
Abstract
Background
Percutaneous radiofrequency ablation (RFA) is a common method for treating liver cancer. Compared to other treatment modalities, RFA has a higher local tumor recurrence rate due to incomplete ablation. On the other hand, to ensure complete tumor removal, multiple ablations may be necessary, but this can lead to excessive thermal damage. Therefore, improving the precision of the ablation margin control is crucial.
Objective
This study aims to investigate an algorithm-controlled ablation mode that can precisely control the tumor treatment margins. This mode uses temperature and impedance as feedback parameters to adaptively adjust the RF power output, ensuring both effective tumor ablation and enhanced safety.
Methods
The study conducted finite element analyses and ex-vivo bovine liver experiments comparing traditional constant power ablation and the algorithm-controlled ablation mode. Simulations primarily analyzed the temperature changes and ablation area in biological tissue, assessing the effectiveness of the two ablation modes. In the ex-vivo bovine liver experiments, temperature and impedance were monitored in real-time to validate the feasibility of the algorithmic ablation mode.
Results
The findings indicate that the algorithm-controlled ablation mode effectively controls the rise in tissue impedance, preventing carbonization and charring. For ablation diameters of 10 mm and 20 mm, it precisely maintained the boundary temperatures within the range of 50–60°C, ensuring effective damage at the ablation margins while avoiding excessive damage to normal tissue.
Conclusion
This study developed an adaptive radiofrequency ablation algorithm for treating liver cancer, using temperature and impedance as feedback parameters. Preliminary results from finite element analysis and ex-vivo bovine liver experiments suggest that for small tumors with diameters of 10 mm and 20 mm, this algorithm may provide more precise control of the ablation zone, improving efficiency and safety compared to traditional constant power ablation.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is the fifth most common cancer worldwide and also ranks among the highest in incidence and mortality rates, with the prevalence of liver cancer increasing annually in many countries. 1 Various treatment options are available for tumors, including liver resection, ablation procedures, and liver transplantation. 2 Radiofrequency ablation (RFA) is widely used due to its simplicity, safety, and minimally invasive nature, particularly for treating single tumors smaller than 30 mm in diameter, where it is the preferred method. 3
Radiofrequency ablation involves the precise placement of a needle-like electrode into the tumor under imaging guidance. Energy is then transmitted from a radiofrequency (RF) generator to the electrode, with the current flowing from the electrode to a grounding pad on the patient's body. During ablation, the current stir free ions within the tissue, converting electrical energy into thermal energy used to heat the tumor tissue. 4
Compared to other treatments, RFA has a higher local tumor recurrence rate due to incomplete ablation at the margins. Incomplete or insufficient tumor ablation can lead to recurrence. 5 Researchers believe that maintaining a safe margin of more than 5 mm can effectively prevent local tumor recurrence. 6 Clinically, Computed tomography (CT), Magnetic resonance imaging (MRI), and Ultrasound (US) imaging assist in RFA, identifying tumor tissue, determining electrode placement, and monitoring the ablation process. 7 However, these imaging methods have limitations, such as susceptibility to contrast agents, signal interference, and inherent technical constraints, thus lacking standardization and effectiveness.8,9
The core mechanism of RFA in treating tumors involves heating the tumor tissue to induce apoptosis, thus achieving the goal of minimally invasive treatment. 10 During heating, the extent of cell structure damage is closely related to the temperature, making temperature a crucial metric for assessing tissue damage. 11 Cells remain structurally intact below 45°C even after prolonged heating. At temperatures exceeding 45°C, cell structures begin to change after sustained heating. After 120 s of continuous heating between 50°C and 60°C, intracellular proteins denature and coagulative necrosis occurs, causing irreversible damage. 12 At temperatures between 60°C and 100°C, cells rapidly lose viability and die almost instantly. When temperatures rise above 100°C, biological tissues undergo carbonization and evaporation, dramatically increasing biological impedance and hindering the conduction of RF current, thus affecting the ablation range. 13
This study designs an ablation algorithm with controllable margins using temperature and biological impedance as control parameters for RF energy output. By assessing irreversible damage based on ablation temperature, this approach achieves quantitative measurement and ensures safe ablation margins, reducing the risk of local tumor recurrence. To validate this ablation mode, we first established a finite element simulation model to compare the effects of traditional constant power RF energy and controllable margin RF energy on tumor tissue ablation. Subsequently, ablation experiments were conducted on ex-vivo bovine liver to further explore the control effect on ablation margins under the algorithm-controlled mode.
Materials and methods
Boundary-controlled ablation method
The boundary-controlled ablation method allows for precise control over the range and degree of ablation during treatment. This ensures complete necrosis of tissues within the tumor boundary while protecting normal tissues outside the boundary from irreversible damage. The key to achieving precise ablation lies in controlling the temperature and impedance of the biological tissues.
During this process, radiofrequency energy gradually increases the temperature of tissues near the electrode. Studies have shown that maintaining the temperature of biological tissues above 50°C can induce coagulative necrosis, while temperatures above 60°C result in immediate cell apoptosis. 12 By precisely controlling the temperature of biological tissues and adaptively adjusting the radiofrequency power, the temperature at the tumor boundary can be maintained between 50°C and 60°C for a duration of 2 min. When radiofrequency energy is applied, the current density is higher near the electrode, generating more heat and causing the temperature to rise faster. 14 Conversely, tissues further from the electrode experience lower current density and slower temperature rise. As the electrode is placed in the center of the tumor, the rate of temperature increase decreases gradually from the inside out. When the temperature at the tumor boundary reaches the ablation standard, the internal tumor cells have already undergone coagulative necrosis, ensuring complete apoptosis of the internal tumor cells while sparing the peripheral normal cells from significant damage.
During ablation, if tissue impedance increases sharply, the device will immediately stop energy output and resume only when impedance decreases. To ensure the efficacy of ablation, the temperature at the tumor boundary must reach 50°C and be maintained for 2 min. Additionally, the tissue impedance should remain low and stable. This control of temperature and impedance not only promotes necrosis within the tumor boundary but also prevents tissue charring during ablation, ensuring that stable impedance indicates complete coagulative necrosis of the internal tumor tissues.
Finite element analysis of tumor radiofrequency ablation
Construction of tumor radiofrequency ablation model
This study utilized COMSOL finite element simulation software to build a model of liver tumor radiofrequency ablation. The software models the entire ablation process by accounting for the thermoelectric coupling effects of radiofrequency energy on liver tumors. The geometric model of liver tumor radiofrequency ablation is shown in Figure 1. We represent the liver tissue with a cylinder that has a diameter of 100 mm and a height of 120 mm. The tumor is modeled as a spherical geometry located at the center of the liver, with the coordinates (0, 0, 0). The electrode needle has a diameter of 2 mm and a total length of 65 mm, of which only a 10 mm segment is the active electrode. The active electrode refers to the portion of the needle that is conductive, while the remaining part is an insulated electrode shaft that lacks conductive properties. The active electrode is positioned at the center of the tumor.

Geometric model for finite element analysis of liver tumor radiofrequency ablation (side view).
In the traditional constant power ablation model, electrodes continuously apply constant power until ablation is complete. To study the impact of different output powers on ablation, we conducted simulations using a fixed tumor diameter of 30 mm and four different output powers (10 W, 20 W, 30 W, and 40 W). To investigate temperature changes in biological tissue during ablation, multiple probes were inserted into the tissue to collect temperature data. The probes were placed at distances of 10 mm, 20 mm, and 30 mm from the center of the electrode. In the simplified simulation model, the material used is uniform and homogeneous. As a result, the temperature changes equidistant from the electrode are consistent in all directions during ablation. Therefore, temperature measurement points were placed in only one direction. The specific placement of the temperature probes is shown in Figure 2.
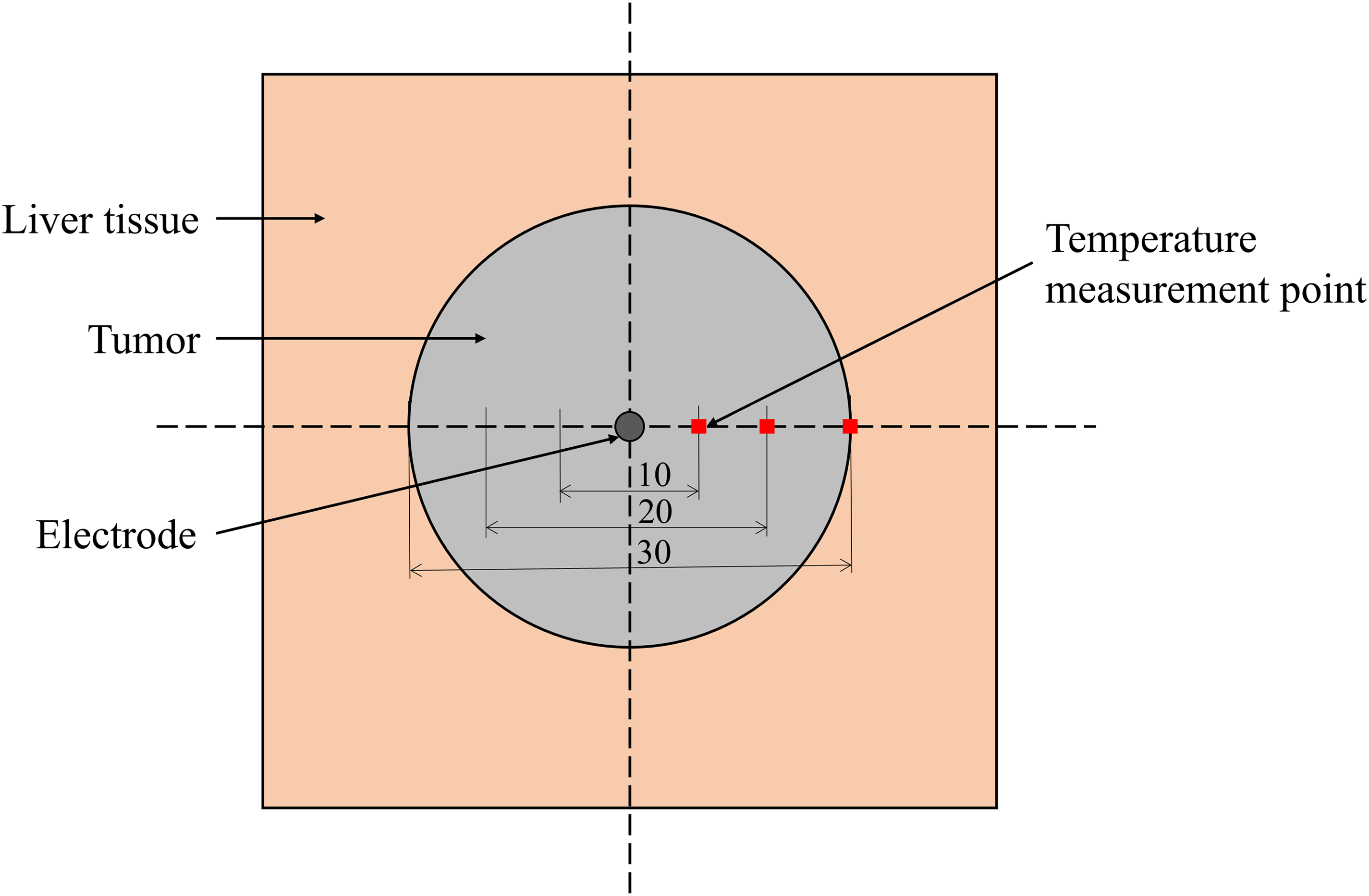
Temperature probe placement in constant power ablation mode (top view).
In the boundary-controlled ablation model, simulations were conducted to explore the control effect of the ablation boundary for tumors with diameters of 10 mm, 20 mm, and 30 mm. Four probes were placed at the tumor boundary to monitor real-time temperature changes, as shown in Figure 3, with d representing 10 mm, 20 mm, and 30 mm, respectively. In this model, when the temperature at the boundary measurement points exceeds 60°C, the power output is paused, and when the temperature drops to 50°C, the power output resumes. This method achieves temperature control. Additionally, the radiofrequency energy output value in the model is set based on the biological impedance; when the impedance exceeds 700Ω, the output power in the model is reduced accordingly.
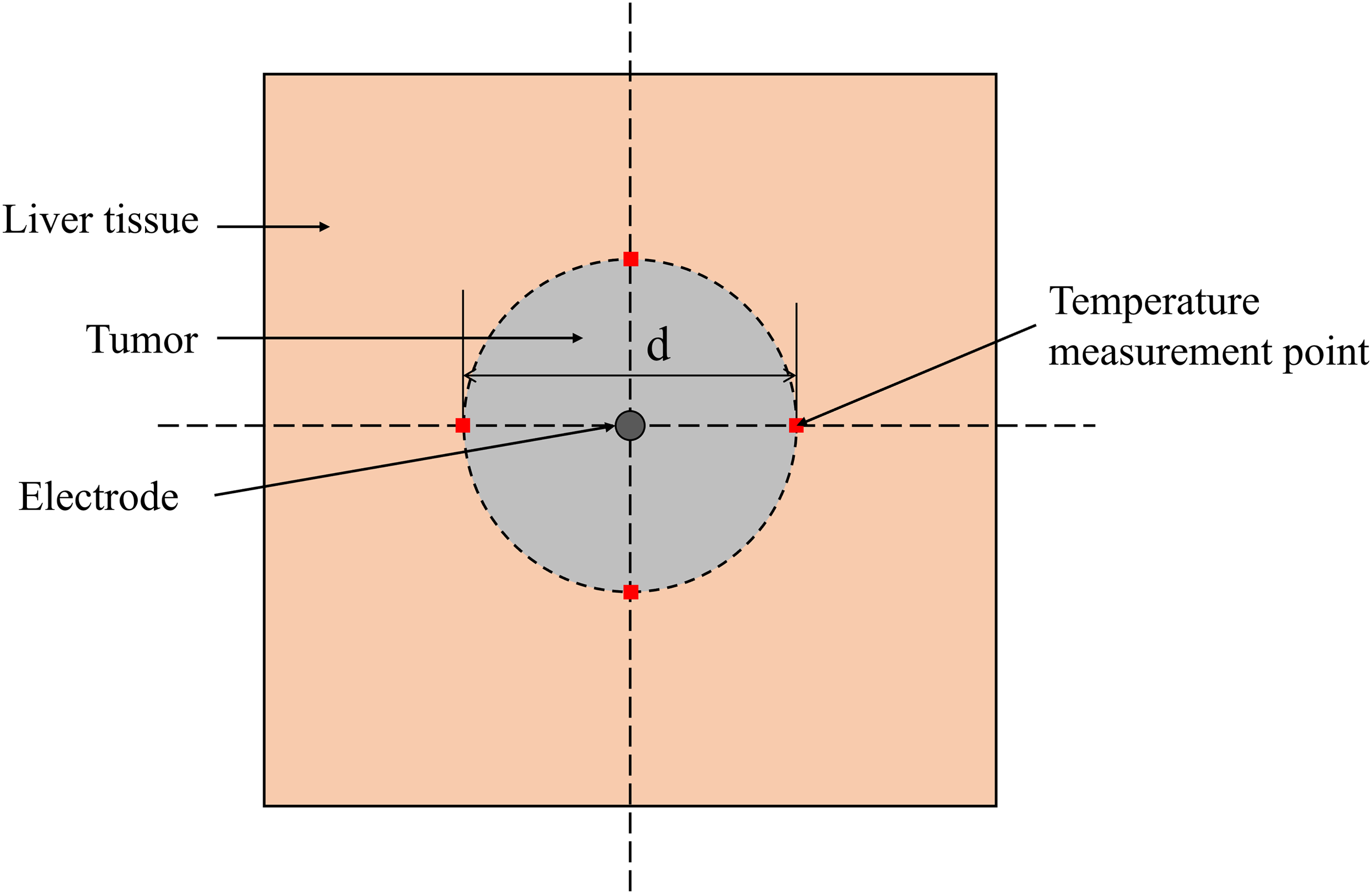
Temperature probe placement in boundary temperature control ablation mode (top view).
Electric field and temperature field
Heating biological tissue with radiofrequency energy involves the conversion of electrical energy into thermal energy, necessitating accurate calculations of the electric and thermal fields in the simulation model. The electrical potential in biological tissues is generated by the application of radiofrequency energy, and the associated electric field distribution is derived by solving the Equation (1) (Laplace equation)15,16

The static electric field in the tissue is given by Equation (2)




Finally, the thermal-electric coupling in the biological tissue is determined using the Pennes equation. The electrical and thermal properties of the tissue and electrode used in the model are taken from references,15,17,18 and are listed in Table 1.
Physical parameters of biological tissues and electrodes in the model.

Ex-vivo bovine liver ablation experiment
The ex-vivo bovine liver used in this study was purchased from a local market and delivered to the laboratory within 24 h for experimental use. Given that the liver was obtained post-mortem from a source not specifically reared for research purposes and the experiments were conducted on non-living tissue, there was no requirement to apply for and receive ethical approval for these experiments.
RF energy generating device
In the laboratory, ex-vivo bovine liver experiments were conducted using a specialized RF energy generator capable of delivering power outputs up to 300 W. This RF energy generator comprises several key components: a power supply module, a microprogrammed control unit (MCU), an RF module, and an interface module. The power supply module provides electricity to the entire device, while the main control module receives inputs such as temperature and impedance, adjusting the output power of the RF energy based on feedback. The RF module consists of a symmetrical Class E power amplifier that emits the RF energy. The interface module includes connections for RF energy output and temperature detection, facilitating communication with external systems. A temperature detection circuit collects thermal data from biological tissues and relays this information to the MCU. Figure 4 illustrates the internal module connections of the radiofrequency energy generation device, while Figure 5 shows the actual device.

Internal module connection diagram of radiofrequency energy generation device.
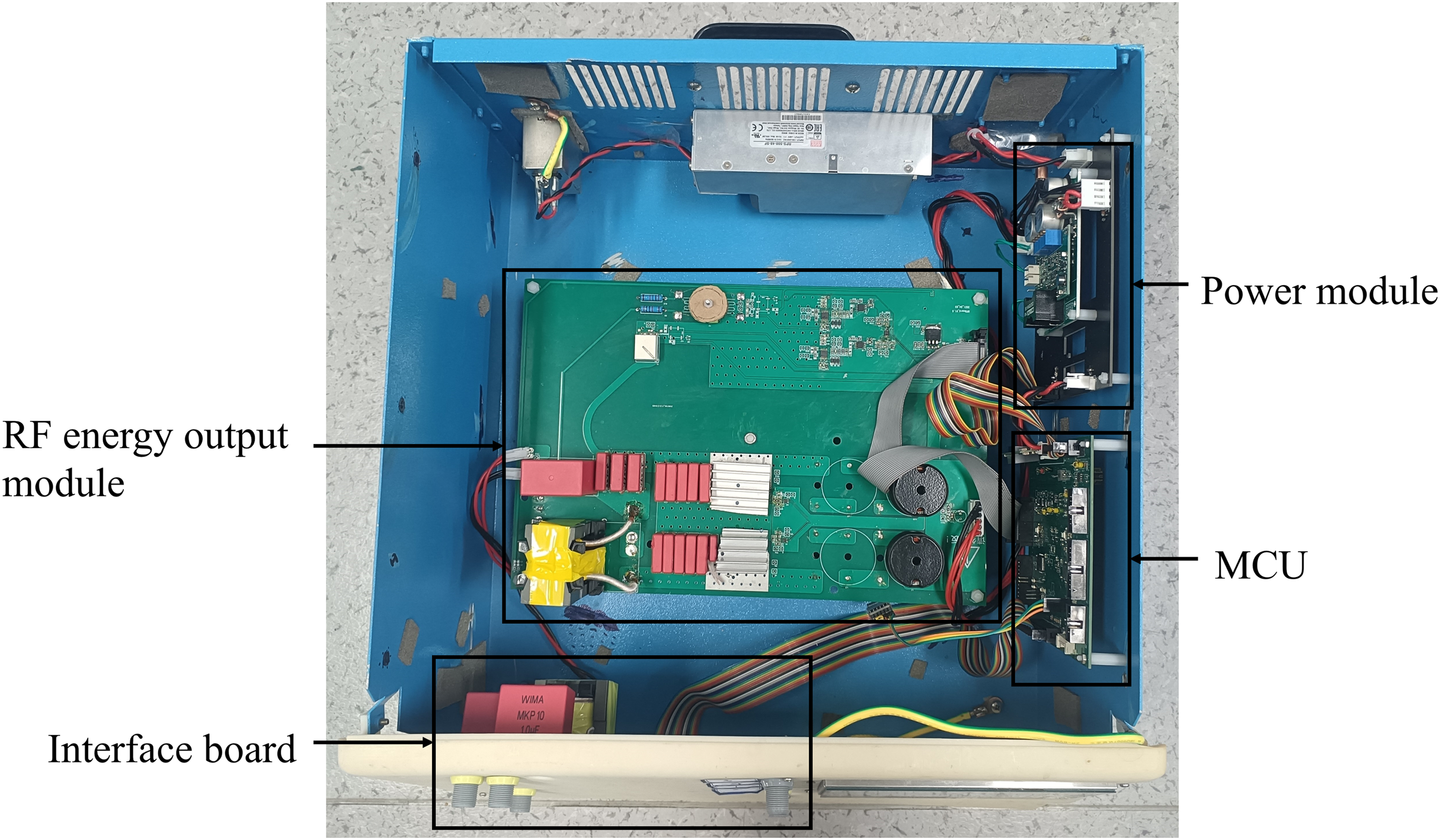
Photograph of radiofrequency energy generation device.
Adaptive ablation algorithm with controllable ablation boundary
During the application of radiofrequency energy to biological tissue, when the temperature exceeds 60°C, the water content inside the cells gradually decreases. When the temperature surpasses 100°C, the water in the biological tissue evaporates instantaneously, leading to tissue charring. As the water content decreases and charring occurs, the electrical resistance of the biological tissue increases sharply. This increase in impedance significantly impedes the transmission of radiofrequency current between the electrode and the grounding pad, thereby limiting the output of radiofrequency energy. This limitation prevents sufficient heating of tumor tissues, thereby impeding the continued application of high temperatures necessary to destroy tumor cells. 19 Therefore, to ensure unimpeded output of RF energy during ablation, monitoring and controlling biological impedance is essential. Under constant power, lower biological impedance allows for higher RF currents, which can extend the damage to biological tissues. 20 However, in the treatment of small tumors, a larger ablation zone is not always beneficial. To prevent excessive damage to the normal tissue surrounding the tumor, precise control of the ablation margins is crucial. An adaptive ablation algorithm with controllable margins, designed based on changes in biological impedance and boundary temperatures during the ablation process, is depicted in the flowchart shown in Figure 6.
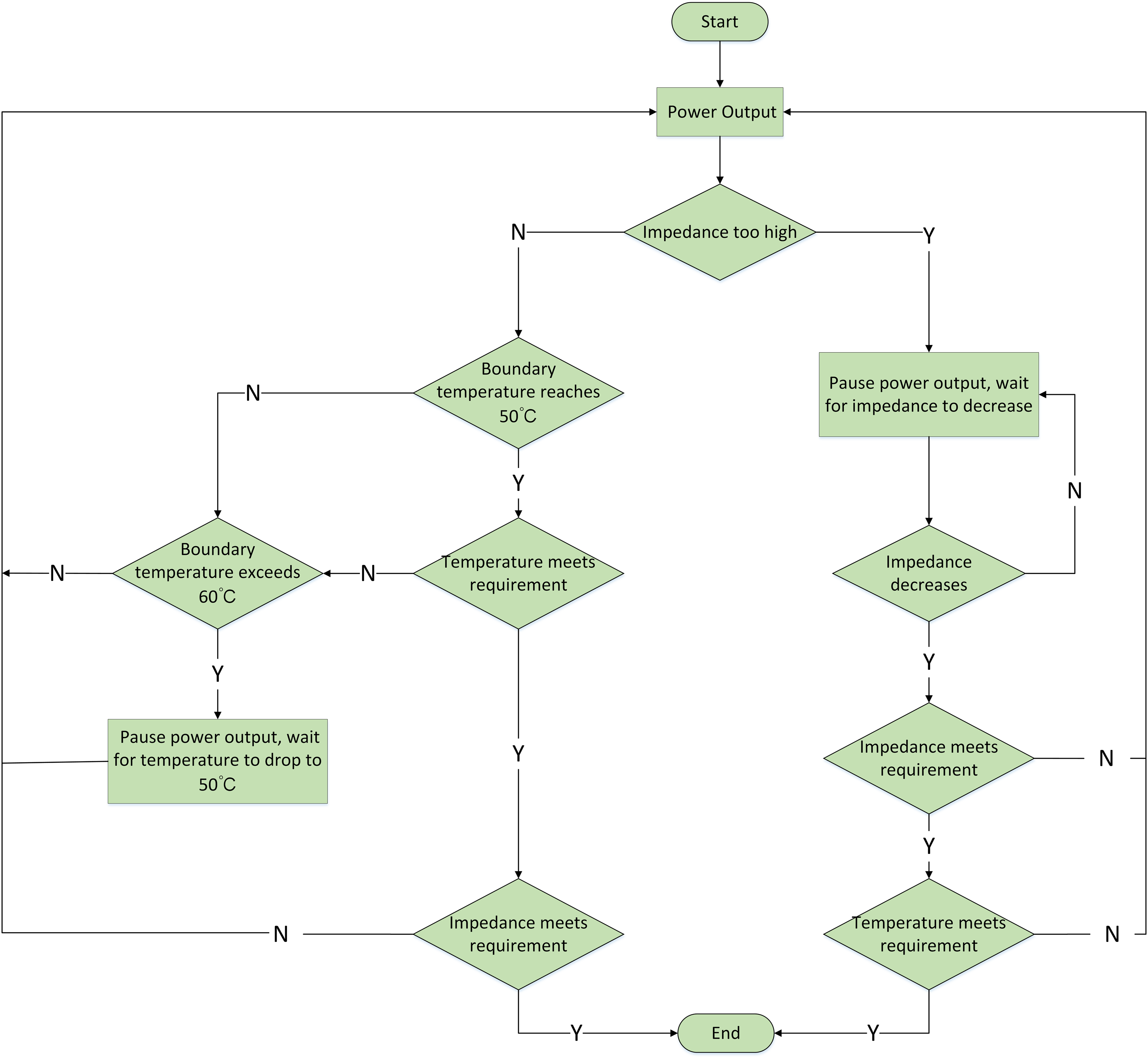
Flowchart of adaptive ablation algorithm for controllable ablation boundaries.
Typically, the temperature rise is fastest near the electrode, and this part of the biological tissue is prone to carbonization. The radiofrequency (RF) module of the RF energy-generating device is equipped with voltage and current detection circuits. These circuits relay voltage and current readings back to the main control board for processing and impedance calculation. When tissue charring occurs, the bioimpedance usually jumps from tens of ohms to several hundred ohms. 21 To prevent this, an impedance threshold is set. When the main control board detects that the bioimpedance exceeds a threshold, it reduces the radiofrequency output power. Once tissue fluid returns and bioimpedance decreases, the output power is gradually increased. This approach helps minimize the impact of tissue carbonization on the ablation range.
Furthermore, to achieve precise ablation boundary control, a temperature detection circuit using thermocouples has been designed on the interface board. This circuit collects temperature data from the ablation margins and feeds it back to the main control board for processing. A temperature threshold is also set to prevent excessive ablation. If the temperature at the ablation boundary exceeds this threshold, the main control board adjusts the RF output to maintain the boundary temperature between 50°C and 60°C. If this temperature range is sustained for more than two minutes, it is considered that irreversible damage has occurred in the tissue at the boundary.
Experimental materials and experimental platform
Figure 7. depicts the steel RF electrode needle and thermocouple used in the experiments. The electrode needle has a diameter of 2 mm and an exposed length of 10 mm. The K-type thermocouple is utilized to measure the temperature of biological tissues.
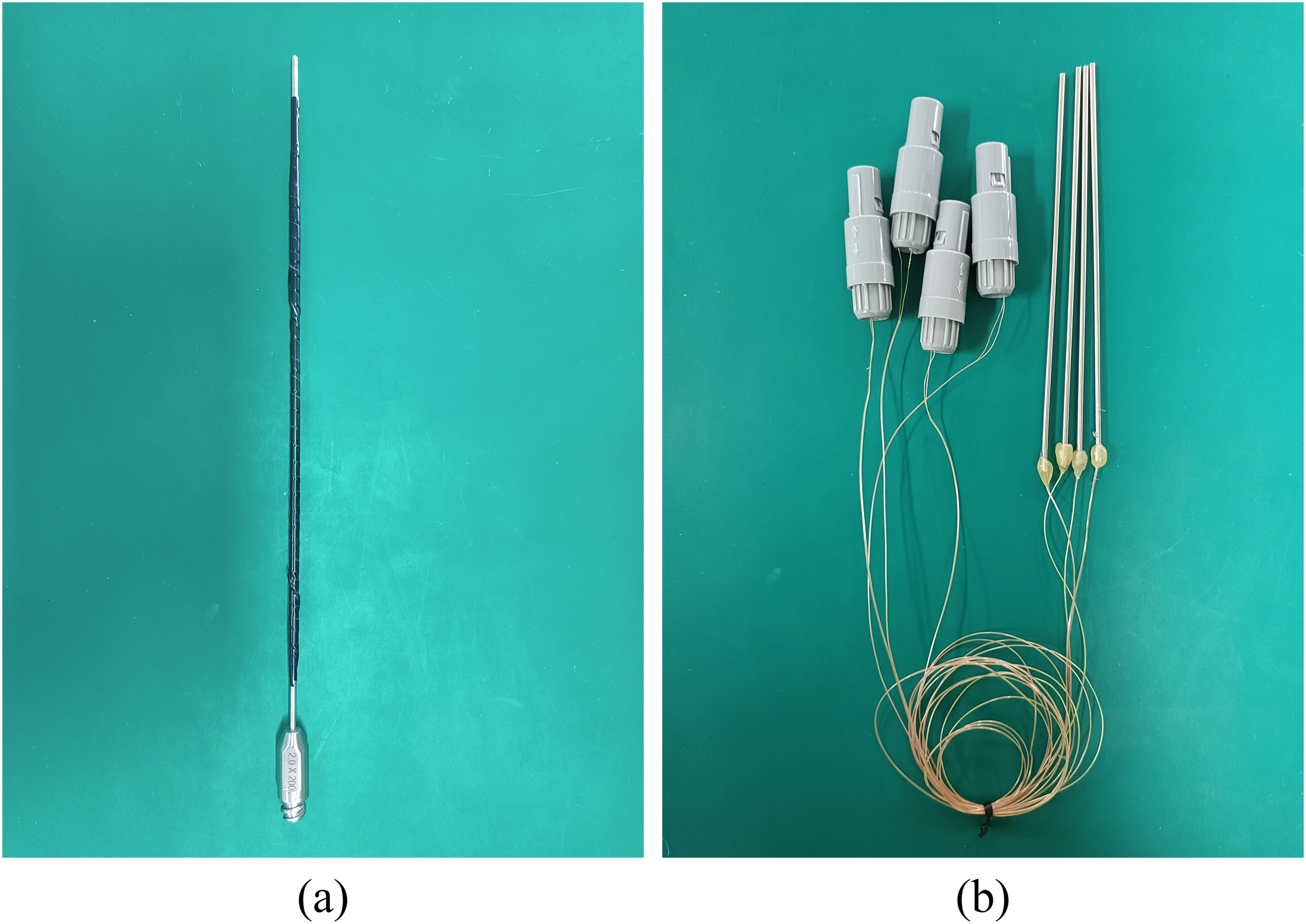
(a) Radiofrequency electrode needle (b) K-type thermocouples.
The experiments investigated the effects of radiofrequency ablation under constant power mode and controllable margin mode, using an ex-vivo bovine liver ablation platform, as depicted in Figure 8. A computer was employed to collect impedance and temperature data from the biological tissues, while an infrared thermal camera (FOTRIC 340, Texas, American)was used to capture the radiative temperatures of the ablation tissue cross-sections.

Diagram of the ex vivo bovine liver ablation experiment platform.
Results
Constant power radiofrequency ablation mode
Finite element simulation analysis of temperature distribution and changes in biological tissues
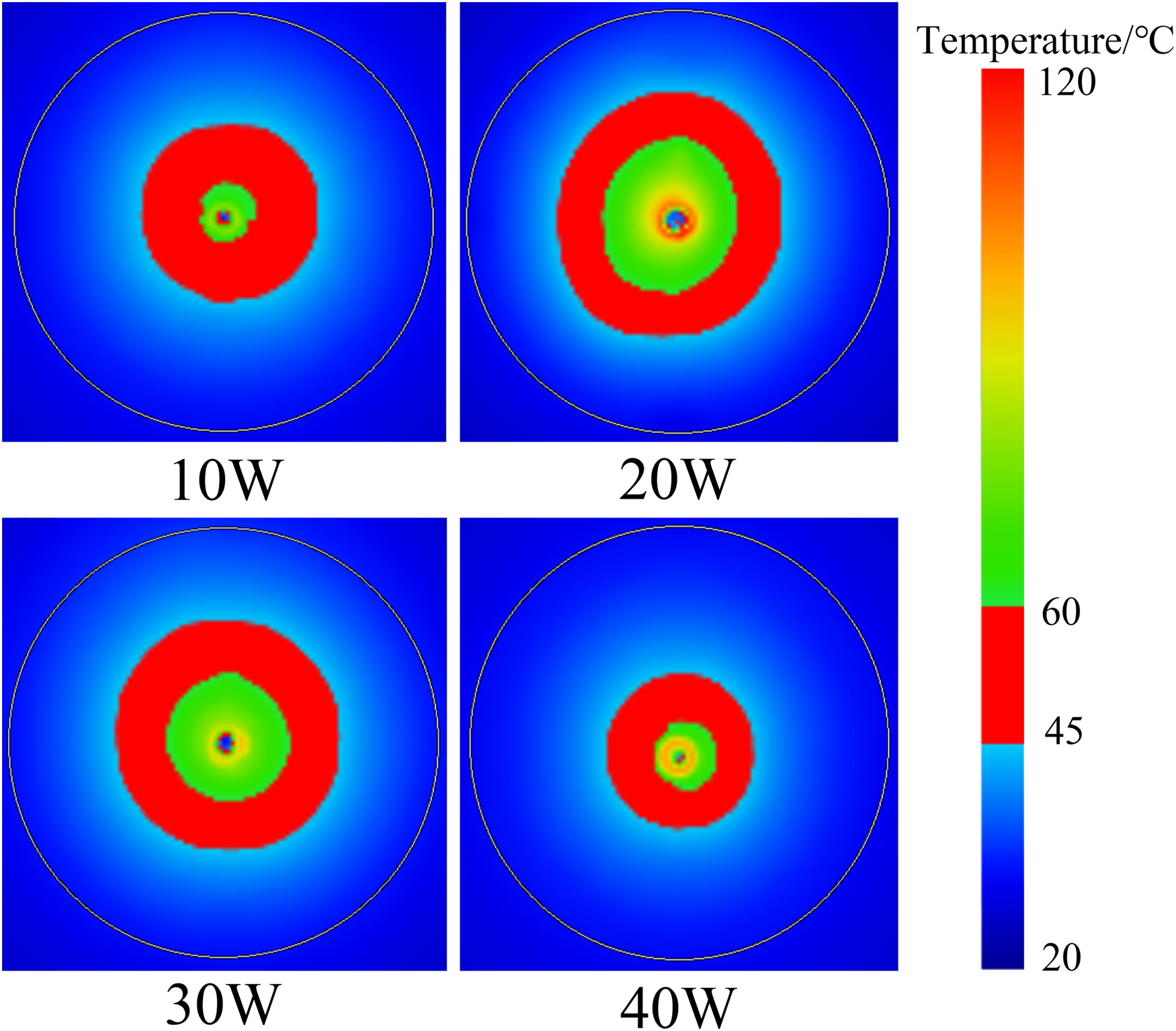
In the simulation study, tissue ablation was performed for 15 min using power settings of 10 W, 20 W, 30 W, and 40 W. The temperature distribution of the tissue is displayed in Figure 9. As the power increased from 10 W to 20 W, the area within the tumor where the temperature reached or exceeded 60°C significantly expanded. However, further increasing the power to 40 W resulted in a contraction of this area.
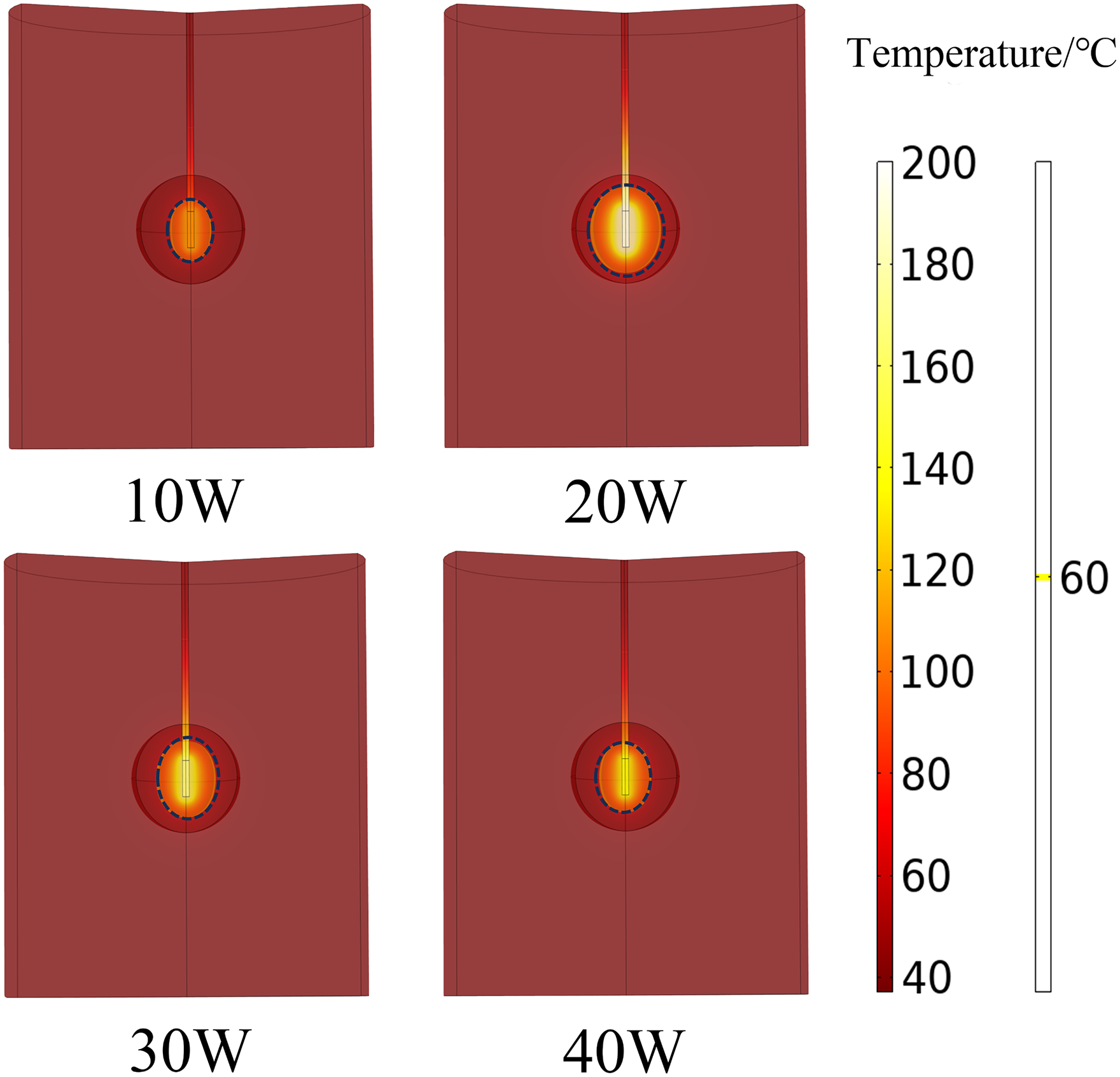
Temperature distribution of biological tissue in constant power ablation mode from finite element analysis (The area enclosed by the dashed lines in the figure indicates regions where the temperature is above 60°C).
Figure 10 shows the internal temperature changes of biological tissues at different power settings during the finite element ablation simulation. At 10 W, the tissue temperature rose slowly; by the end of the ablation, the temperature at 10 mm exceeded 70°C, at 20 mm exceeded 40°C, and at 30 mm exceeded 30°C. At higher power settings of 20 W, 30 W, and 40 W, the temperature at 10 mm rapidly increased. When the temperature exceeded 80°C, it suddenly dropped and then stabilized around 65°C until the end of ablation. The temperature at 20 mm quickly stabilized around 40°C, and at 30 mm, it initially rose rapidly before stabilizing. Notably, as the power increased, the stable temperature at 30 mm decreased; at 20 W, it exceeded 35°C, but at 40 W, it stabilized around 30°C.
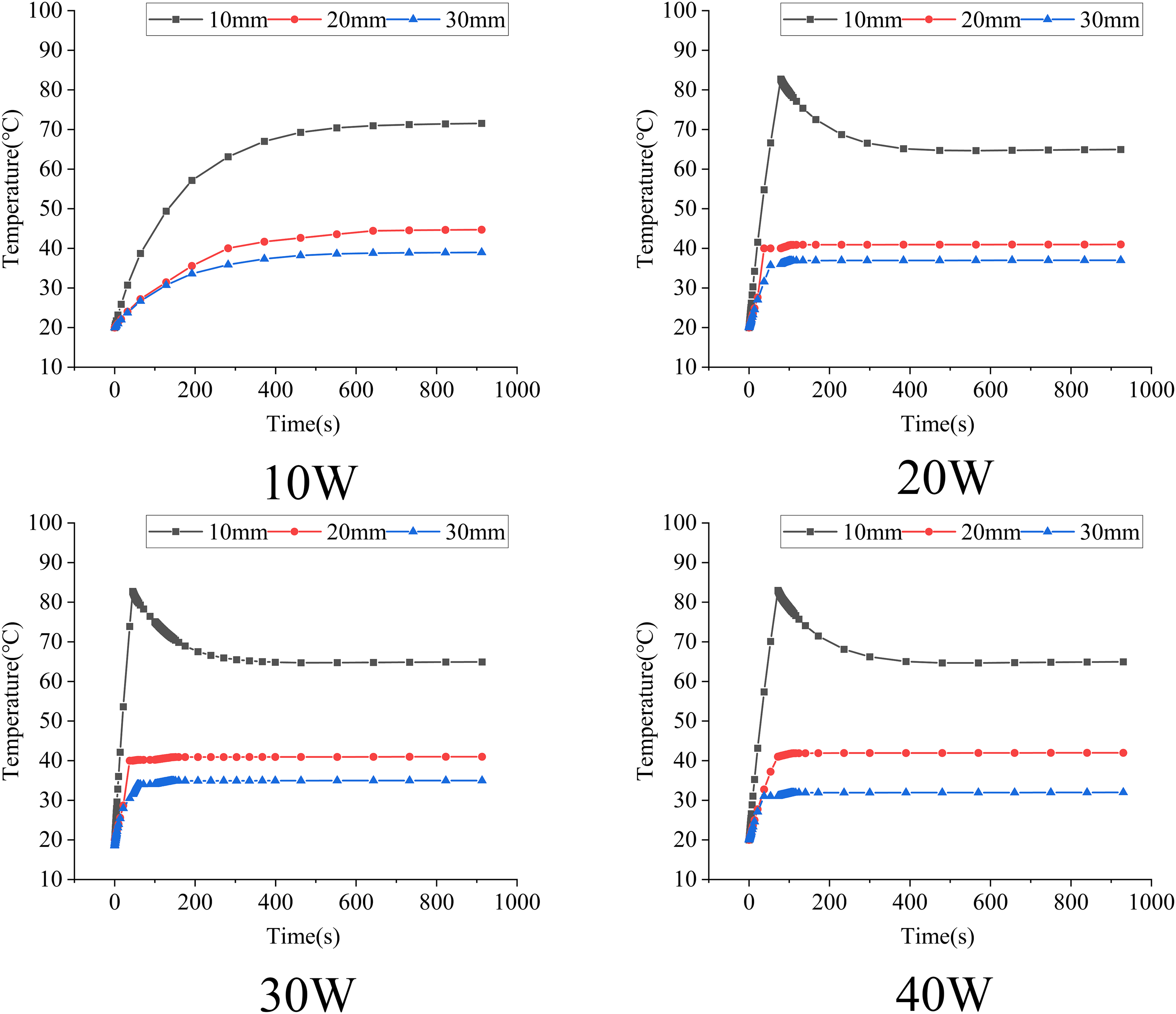
Temperature variation curve of biological tissue in constant power ablation mode from finite element analysis.
Temperature distribution and changes in biological tissues in ex-vivo bovine liver experiments
In the ex-vivo bovine liver ablation experiments, we examined the effects of output powers of 10 W, 20 W, 30 W, and 40 W. Each power setting was tested in five repeated experiments. Figure 11 presents the ablation cross-sections of the bovine liver tissue, with actual images and thermal distribution captured by the thermal camera.
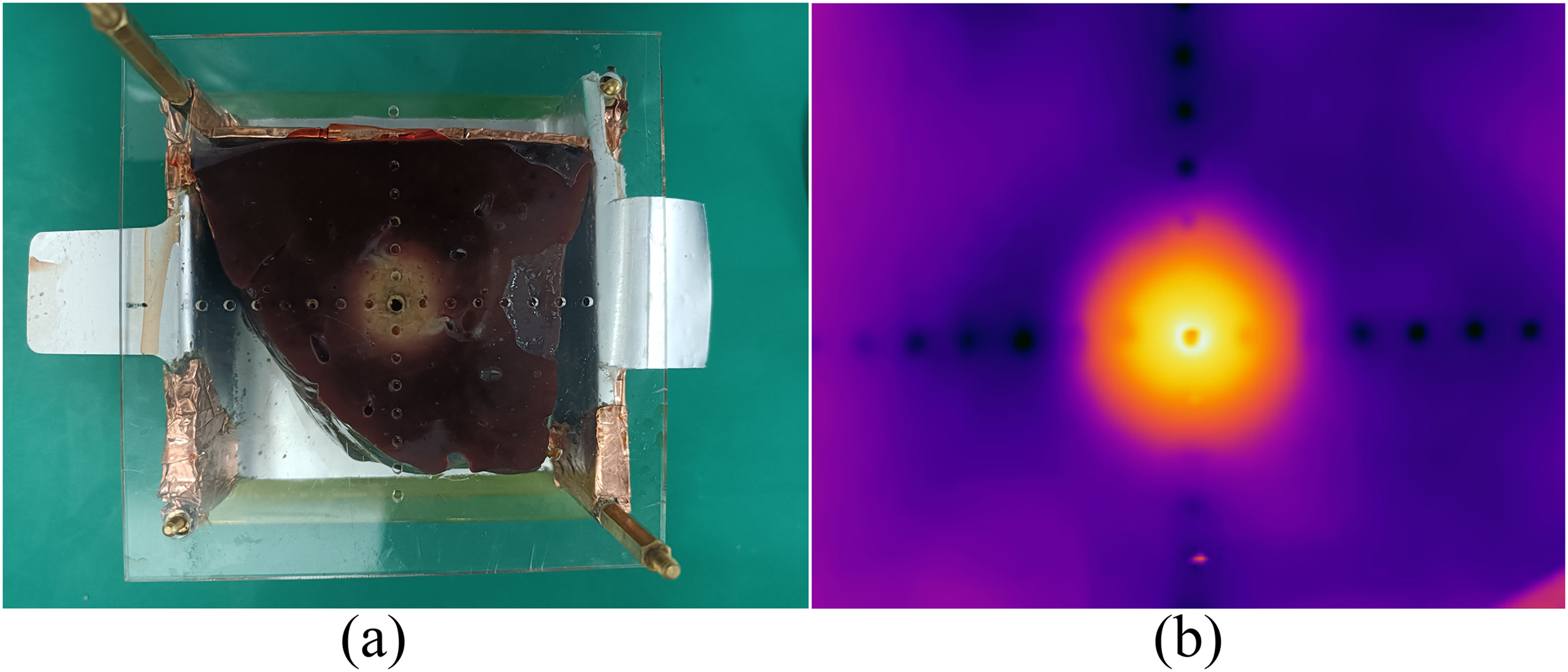
(a) Actual ablation cross-section of ex vivo bovine liver tissue (b) thermal image of tissue ablation cross-section.
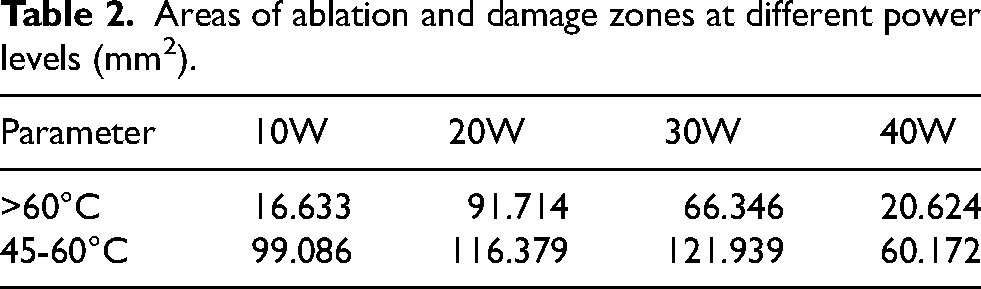
Figure 12 displays thermal imaging of bovine liver ablation cross-sections obtained at varying power levels, clearly delineating regions defined by 60°C and 45°C isotherms. Tissue within the 60°C isotherm exhibited complete necrosis and was designated as the ablation zone 22 ; tissue between the 45°C and 60°C isotherms showed partial necrosis and was thus referred to as the damage zone 23 ; tissue outside the 45°C isotherm retained biological activity, categorizing it as the undamaged area. 24 The distribution of tissue temperatures beneath the thermal images, at different output powers, is quantified in Table 2, revealing that the areas of ablation and damage initially increase and then decrease as the power output rises.
Temperature interface of bovine liver tissue in constant power ablation mode during ex vivo experiments.
Areas of ablation and damage zones at different power levels (mm2).
Temperature measurements inside the bovine liver tissue were taken using thermocouples, placed in the same positions as in the simulation. The temperature profiles, as shown in Figure 13, indicate that at 10 W, the temperature within the liver slowly rose, reaching over 70°C at a 10 mm diameter, over 40°C at 20 mm, and above 30°C at 30 mm. At higher power settings of 20 W, 30 W, and 40 W, temperatures at a 10 mm diameter rapidly increased to between 80°C and 90°C, then sharply decreased and stabilized around 60°C until the end of ablation.
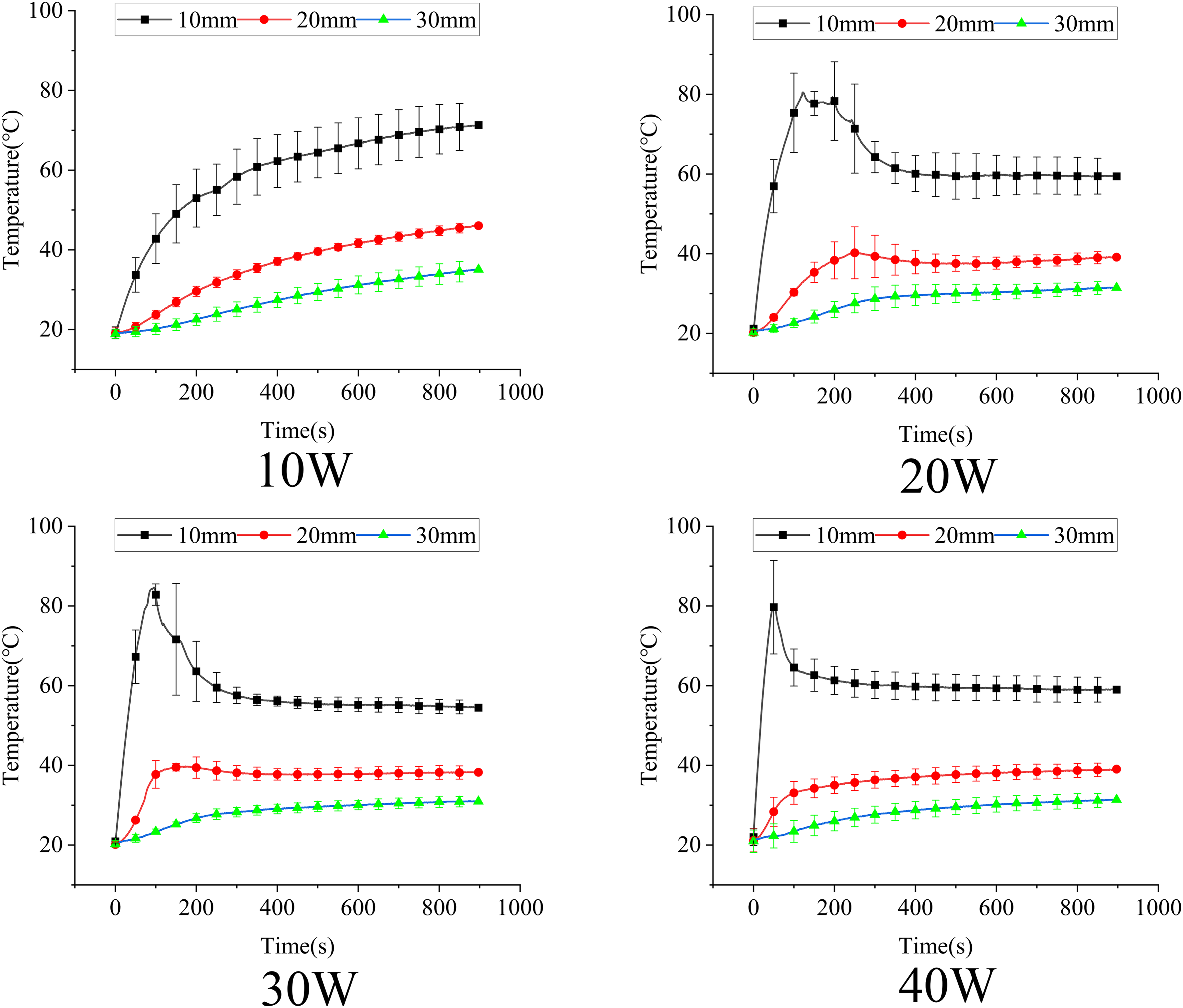
Internal temperature variation curve of bovine liver tissue in constant power ablation mode during ex vivo experiments.
Boundary-controlled temperature ablation mode
Finite element simulation analysis of temperature distribution and ablation margin temperature changes in biological tissues
To better understand the effects of ablation on biological tissues under controlled boundary conditions, this study conducted 15-min ablation simulations on tumor models with diameters of 10 mm, 20 mm, and 30 mm. Figure 14 shows the temperature distribution after ablation of tumors of different sizes. It was observed that for the 10 mm tumor, the 60°C isotherm extended slightly beyond the tumor itself; however, for the 20 mm and 30 mm tumors, the 60°C isotherm precisely matched the size of the tumors.
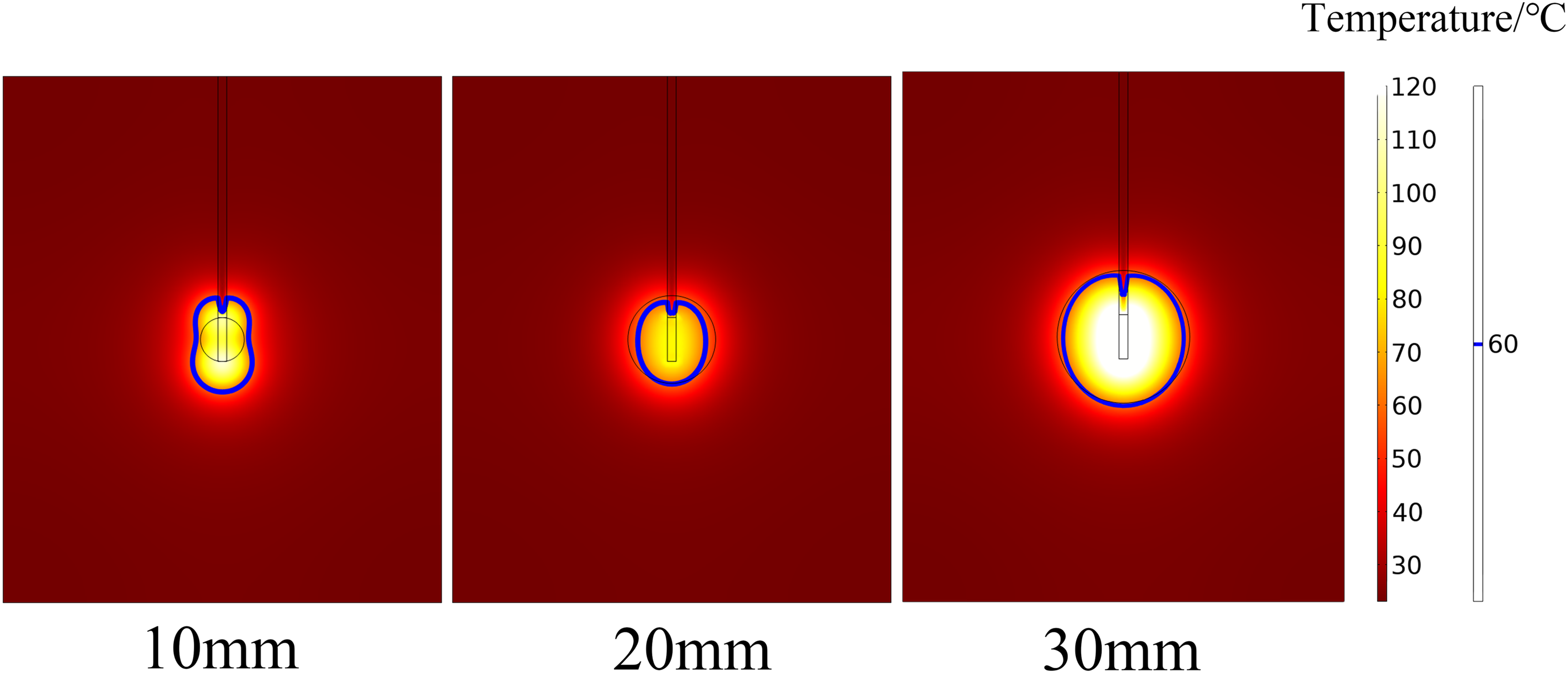
Temperature distribution of biological tissue in boundary temperature control ablation mode from finite element analysis (The area enclosed by the thick lines in the figure indicates regions where the temperature above 60°C).
Figure 15 illustrates the temperature changes at the tumor boundaries during the ablation process. For all three tumor sizes, the temperature trends began with an increase from the onset of ablation, followed by a decline after reaching a certain threshold, and then an increase again when the temperature dropped to 50°C. Notably, the 20 mm and 30 mm tumors began to cool once the temperature reached the 60°C threshold, whereas the 10 mm tumor displayed a variable cooling threshold, which showed a decreasing trend throughout the ablation process but consistently remained above 60°C.
Temperature variation curve at the ablation boundary in boundary temperature control ablation mode from finite element analysis.
Temperature distribution and ablation margin temperature changes in biological tissues in ex-vivo bovine liver experiments
This study employed a boundary-controlled adaptive power ablation algorithm to explore ablation effects on bovine liver tissue, specifically examining ablations of 10 mm and 20 mm diameters ex-vivo. Figure 16 presents thermal images of the ablated bovine liver tissues at these sizes. In the 10 mm diameter ablation experiment, the area where temperatures exceeded 60°C was less than 10 mm in diameter, while the region experiencing temperatures between 45°C and 60°C ranged from 10 mm to 20 mm. Additionally, temperatures at all four measurement points on the 10 mm boundary exceeded 50°C. For the 20 mm diameter liver tissue, the area with temperatures above 60°C had a diameter of about 10 mm, and the 45°C to 60°C zone extended from 20 mm to 30 mm, with temperatures at the 20 mm boundary also surpassing 50°C.
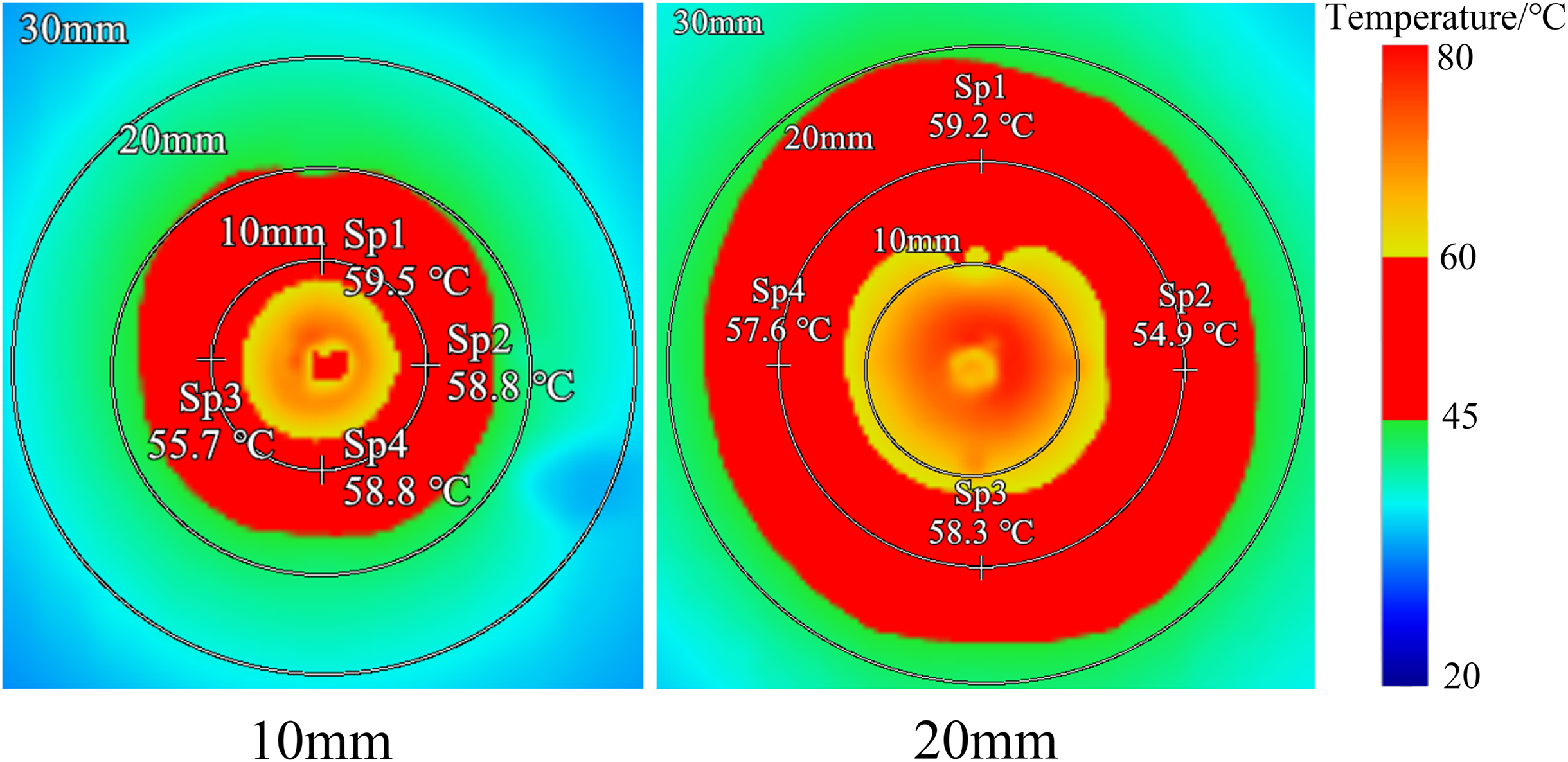
Temperature interface of bovine liver tissue in boundary temperature control ablation mode during ex vivo experiments.
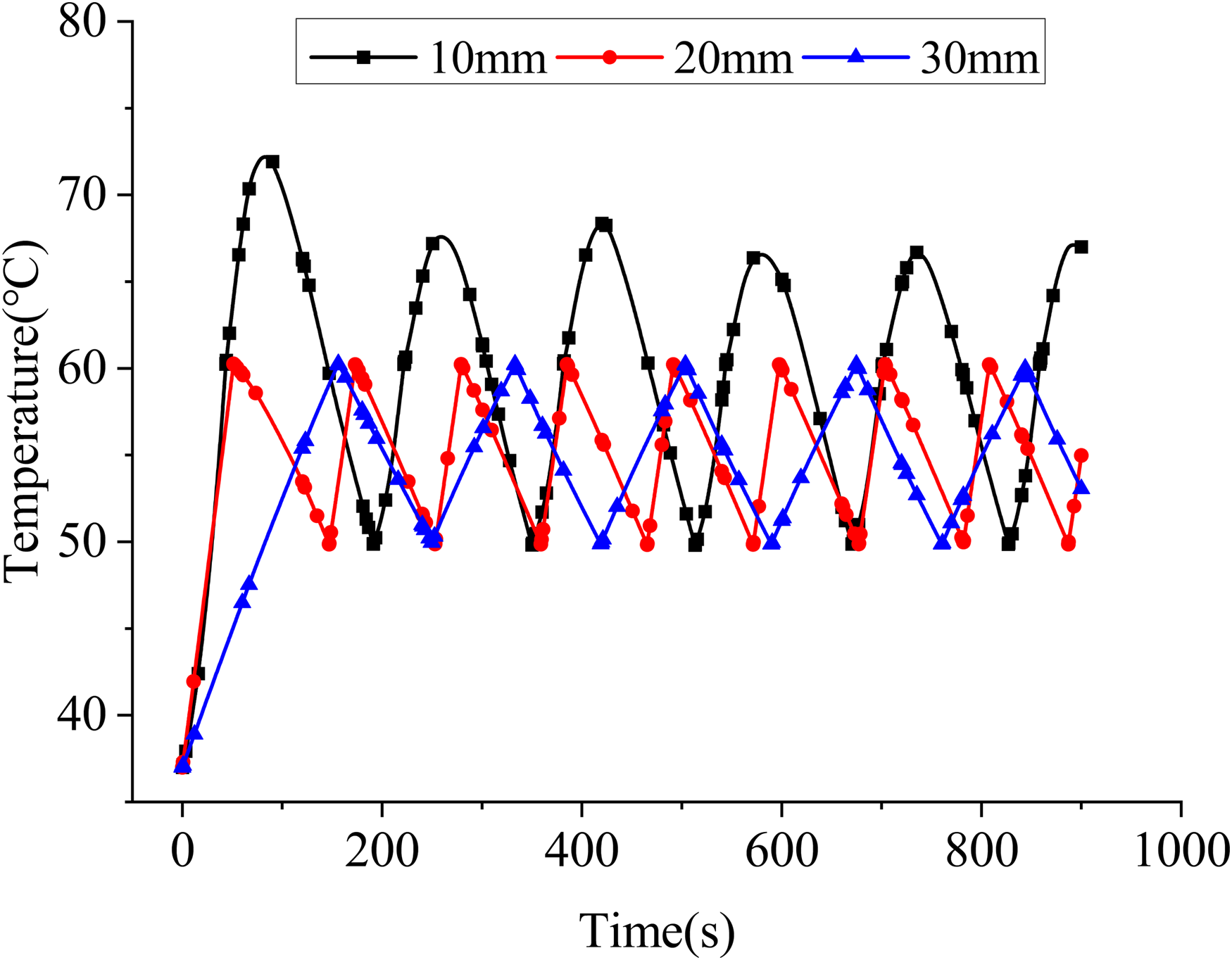
To ensure precise ablation, we evaluated whether tissue experienced irreversible damage based on the criterion of maintaining a temperature above 50°C for 2 min. Therefore, in the ablation experiments, we placed four thermocouples at the ablation boundary to monitor temperature changes. The placement of the thermocouples was consistent with the positions used in the simulations. Figure 17 demonstrates the temperature variations at the boundaries under different ablation sizes, revealing that the temperatures recorded by all four thermocouples at the boundaries of both the 10 mm and 20 mm ablation sizes reached 50°C and were sustained for 2 min.

Temperature variation curve at the ablation boundary in boundary temperature control ablation mode during ex vivo experiments.
Discussion
This study conducted finite element modeling simulations and ex-vivo bovine liver experiments to explore the effects of radiofrequency energy ablation at four different power outputs. Figures 9, 10, 12, and 13 present the simulation and experimental results, illustrating the temperature distribution and changes in biological tissues during the ablation process. These findings facilitate an analysis based on the temperature-dependent extent of tissue damage.
Observations from Figures 9 and 12 reveal that areas where temperatures exceeded 60°C initially expanded and then contracted as the power output increased, with the largest area observed at 20 W. It is noted that temperatures above 60°C cause immediate coagulation and irreversible cellular damage. 25 Therefore, the irreversible damage zone in constant power output ablation first increases and then decreases with rising power outputs. This phenomenon can be attributed to lower power outputs delivering less RF energy, resulting in smaller zones of irreversible damage and necessitating longer ablation times to achieve larger ablation areas. 26 At an optimal power of 20 W, the energy impacting the tissue interior increases, enlarging the zone of irreversible damage. However, at higher outputs of 30 W and 40 W, extensive RF energy leads to tissue charring, which impedes the transmission of RF energy, thus reducing the area of irreversible damage. Research by Lozano Granero et al. 27 on the effects of different powers on cardiac RF ablation confirms that higher powers result in smaller ablation volumes, while lower powers produce larger volumes.
Temperature variations inside the biological tissues, as shown in Figures 10 and 13, indicate that higher powers cause temperatures near the electrode to rise more rapidly and drop sooner, while tissues farther from the electrode exhibit lower and slower temperature increases, suggesting a link to biological impedance. 28 Figure 18 shows impedance changes in biological tissues under constant power ablation. At 10 W, the biological impedance decreases slowly, with no charring observed post-ablation. At increased powers of 20 W, 30 W, and 40 W, the impedance steadily rises to the hundreds of ohms and remains stable, with faster impedance increases correlating with higher powers and leading to tissue charring observed post-ablation. As the energy applied to the tissues is greater, charring occurs quicker, thus reducing the duration that RF energy can effectively interact with the tissues, thereby confirming our hypothesis that increased power paradoxically reduces the extent of tissue damage.
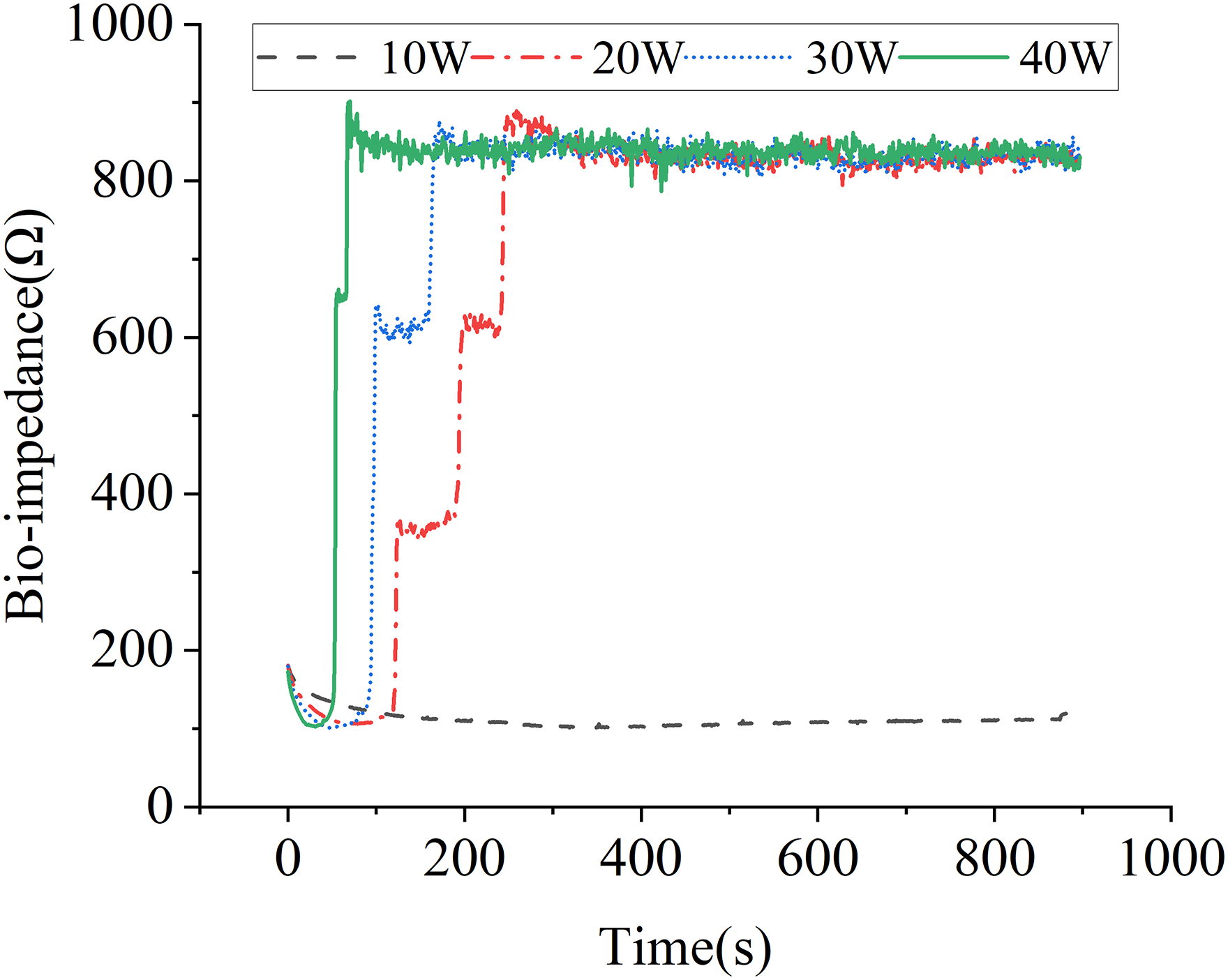
Bioimpedance variation curve in constant power ablation mode during ex vivo experiments.
In summary, the primary issue with the constant power ablation mode is its uncontrollability: both excessively low or high RF power can result in insufficient ablation of biological tissues, and the fixed power output cannot ensure the safety of the ablation, posing a risk of excessive ablation. 29 Developing controllable ablation techniques is crucial to ensure optimal ablation outcomes. Studies have shown that the temperature and impedance of biological tissues are significantly correlated with ablation efficacy11,30; many clinical trials involve controlling these parameters to enhance ablation results. Leshem et al. 31 conducted experiments using a temperature-controlled ablation technique, finding that this approach could increase ablation size while reducing the risk of steam pops. Lee et al. 32 evaluated the safety of a new automatic temperature-controlled endoscopic biliary radiofrequency ablation system in 30 patients, demonstrating its safety and effectiveness in treating biliary diseases. Fukushima et al. 33 treated 15 patients with hepatocellular carcinoma using an impedance-controlled radiofrequency interstitial thermal ablation system, showing superior results in ablation size and duration compared to traditional temperature-controlled methods. Furthermore, Glaiberman et al. 34 investigated factors affecting the size of the thermal effect zone in liver tumor treatments using an impedance-based radiofrequency ablation system in 42 patients across 59 RFA procedures. Their findings indicate that while most small liver cancers can be successfully treated with an impedance-based system, special attention is required for patients with conditions like cirrhosis.
To ensure complete ablation of tumors, this study successfully developed a controllable boundary ablation algorithm that adaptively adjusts the radiofrequency power output based on feedback from the temperature and impedance of biological tissues. The effectiveness of this algorithm was validated through both simulation models and ex-vivo bovine liver experiments, with results illustrated in Figures 14 through 17, showcasing the temperature distribution within biological tissues and changes at the ablation boundaries during the process.
Simulations based on the finite element model, depicted in Figures 14 and 15, demonstrated complete tumor ablation by precisely maintaining the boundary temperatures between 50°C and 60°C, particularly for tumors measuring 20 mm and 30 mm in diameter. However, for the 10 mm diameter tumors, the temperature at the boundary exceeded the preset threshold of 60°C, likely due to the proximity of temperature probes to the high-heat electrode, affecting boundary temperature control.
Further ex-vivo experiments on bovine liver tissues with 10 mm and 20 mm ablation diameters, illustrated in Figures 16 and 17, confirmed that the controllable boundary ablation algorithm effectively achieved tissue ablation within the target range, maintaining the boundary temperatures within the 50°C to 60°C range for at least 2 min, indicating irreversible damage had occurred. 12
Additionally, impedance monitoring during the experiments, as shown in Figure 19, revealed that the impedance first decreased, then increased, and spiked abruptly during the ablation process. Each spike was immediately followed by a reduction, effectively suppressing impedance throughout the ablation process by adjusting RF energy output to prevent charring.
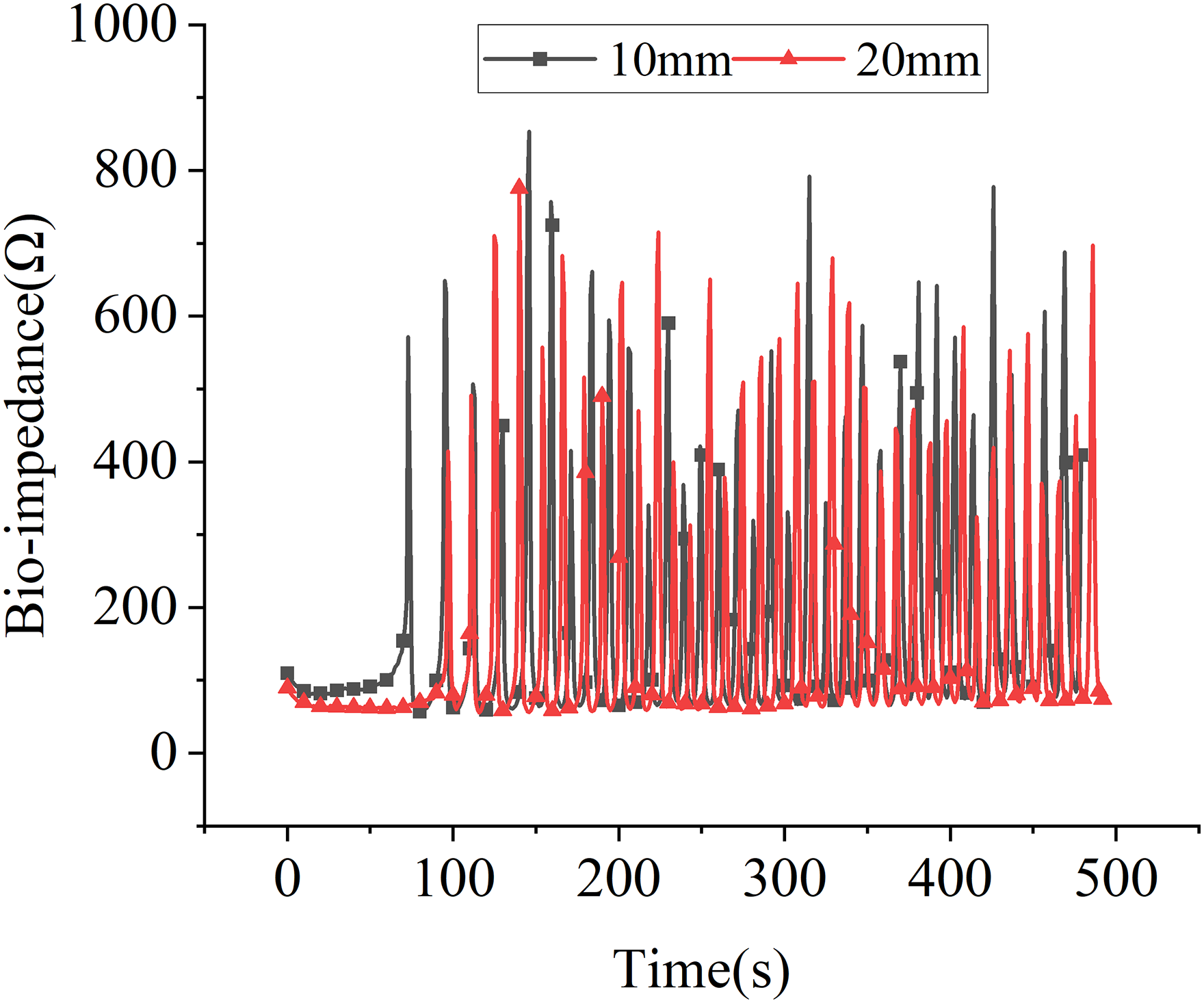
Bioimpedance variation curve in boundary temperature control ablation mode during ex vivo experiments
However, challenges were encountered when attempting to ablate larger bovine liver tissues of 30 mm diameter. The larger target ablation area required higher power outputs, which inevitably led to charring and subsequently hindered effective energy transmission, preventing adequate heating of the boundary tissues. Therefore, achieving the ablation of 30 mm tumors remains challenging under current equipment conditions.
This study aims to design an adaptive radiofrequency output algorithm to precisely control the ablation boundaries in tumor RF ablation procedures. We combined finite element simulation analysis with ex vivo experiments to validate the effectiveness of this algorithm in enhancing the accuracy of ablation boundaries. Numerous studies have investigated the issue of incomplete necrosis at lesion boundaries caused by RF ablation. For example, Thieme et al. 35 proposed the use of postoperative CT perfusion analysis as a precise tool to measure and visualize ablated liver lesions, allowing for immediate detection of incompletely ablated areas. Other studies36,37 suggested monitoring and controlling ablation temperature or impedance intraoperatively to expand the ablation area and reduce the risk of tumor recurrence due to incomplete necrosis of the lesion tissue. Unlike these studies, the equipment and ablation algorithm in this study were independently developed. Our approach comprehensively considers intraoperative variations in both tissue temperature and impedance. The adaptive RF output algorithm is designed to fully cover the target tissue while minimizing excessive ablation and unnecessary thermal damage, thereby improving boundary precision in HCC RF ablation. This algorithm effectively enhances the efficacy and precision of the RF ablation process, improves boundary control, and reduces the risk of residual tumor cells.
Notably, both the ablation algorithm and equipment used in this study were designed with safety considerations in mind. In the ablation algorithm, RF energy output is regulated by both tissue temperature and impedance: impedance regulation effectively prevents carbonization of tumor tissue, while temperature control ensures complete necrosis of the target tissue and minimizes excessive thermal damage. Additionally, the output section of the ablation equipment includes an isolation circuit that separates the applied and intermediate sections, ensuring safe device operation. The ablation equipment and algorithm used in this study are strictly limited to laboratory research and are currently being explored through ex vivo experiments. Only after further refinement in future studies will animal experiments and subsequent clinical trials be considered. Therefore, this study demonstrates a high degree of inherent safety.
Conclusion
This study developed an adaptive radiofrequency (RF) output algorithm for treating hepatocellular carcinoma, uniquely utilizing both temperature and impedance as feedback parameters for regulation. Initially, finite element analysis software was employed to model and simulate both the traditional constant power RF ablation mode and the algorithm-controlled ablation mode. Subsequent ex-vivo experiments on bovine liver validated these modes. The findings indicate that, compared to the traditional constant power ablation mode, the algorithm-controlled mode allows for precise control of the ablation area, significantly enhancing the efficiency and safety of the ablation process.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.