension of access, the arguments from the government and the opposition parties revealed substantive differences. The government spoke of a general improvement in access following the reform, as this was believed to lead to an increased establishment of providers. The opposition parties feared that an increase in private providers would foremost benefit the better-off, as they believed it likely that new providers would choose to be established foremost in densely populated areas and residential areas for the better-off. With such a pattern, the value of equity in access in the Swedish healthcare system risked being undermined, they argued, as this would lead to growing differences in access to primary care between geographical areas as well as between different socioeconomic groups.
The government’s arguments for a generally improved access drew both on improved entry options for private providers and the stronger economic incentive created for providers to meet the demands of patients with the new competitive system. The Moderate party’s social policy spokesperson explained this in the parliamentary debate: ‘Those who are inefficient get an incentive to actually pull themselves together and make things better, to improve themselves. It is positive; patients receive better access.’ 7 The logic of how patient choice would lead to improved access was also stated in the government bill: ‘In a choice system, individual healthcare providers take a financial risk if they are not chosen by a sufficient number of patients’ (government bill 2008/09:74).
The opposition, however, questioned whether access to healthcare would really improve in all areas as a result of the reform. They pointed to the risk that there would be areas less attractive to profit-maximizing providers, especially where access might deteriorate as a consequence of the reform. What, asked a social democratic MP, happens to people who cannot choose, people who ‘because of their disability or their age are stuck in their own neighbourhood. What happens to these people if they live in an area that is not attractive for new providers?’ 8 Hence, the opposition parties also raised the question of whether all patients have the same ability to make choices that give them access to high quality providers. This question was discussed in the government bill, where the government acknowledged that there are patients less able to make choices: ‘All patients do not have the potential to make their own choices. For example, multi-ill elderly persons who need home care. A prerequisite for these patients to make rational choices is that they have information about the options and differences between healthcare providers.’ Hence, the governments choose to see the problem of different abilities to make choices as foremost a question about information. This problem, it stated in the bill, would be addressed by the provision of better information about healthcare quality made available to patients in the future, as technology and measurement techniques improve (government bill 2008/09:74). As for the proposition by the opposition that a more demand-driven primary care system might lead to an over-consumption of healthcare by some groups who might seek care for trivial medical needs, this was refuted by Göran Hägglund, Minister of Health and Social Affairs, who argued that this was a faulty notion, which had guided health policymakers in Sweden for too long: ‘Too many healthcare politicians have acceded to the idea … that if it is too easy to get a doctor’s appointment too many healthy people will make use of healthcare resources.’ 9
However, the government did acknowledge that potential imbalances in provider establishment may have to be counteracted by adjusting the reimbursement levels to better reflect differences in patient composition in different areas. For example, the government noted in its bill that there may be reason to set higher reimbursement levels in sparsely populated areas to encourage establishment (government bill 2008/09:74). In his statement in the plenary debate, the Minister identified the reimbursement system (which county councils are free to design) as a crucial factor, stating that he wanted the county councils to try out different types of reimbursement models to find systems that would provide adequately balanced incentives for provider establishment: ‘I would like to see politicians who without prestige try out reimbursement systems, because that is the important factor in governing in a way that enables us to meet the needs of citizens in the best possible way.’ The risk for over-establishment of providers in some areas and resulting over-supply of healthcare among their inhabitants was, however, refuted by the Chairman of the Social Committee from the Centre party: ‘Obviously, when (such an area) is saturated with general practitioners, there is no reimbursement to bring home. What is the problem?’ 10
Equality of access to healthcare is further complicated if healthcare quality is taken into account. In its Bill, the government expressed confidence that choice of primary care provider would lead to an increase in medical quality within the system as a result of increased competitive pressures, as ‘large patient groups will list with the provider that provides the best quality care’ (Proposition 2008/09:74). Hence the competition mechanism in and of itself, together with the quality-sensitive choices of patients were seen by the government as a mechanism that would bring about higher medical quality. The opposition, in contrast, saw a risk for reduced medical quality within the system after the reform, as they feared that in order to maximize profit, providers will ‘chase as many visits as possible’ and ‘give priority to short, uncomplicated patient visits’ – a pattern that they thought would disfavour the chronically ill and people with co-morbidities. 11
Arguments bearing on equity in health outcomes
When it comes to the equity dimension of health outcomes, the government remained rather silent while the opposition parties, most notably the Left party, brought forward several arguments in relation to this dimension. The main argument by the opposition was that this aspect had not been properly addressed in the government Bill or the commission report that preceded it, and that the reform risked contributing to further inequalities in this regard, as it would lead to a more uneven distribution of healthcare resources within the population.
The argument that the effects of the reform had not been evaluated in light of the growing inequalities in health status within the population was put forward by all the opposition parties. 12 The subject area spokesperson of the Left party stated in the parliamentary debate: ‘We are told that there are more doctor visits and that productivity is increasing, but nothing about whether citizens have become healthier, have received proper care.’ The subject area spokesperson of the Green party asked whether the Minister himself really believed that ‘today’s unequal distribution of health will not be further enhanced?’ 13
The opposition parties also accused the governing parties of lacking an understanding of the social mechanisms behind uneven distribution of health and illness: ‘Today we know that health is closely linked to the social status one has. People with low incomes have poorer health than high income earners. The need for healthcare therefore varies between different areas and different parts of the country.’ 14 The opposition parties also argued that the reform would reinforce the unequal distribution of health outcomes within the population by re-allocating resources from groups with extensive need to groups with a lesser need and that the general public health in Sweden would deteriorate as a result of the reform. The system would become more demand-driven, they argued, and citizens with poor health could not be expected to articulate their demand for resources as actively as some other groups with lesser needs. As stated by a Left Party MP in the parliamentary debate: ‘persons with poor health are generally not the most vociferous in demanding healthcare’. 15
The government parties did not directly address the reform’s implications for equitable health outcomes but maintained that the reform would result in a general improvement of the Swedish healthcare system by strengthening the primary care sector. The subject area spokesperson of the Liberal party expressed this view in the parliamentary debate: ‘We in the alliance government make healthcare quality the top priority.’ 16
Critical analysis of the arguments
In the previous three sections, we have presented arguments put forward by Swedish policymakers that have a bearing on equity in terms of need, access and health. We will now examine the arguments put forward in the political process in the light of previous research and current regulation of equity in Sweden.
Distribution according to need
Distribution of healthcare services according to need is a central principle in Swedish healthcare. In 1995, need was defined by the Swedish Parliamentary Priorities Commission. Since then the concept implies that an individual has a greater need for healthcare the more serious the disease or the injury, or the poorer the life quality, but also that need is a function of the individual’s capacity to benefit from interventions and treatments. Thus, the need for healthcare can be valued differently by individuals and healthcare professionals. In fact, the individual is not able to establish his/her own medical need, in other words, the severity of the condition and capacity to benefit, only his/her own personal needs – which must not be confused with the need for healthcare (although the person might experience ill health). When speaking about need, the government’s definition of need seems to refer to personal needs (which may include personal preferences and desires) and not to medical needs. Thus, their rhetoric suggests that they advocate what the Swedish Parliamentary Priorities Commission called an expectation-related need concept – defining need in terms of patients’ expectations and wishes. One disadvantage of this concept is that one cannot assume that those who step into the doctor’s office are those with the greatest [medical] need (SOU, 1995: 5). This way of arguing could be linked to the fear of demand-driven healthcare and seems to be in line with the expectations of the citizens. For example, Arvidsson et al. (2009) show that a majority of patients visiting healthcare centres in Sweden thought that all healthcare needs should be met regardless of cost, even minor problems.
In addition, there is a risk that the incentives created by the new primary care choice reform may change the balance between the professionals and individuals regarding decisions about medical needs. The National Board of Health and Welfare concludes that it is relevant to follow-up whether competition for patients may be so extensive that healthcare providers are too willing to meet individuals’ needs and wants, for example by prescribing medication that is not medically justified (Socialstyrelsen, 2011).
It is important to analyse not only individual needs, but how resources should be allocated on a broader basis according to need. The government’s arguments about ‘moving past county council politicians’ 17 when allocating resources in primary care imply that political allocation – supported in the ethical platform for priorities in Sweden – should be ignored, in favour of relying solely on patient choice for allocating resources according to need (that is, health professionals employed by a plurality of providers making identical priorities). Carlsson (2010: 562), however, argues that ‘healthcare personnel still appear to be relatively unaware of the ethical principles’ and furthermore that ‘local models or documents to facilitate the priority setting process are uncommon’, which may hinder distribution according to need. Thus, in what way choice in primary care is consistent with the principles of horizontal and vertical need could be questioned. In 2009, the National Board of Health and Welfare (NBHW) concluded that highly educated people make more doctor visits than do less educated people relative to their health needs. As health is unequally distributed in the population as a function of socioeconomic status, education, income, and so on, the principle of vertical need implies that socioeconomic groups with higher rates of disease and poor health have greater needs and should be prioritized (see Burström, 2009). It also means that socioeconomic groups with lower rates of disease and poor health have lesser needs and should be given lower priority. It could be argued that to safeguard distribution according to need, Swedish policymakers should have asked and answered two important questions concerning choice in primary care: How can we make sure that people with the greatest need for healthcare are prioritized? How can we make sure that people with lesser need for healthcare are given proportionally lower priority?
Equality of access
Equality of access is highly important for equal healthcare. There are different barriers for access to healthcare services, for example, geographical, personal and economical hindrances. One type of maldistribution of access that is specifically discussed by the governing parties is between sparsely and densely populated areas, that is, geographic inequalities. Access according to need can be achieved by adjusting the reimbursement system in order to attract providers to all geographical areas. In the political debate described in the section above both political sides agree on this. The county councils, however, are in practice free to decide on the reimbursement systems, making equal access according to equal need a local concern rather than a national one. This in itself paves the way for regional inequities.
What about the distribution of access to high-quality providers? Oliver and Evans (2005) argue that those less able to make choices may effectively be left with poor quality services. The logic behind choice of primary care provider is that patients will list with the provider rating highest on quality indicators. In this way, low-quality providers will eventually be eliminated. However, given that the demand for medical care always exceeds the supply, the question is to what extent providers with low quality ratings will be eliminated and which patients will be listed with low-quality providers. An important limitation of the reform that is not discussed by politicians is that the relation between supply and demand in healthcare does not follow normal market patterns. Roemer’s Law, for example, suggests there is a supplier-induced demand, which means new establishments of providers will always create demand independent of the level of need within the population.
Another complicating factor is that once individuals have made a choice (listed with a primary care provider), they are generally not likely to change providers, suggesting that patients do not delist from providers with poor performance (Anell, 2010). In addition, chronically ill patients are less likely than others to change providers because they value continuity most highly (Schlesinger, 2010). Recent Swedish research suggests that improving health for patients who are chronically ill or have multiple conditions requires coordination rather than competition (Ahgren, 2010), indicating that choice systems face major challenges in terms of equal access to high-quality care for these patient groups.
How choices are made can be attributed to both demand- and supply-side factors. In the debate, the government primarily speaks of supply-side factors – in other words, how the actual system is designed. They argue that as long as appropriate and tailored information is available, patients will be able to make rational choices. This assumption is criticized by researchers who argue that such a model of decision-making is too simplistic, that it is thus not realistic to assume that information is easily accessible and comprehensible, and that people have defined expectations and are able to evaluate their current needs and expectations as well as future needs (Bevan et al., 2010; Schlesinger, 2010). Elderly people as a group are particularly vulnerable regarding information and are also a large consumer of healthcare. Recent research points to the fact that the problem of tailoring information to elderly people may be greater than previously assumed. Investigating the proportion of very old people (older than 77 years) who have the capacity to find information and make decisions concerning providers, Meinow et al. (2011) concludes that only a small number of very old people have the cognitive, physical and mental resources needed. A total of 10 percent did not report any of the problems measured in the study. This is a condition that is not easy to handle by information system design, as it may be described as a supply-side impairment. In addition, the proportion of people over 65 years will increase by 15 percent by 2020, implying that healthcare in the future must handle an increasing number of elderly patients who need support when choosing a primary care provider (Socialstyrelsen, 2010).
Regarding other demand-side factors, the governing parties do not discuss in-depth how factors such as education, initial health and socio-economy – related to inequities in health – affect access and the opportunities to choose. Dealing specifically with conditions for equal choice, Le Grand (1991) argues that a distribution of healthcare is equitable if choices are not affected or constrained by factors beyond individual control. Most would agree that, for example, gender and ethnicity are factors beyond individual control. How are individuals affected, however, by family background or class preferences? Le Grand points out that individuals’ choices are also affected by preferences, that is, their values, beliefs and tastes, which are at least in part the product of factors beyond individual control, such as upbringing. Therefore, individuals’ actual choices may be more constrained than would appear at first glance. In addition, there is no discussion about the fact that young, well-educated, mobile and prosperous individuals are more in favour of exercising choice of provider (for example, Ringard and Hagen, 2011; Thomson and Dixon, 2006). The opposition, in the analysis above, questions choice of primary care provider more fundamentally by arguing that all patients have great difficulties in estimating quality in healthcare, thus questioning whether competition based on quality will work. To safeguard equal access and equal opportunity to choose a provider, the Swedish policy-makers should have asked and answered two important questions: Are there structural barriers facing some groups when making choices, and how can we make sure such barriers do not translate into unequal distribution of access to high-quality care?
Equality of health
Equality of health, that is, the choice-reforms effects on individuals’ health outcomes, is an issue that the Government does not discuss at all. The discussion referred to above showed clearly that the government preferred to discuss issues of access rather than health outcomes. As ill-health is unevenly distributed in the population, the vision of equal health for all, established in the Health and Medical Services Act, requires that more healthcare resources are invested in people with ill-health. As pointed out by, for example, Starfield (2004), unequal distribution of healthcare is necessary to achieve equitable health outcomes. From this perspective, equality of health in the choice of provider system presupposes that people with poor health demand/utilize proportionally more healthcare than do healthy people. However, a great deal of experience indicates that people with poor health utilize proportionally less healthcare. Health inequalities in Sweden are at present manifested in, for example, significantly higher death rates in so-called ‘amenable mortality’ among men, foreign-born individuals and groups with a lower level of education. Moreover, people with a psychiatric diagnosis are more likely to die from a treatable cardiovascular disease (Socialstyrelsen, 2010). In order to counteract such differences when introducing new reforms within primary care, policymakers should have asked and answered a two-part question: How is health distributed today and in what way will the suggested changes in the primary care system ensure the opportunity for all individuals to achieve the same level of health? It should be noted that in the government bill the word ‘health’ (hälsa) is mentioned only once in the 65-page document. The passage reads: ‘healthcare should be based on the individual’s right to the best possible health’ (government bill 2008/09:74, p. 23).
Conclusions
We will begin the concluding discussion with three main observations from the analysis of Swedish policymakers’ arguments put forward in the parliamentary process of introducing a mandatory choice of primary care provider.
The first finding of the paper is that the potential conflict between choice and equity was not adequately problematized by the government as it proposed the primary care choice reform. In the following parliamentary debate, the government maintained that it saw no such conflict and that increased choice would create better opportunities for access to primary care for all. The dimension of equity in health outcomes, which can be said to be the most demanding principle, as it would imply a significant shift of health resources to weaker socioeconomic groups to compensate for structural inequalities in a range of areas in life, was hardly discussed at all by the government. The opposition, represented by three opposition parties on the Left, argued that the choice reform would risk deepening such inequalities.
In sum, both the governing parties’ and the oppositions’ arguments can be described as one-sided. It is a case of visions versus fears. Potential gains and losses of the reform were not weighed against each other in the actual reform design. The governing parties focused almost solely on the positive effects, asking how anyone could be against increasing choice. Contrary to that, the opposition held a critical attitude and seemed to dispute whether any positive effects at all would come out of the reform, although they acknowledged that it is important that citizens should have the opportunity to choose their primary care provider. The implications of these findings are that the policymakers shy away from discussing trade-offs between policy principles and that they do not base their arguments on empirical evidence.
Second, the political discussion seemed to be polarized and arguments were put forward on an ideological basis rather than based on a thorough investigation of the potential effects on primary care utilization in Sweden. In fact, the consequences for equity were not investigated at all in the government bill or the government official report preceding the government bill. The arguments from both sides appear to be part of broad political programmes concerned with how to manage the public sector more generally. Thus, the government appears to regard primary care as a welfare service among others. Primary care, however, has a specific function in healthcare systems. In Sweden, primary care is the foundation of the healthcare system and must accept all patients irrespective of disease, age or patient group, and carry out preventive work (1982:763 Hälso-och sjukvårdslag [Swedish Health and Medical Services Act]). It has been suggested that a major proportion of health differences in Sweden could be reduced through preventive work (Socialstyrelsen, 2010), making equity in primary care of uttermost importance.
A third finding is that no political actor discussed the relation between the values underpinning the primary care choice reform (individual choice and consumerism) and the values in current healthcare legislation in Sweden, more precisely, the Health and Medical Service Act, which places a strong value on equity and a needs-based healthcare system. The government outlines a more personal or demand-driven concept of need that conflicts with the traditional way in Sweden of letting the professionals, that is, the doctors, decide on the medical need of the individuals.
Thus, the results from the analysis of policymakers’ arguments when introducing mandatory choice of primary care provider in Sweden is consistent with Fotaki’s (2010) observation in the UK, that impacts on equity are not fully considered in the current choice policy agendas. Equity in terms of need, access and health were sporadically addressed during the legislative process in Sweden, that is, in an ad hoc rather than in a systematic way. Even though the decision concerned a reform with a potentially great impact on health and the distribution of health, the reform was founded on ideology (visions versus fears) rather than a systematic investigation of possible consequences for equity – the primary objective of Swedish healthcare. A systematic approach to addressing equity consequences should have been based on an overview of current socioeconomic differences in health, as well as regional and gender differences, and in addition, on some predictions about how the choice reform would reduce the established differences, or at least how to maintain the status quo. In fact, the Swedish government did not discuss the effects on existing socioeconomic differences in health, and it did not discuss how the reform might benefit the most disadvantaged.
It is, however, worthwhile to ask whether politicians are supposed to base their decisions on scientific or empirical evidence. Isn’t their role to present visions for the future – visions about how we can best organize society? The Social Democrats – who have been the governing party for most of the post-war period in Sweden, are being criticized from within their own ranks for lacking vision in social policy. Dealing with value trade-offs, such as that between choice and equity, in the seminal work Democracy and its Critics, Dahl’s critics of ‘guardianship’ (expert rule) argue that ‘there may not be an expert answer to the problem’ (Dahl, 1989).
As Sweden is a country that traditionally has placed great emphasis on equity, it seems likely to assume that equity aspects are unlikely to be sufficiently addressed when introducing new choice policies in European healthcare today. As inequalities in health, related to socioeconomic status, constitute one of the main challenges for public health today (Mackenbach et al., 2008), the importance of investigating the impact of healthcare reforms on equity should receive more attention. Similarly, the WHO Commission on Social Determinants of Health (Commission on Social Determinants of Health, 2008) concluded that to reduce inequities in health, responsibility for action on health and health equity need to be placed at the highest level of government.
Finally, the analysis of the Swedish policymakers’ arguments also indicates that the Swedish healthcare system is undergoing a transformation. The notion that patients are given control over the allocation of healthcare resources actually implies a major change in democratic decision-making in Swedish healthcare. The government argues that choice ‘democratizes healthcare’. Drawing on Fotaki (2011), however, one can also view the recent policy changes as Swedish being consumerized. The consumer role is linked to the option of exit, use of information and control of resources, which is consistent with the present reform ideas, while the citizen role is linked to voice, participation and political influence. Furthermore, the suggestion that choice democratizes healthcare may be problematic from a constitutional point of view, as Swedish democracy is to be realized through representative and parliamentary polity and by local self-government (Instrument of Government 1:1). Bypassing the political process means that some democratic processes will be sidelined, for example, aggregation of interest, political goal-setting, the safeguarding of social interests and political mobilization.
The reform and parliamentary debate presented in the article illustrate that libertarian principles are gaining importance vis-a-vis communitarian principles as regards the relation between the state and citizens. Swedish welfare policy has largely been built on communitarian principles and ‘uniform standard solutions’ in healthcare (Rothstein, 1998). The patient choice reform signifies a shift towards an increasing emphasis on autonomous individuals and a state that is neutral to the choices people make. Primary healthcare seems to be less ‘a common project’ and more an individual project. Linked to this transition is the question of whether health outcomes are important. That is, is actual utilization of primary care or health distribution. What matters? Or is it important that all individuals are given the same opportunity to make choices? The explicit purpose of the reform is to increase citizens’ individual autonomy – by empowering them to make individual choices in their role as patients. The expected result is of course that will make different choices – otherwise there would be no need for a choice reform. The question is whether or not these differences are equitable.
Footnotes
Notes
Acts and bills
1974:152 Kungörelse om besultad ny regeringsform.
1982:763 Hälso- och sjukvårdslag [Swedish Health and Medical Services Act].
2007:90 Kommittédirektiv. Patientens rätt i vården.
2008:37 Vårdval i Sverige: delbetänkande av utredningen om patientens rätt.
2008/09:73 Riksdagens protokoll. Torsdagen den 19 februari. Anförande (statement)1–21, 88–105.
2008/09:74 Regeringens proposition. Vårdval i primärvården.
2008/09:SoU9 Socialutskottets betänkande. Vårdval i primärvården.
2007/08:So480 Parliamentary Bill by the Moderate party.
2008/09:So10 Parliamentary Bill by the Social Democrats and the Green party.
2008/09:So12 Parliamentary Bill by the Left party.