
Abstract

Introduction
The launch of the term clinical governance in 1998 sought to place quality at the centre of NHS reforms. The Royal College of Nursing maintains that clinical governance aims to integrate all the activities that impact on patient care into one strategy. This strategy involves improving the quality of information, promoting collaboration, team working and partnerships, as well as reducing variations in practice, and implementing evidence-based practice.
This section aims to bring together all of those key aspects and considers what they mean for a practice manager. Increasingly, the practice manager needs to understand aspects of the clini-cians’ work that used to be entirely in doctors’ hands, while GPs need to respect the practice manager’s responsibility for the outcomes of their work. Clinical governance forms the majority of the key lines of enquiry in Care Quality Commission (CQC) inspections of general practice in England and in similar inspection or peer review schemes in Scotland, Wales and Northern Ireland.
The title of the section has evolved from ‘Quality’ into ‘Clinical governance’ as the authors have come to appreciate that this term must underpin all working practices.
What is clinical governance? What does it really mean?
The term clinical governance was first defined in the 1998 consultation document ‘A First Class Service: Quality in the New NHS’ as: A framework through which NHS organisations are accountable for continuously improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish. (http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/publicationsandstatistics/publications/publicationspolicyandguidance/dh_4006902)
It is a term that has proved to be not just an initiative but more a philosophy … and a phi-losophy that should underpin all working practices. It is also a very broad term that has been interpreted in many different ways, but fundamentally it is about ensuring accountability and safe medical practice. The idea of clinical governance and ensuring a minumum expected level of quality in primary care was taken forward in 2003 by the introduction of organisa-tional domains in the Quality and Outcomes Framework (QOF), which expected certain standards on education and audit. But the QOF was technically voluntary. In 2013 these QOF indicators ceased, but from April 2013 there was a statutory obligation for practices to register with the Care Quality Commission (CQC) who expect many of the standards outlined in this chapter. This will be discussed further later in the chapter.
The key components and themes of clinical governance include:
patient, public and carer involvement
strategic capacity and capability
risk management
staff management and performance
education, training and continuous professional development
clinical effectiveness
information management
communication
leadership
team working.
Quite simply it’s a system for improving the standards of clinical practice. It is important, however, that the philosophy does not just touch clinicians as it is a principle that all members of the practice should buy into, right through from the partners, who should show leadership, to the cleaners who are there to provide a safe and clinically clean environment in which to provide medical care.
The specific topics listed above are considered in this section or in other parts of the Handbook of Practice Management, and these will be cross-referenced where necessary.
Clinical governance and the practice manager
The practice manager is key in instilling the principle of clinical governance into everyday organisational practice. The practice manager is often the registered manager for CQC registration. It is a requirement for every practice to have a clinical governance lead, and the practice manager may take this role, but in these cases clinical support is always best practice.
You should create the appropriate policies and procedures on which to base working practices that embrace the principles of clinical governance. Your policy should cover the key elements as outlined above and explain who will be responsible for delivering and monitoring them. Advice on such policies can be found through national organisations, but also through practice manager networks.
It is envisaged that the practice manager will be responsible for the following areas that incor-porate clinical governance:
maintaining audit activities and ensuring that the results are disseminated throughout the practice
ensuring that Significant Event Anaylsis is in place and that clinical governance meetings are arranged
developing robust IT systems that can produce appropriate data
developing personal leadership skills and supporting others to do the same
welcoming a no blame culture so that ideas can be shared and ownership of those ideas belongs to the whole team.
Significant Event Analysis provides a perfect opportunity for the whole team to discuss events that have touched the practice, and discussions stemming from significant events will no doubt comprise the entire list of the key elements that our umbrella term of clinical governance covers. It is about setting the right culture and climate within which to work. It should be a climate of support and challenge where people are encouraged to share information in order that lessons may be learned and beliefs are shared with the whole team. For more information on significant event analysis see page 6-17.
Further information:
— Department of Health. A First Class Service, Quality in the New NHS. London: DOH, 1998
— Royal College of Nursing. https://www.rcn.org.uk/clinical-topics/clinical-governance
Clinical governance, the practice manager and the GP
The GP delivers the clinical care but the practice manager has a role in ensuring that the practice’s clinicians are safe practitioners. The practice manager is responsible for the administrative aspects of care, but the GP is often the practice manager’s employer and has at the least a strategic role in the way the practice is run. This entwined relationship works well in practices with open cultures, flat hierarchies, and good teamwork and personal relations, but can be difficult if the roles and responsibilities and relationships have not been clarified.
The practice manager has a responsibility for ensuring that doctors are fit to practise safely. Clinicians need an environment that permits them to do their job properly; they need to keep up to date, and they need to have a work–life balance that allows them to devote an appropriate amount of their personal resources to their work. The practice manager usually has authority to ensure the first of these, but problems with the second and third can be difficult to handle.
Continuing professional development (CPD) and ‘Revalidation’ is an obligation for GPs (see page 5-18), and their annual appraisal (see page 2-61) should in theory pick up problems with their CPD, their health, and other personal problems that bear on their professional perfor-mance. But appraisal is a formative process, not performance management. Furthermore, the appraiser may not pick up a problem, and unless a doctor’s performance is recognised as threatening patient safety, only the appraisee has access to the report and recommendations. Even with revalidation in place, there are ways that a practice manager can increase the chances of picking up problems, such as checking that doctors are taking study leave, and adopting a cor-porate approach to building up GPs’ appraisal portfolios and shared learning plans. Practices may decide that doctors should have an in-house appraisal as well as the primary care organisation (PCO)-organised one. The CQC expects that regular checks are made to ensure that indemnity cover is in place, immunisations are up to date and there are no General Medical Council (GMC) restrictions on the practice. But the best protection is an open, supportive culture in which doctors, even the senior partner, feel able to share problems with colleagues and the practice manager.
For information on the management of sick and poorly-performing doctors see page 2-09.
The practice team and clinical governance
It is important to consider how the practice team can contribute to your quality standards. Quality standards should not be imposed if they are to be successful. They should be embraced and upheld by the entire team. The key to ensuring that the principles are indeed embraced is of course involvement in setting those standards and excellent communication throughout the team. Strong leadership is also key to embedding the standards you are aiming for, as quality undoubtedly starts at the top with the attitudes of the partners and the managers. It is essential that they demonstrate those standards by their actions and behaviour. With these key leadership skills, strong communication links and involvement in the setting of standards there is every possibility that the team will believe in its value and continue to improve its performance.
The reception team, for example, is the gateway to your organisation. Team members who know their worth and know what is expected of them will be an invaluable first point of contact to your practice and an asset to the organisation, as they will provide the patients with confidence that this practice can indeed provide an appropriate service to its patients, i.e. good customer service. After all, that is exactly what our patients are – customers, who have the freedom to take their custom elsewhere if our quality standards don’t meet their expectations. Of course some of their expectations may be unrealistic, but what we are referring to are the fundamental principles of customer service.
How should the aims and objectives be defined and communicated?
Sharing the vision: Holding a meeting for the entire team including attached staff is an excellent way to discuss what the practice is trying to achieve and why. An away afternoon at local hotel, for example, can provide the relaxed atmosphere required to be conducive for discussing the vision, sharing ideas and debating the opportunities presented. This can have cost implications in terms of getting an Out-of-Hours provider to cover the afternoon, but the long-term benefits of this action may make the investment cost-effective overall.
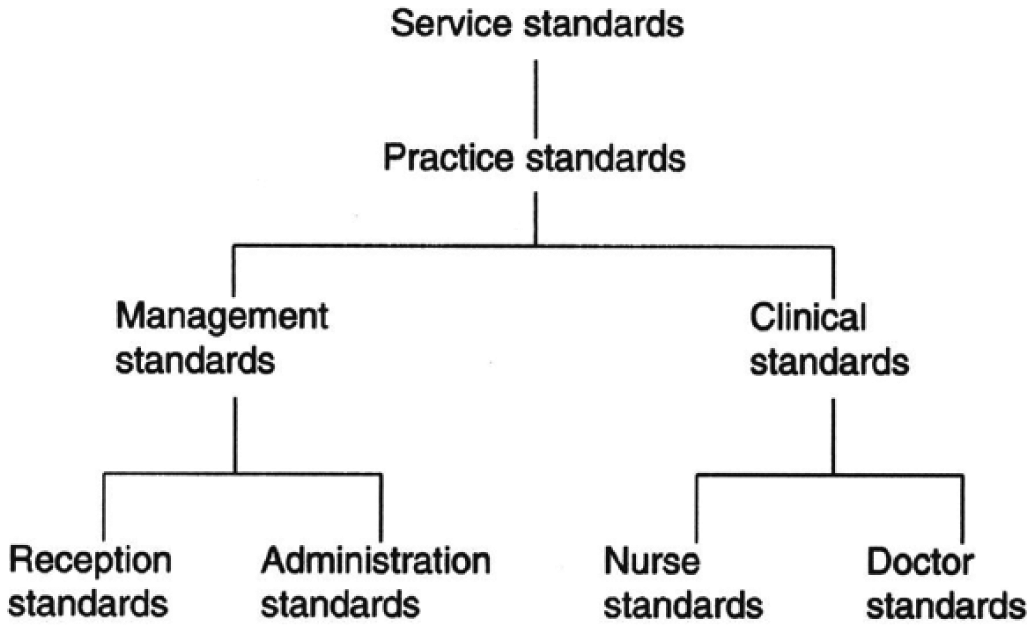
Quality standards
Preparing a written statement: Preparing a written document outlining your key objectives will undoubtedly provide benefits as the process of committing ideas to paper leads to clarification and formality. It also ensures that everyone receives the message in exactly the same way and that there can be no misunderstanding about what has been debated, agreed and is therefore now expected. The CQC call this a statement of purpose document and it is expected to be seen during inspections.
Maintaining quality standards
As mentioned in the preceding paragraphs, quality standards have to start at the top, but as we have discussed, in order to be effective the principles have to cascade throughout the entire team. In addition, some quality standards will be initiated from outside of your immediate team. The National Institute for Health and Care Excellence (NICE), for example, is responsible for providing national guidance on promoting good health and preventing and treating ill health.
The cascade therefore begins outside of the practice at a national level, ending internally with each individual team member.
Management standards
Perhaps the most high profile quality standards to hit the practice manager’s desk over the last two decades have been via the QOF. Even with the removal of the organisational domains (see Chapter 3 for more details), the clinical domains of the QOF still require intense input from the practice manager to put in place systems to capture the relevant clinical information and systems for recall. Compsulory CQC registration from April 2013 covers many of the areas lost through the QOF organisational domains and includes new standards. This is discussed later in the chapter.
There are also independent rewards for organisations that ascertain a defined level of achieve-ment. Aspiring to one of these external quality standards can be a huge motivator for the partners and staff alike, and an excellent achievement for the manager who feels that the hard work that comes with establishing the required culture and climate has paid off. An example of such an award is the Quality Practice Award developed by the RCGP.
Further information:
— Lyndsay Swinton. Mind Tools. 30 December 2004 Newsletter. www.mindtools.com
— National Institute of Health and Care Excellence. www.nice.org.uk
Quality outcomes in general practice
Within the NHS there are increasing demands for accountability and improvements in quality of care. In general practice the outcome measures used to judge ‘quality of care’ are a matter of some debate. Possible measures are patient satisfaction, patient concordance or compliance, prescribing rates, patient recall, referral rates, doctors’ ability to detect illness and performance against pre-set targets. These are discussed in the following.
Patient satisfaction
What is satisfaction?
Satisfaction is defined in the dictionary as ‘giving (a person) what he wants or demands or needs’. There is some debate about the meaning of satisfaction scores as outcome measures in healthcare settings. In the context of medical care, satisfaction is a reflection of both the needs and the wants of the patient, and is therefore a measure of both the actual care received and a reflection of the person responding to the question. Five elements determine satisfaction with medical care:
occurrences or realities – the events that actually occurred and the individual’s perceptions of them
value – evaluation in terms of good or bad, of the service received
expectations – beliefs about the probability of certain attributes being associated with certain events or objects and perceived probable outcome of those associations
interpersonal comparisons – an individual’s rating of the healthcare received based on either direct (his own previous experiences) or indirect (comparison with care received by someone else known to the patient) comparison with previous experiences
entitlement – a person’s belief that he has proper, accepted grounds to certain services or outcomes.
The components of care thought to have most influence on patient satisfaction are: availability of care; technical quality of care; accessibility and convenience; efficacy or outcome of care; continuity of care; and physical environment. In UK healthcare settings (general practice, hospital inpatients and dentists’ patients), independent of medical context, the most important factors determining patient satisfaction are professional competence and quality of the relationship between the patient and healthcare provider.
Two aspects of this relationship between healthcare provider and patient – empathy and communication – are particularly important in determining satisfaction.
Determinants of satisfaction
Expectations of care that should be received have a fundamental role in the expression of satisfaction. Therefore different levels of satisfaction do not necessarily imply different levels of quality, but may reflect different perspectives on quality. For example, the more a doctor’s performance meets a patient’s expectations, the more satisfied the patient will be, and patients with lower expectations tend to be more satisfied.
Expectations change with knowledge and experience. For example, increasing quality of care raises expectations. Thus ultimately higher quality of care may be associated with lower levels of satisfaction.
A common factor in many patient satisfaction surveys is that very few patients express dis-satisfaction or are critical of their care. In UK general practice overall satisfaction rates of over 80% have been consistently reported over the past 30 years, but anyone sitting in a general practice waiting room for any length of time will hear adverse comments, suggesting that satisfaction levels are considerably lower than this in reality. There are many reasons for this:
Patients report greater satisfaction than they actually feel because they believe positive comments are more acceptable to survey administrators.
Patients are reluctant to complain for fear of unfavourable treatment in the future.
If patients are using a service and need that service, expressions of satisfaction will contribute to the continuation of the service, which in turn is in their own self-interest.
Patients are likely to report satisfaction as a way of justifying the time and effort they themselves have put into a programme of care.
Additional attention implicit in giving the patient a survey form to complete, and the apparent concern for the patient’s views, are likely to increase satisfaction regarding a particular service being asked about (though the reverse could also be argued).
Patients generally feel grateful for the care and attention that they have received. They tend to try to be cooperative and positive about the services they receive. Expressing dissatisfaction would appear ungrateful.
Patients feel that problems will not be remedied either because they are too small and thus deemed trivial by the patient or because the problem is just too large to change. There is therefore no point in commenting on them.
As a result of the high levels of overall satisfaction consistently seen, there is a tendency for satisfaction scores to respond poorly to change. A way around this problem is the ‘discrepancy model’. This shifts the focus from analysis of overall levels of satisfaction to concentrating on areas of expressed dissatisfaction. It has been shown that if patients are asked more specifically about different components of care (e.g. information provided or communication), significantly less will be completely satisfied. These areas of dissatisfaction can be used to improve care.
There has also been some concern that satisfaction levels reflect characteristics of the people interviewed and not the care provided. For example, depressed patients tend to be less satisfied with care provided than happy patients, and older people tend to be more satisfied with care than younger people. There is evidence for this not only in the UK (where it can be argued that older people’s expectations are different as they remember pre-NHS days), but also in other countries throughout the world.
Purpose of measuring satisfaction
Measurement of satisfaction fulfils several distinct functions:
understanding patients’ experiences of healthcare
identifying problems in healthcare and generating ideas towards solutions
evaluation of healthcare – comparing a service against a set of standards deemed to be acceptable.
Measurement of satisfaction in UK general practice
Questionnaires often have low validity and reliability. Nevertheless, satisfaction measures are increasingly being used to judge the effectiveness of the NHS. In the surgery, patient sat-isfaction audits, such as audits of the appointments system, are a useful way of identifying deficiencies in the system from the user’s perspective. As part of the QOF organisational domains in 2004, practices were expected to carry out an in-house survey covering areas including access, and develop action plans based on these results. Such surveys included the General Practice Assessment Questionnaire (GPAQ). The QOF points were for carrying out the survey and developing action plans, rather than for the results themselves. In 2008 these in-house surveys were replaced by an independent national scheme carried out by IPSOS MORI. With this scheme, the QOF points achieved were dependent on the level of patient satisfaction with access, although other aspects of care were also surveyed. This national survey continues, but since 2012 has no longer been part of the QOF. But it will continue to be used to aid PCOs in understanding patient access issues and wider aspects of care. In addition the data will be available to patients for them to compare practices. In 2015 the Friends and Family Test, that has also been applied to hospital and mental health providers, became a contractual obligation in general practice. The test asks the following standardised question: “How likely are you to recommend our ward/A&E department/GP Practice to friends and family if they needed similar care or treatment?” Patients then use a descriptive six-point response scale to answer the questions with the following response categories:
1 Extremely likely 2 Likely 3 Neither likely nor unlikely 4 Unlikely 5 Extremely unlikely 6 Don’t know
The score is calculated by subtracting the proportion of respondents who would not rec-ommend (response categories: “neither likely nor unlikely”, “unlikely” and “extremely unlikely”) from the proportion of respondents who would be extremely likely to recommend (response category: “extremely likely”). This produces a score from −100 to +100. It is thought such a simple measure will allow more easier comparison for patients between practices. The test can be completed by handing out slips after consultations, through text messages and via practice websites.
Further information:
— National GP Patient Survey - http://www.gp-patient.co.uk
— Friends and Family Test - https://www.england.nhs.uk/ourwork/pe/fft/fft-guidance/
Despite these national initivates, practices still often carry out in-house surveys for added value and in particular to aid them in their Patient Participation Groups.
Two practices share the same health centre. The blue practice with two doctors has opted to use the ‘consultation’ version of the GPAQ as it is designed to allow individual assessment of doctors. They will then combine the results to produce information about the practice overall. The red practice wants a more general overview of the quality of care that they provide and so has opted to use the postal version of the same questionnaire.
The blue practice
As the survey is being carried out in the surgery when patients come for appointments, one of the reception staff is given the task of collecting together 20 clipboards and 50 pens for patients to use when completing the survey and making a suitable box in which patients would be able to confidentially return their questionnaires. Another is given the task of displaying a poster in the waiting room informing patients that the survey is being carried out. Another is given the task of preparing some stamped envelopes with the practice address on them for patients to return questionnaires in, if they do not have time to stay and complete them after their consultation.
As the list size for the practice is 4000, it is calculated that 100 completed surveys will be needed, so 120 copies of the survey are photocopied. The questionnaires are then numbered. Fifty questionnaires are marked for patients seeing Dr Philips, and fifty for patients seeing Dr Andrews (regardless of whether that doctor is the registered doctor of the patient).
On the day of the survey, patients are told about the survey and what it is measuring (i.e. the patients’ views of the practice and the quality of care they receive from their GP) when they book in at reception, and are asked if they could stay behind for a few minutes to complete the questionnaire when they have seen the doctor. The survey is offered to every patient booking in, as long as the patient is over 16 years of age and registered with the practice.
Receptionists are instructed to remind people about the questionnaire on their way out. If patients can’t wait, they will be given a stamped addressed envelope to return the questionnaire in.
The red practice
A hundred patients nominally registered with each doctor in the practice are randomly selected by the computer. Deborah, a member of the office staff is then allocated the task of checking the list to ensure that the patients are over 16 years of age, still registered with the practice (and have not moved away or died), and are suitable for inclusion in the survey (i.e. do not have dementia, or are otherwise unable to complete the survey). A note is made to obtain appropriate foreign language versions of the GPAQ for the three patients selected who do not speak enough English to complete the questionnaire. Once a list of suitable patients has been generated, Deborah is asked to label each questionnaire with a number linking the patient’s name to the questionnaire.
Meanwhile, the doctors and practice manager get together to compose a letter to be sent to patients inviting them to participate in the survey. This letter states that the practice has given full support to the survey, that doctors and nurses will not be able to identify individual patients from the responses and that, whatever views the patient expresses, these will not affect future care. As Deborah has been given the task of running the survey, her contact details at the practice are also included in case patients have any questions about the survey.
Then Deborah sends a numbered questionnaire, a copy of the letter and a stamped envelope completed with the practice address to enable the questionnaire to be returned to the practice, to each patient on the list. When questionnaires are returned, she identifies them by the number on the questionnaire, and ticks them off on her list of questionnaires sent out.
After two weeks only 35% of questionnaires have been returned. Deborah generates a new list of patients who have not returned their questionnaires and sends them a reminder letter by post. Two weeks later the total returned has only risen to a disappointing 45% so she telephones all those patients with contact numbers who have been sent questionnaires but not returned them. This brings the total number of questionnaires returned to 310, or 62% of the total surveyed.
Further information;
— Carter M, Roland M, Bower P, Gask L, Greco M, & Jenner D. Improving your practice with patient surveys. Available from http://www.gpaq.info/patientsurveyhandbook.pdf
— For general advice on patient surveys see page 8-58.
Patient concordance or compliance
Another measure of the effectiveness of a consultation is the degree to which the patient com-plies with advice and uses medication supplied as directed. Patient concordance (or rather lack of it) is a major challenge in general practice. In general practice around one in three patients follow advice closely enough to make it effective; one in three follow some advice but not closely enough to make it effective; and one in three follow no advice at all.
Consequences of non-concordance are: 1) failure to attain therapeutic targets, for example failure to take antihypertensive medication reduces the number of strokes; and 2) wastage of precious resources. Around £300 million worth of medicines are returned to pharmacies each year for disposal – the true quantity wasted is many times that (http://www.medicinewaste.com).
Causes of non-concordance
Patient beliefs are the strongest predictors of compliance with advice and medication. For drugs, how natural a medicine is seen to be, the dangers of addiction and dependence, and the belief that constant use may lead to reduced efficacy have all been shown to influence compliance.
Lifestyle choices are also important. Patients will not follow advice if it causes them inconvenience or they cannot see that it will have any benefit. For example, drugs with once daily or twice daily dosage are more likely to be taken than those prescribed more frequently. Unpleasant side effects of treatment will also reduce concordance, especially if patients are not forewarned.
Another factor that influences whether the patient follows the recommended course of action is whether the patient understands the condition being treated and instructions given. This can be a particular problem if there are language barriers. Printed information available in other languages can be helpful. Practical factors, such as forgetfulness or inability to open containers, can also influence concordance.
Finally, professional factors can affect the degree to which advice is followed. For example, there is a link between patient satisfaction with a consultation with a doctor and subsequent concordance with treatment. Inappropriate prescribing and mistakes in administration of the treatment or dispensing mistakes can also affect patient confidence and thus decisions to fol-low advice.
Improving concordance
Around 70% of patients want to be more involved in decisions about treatment (http://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/people-in-control-of-their-own-health-and-care-the-state-of-involvement-november-2014.pdf). Doctors underestimate the degree to which they instruct and overestimate the degree to which they consult and elicit their patients’ views. The doctor’s task is, by negotiation, to help patients choose the best way to manage their problem. Patients are more likely to be motivated to follow advice when they:
understand and accept the diagnosis
agree with the treatment proposed
have had their concerns about the treatment specifically and seriously addressed.
Ways to improve concordance:
— Use simple language and avoid medical terms.
— Discuss reasons for treatment and consequences of not treating the condition, ensuring information is tailored, clear, accurate, accessible and sufficiently detailed.
— Seek the patient’s views on their condition.
— Agree course of action before referring or prescribing medication.
— Explain what the treatment is, its function and (if known and not too complex) its mechanism of action.
— Keep the regime suggested as simple as possible.
— Seek the patient’s views on how they will manage the regime within their daily schedule and try to tie treatment in with daily routines (e.g. ‘take your tablet in the morning when you get up’). It may be necessary to consider religious views, e.g. not prescribing gelatine capsules for Muslims and tailoring regimes to comply with the Ramadan fast.
— Discuss possible side-effects of treatment (especially common or unpleasant side-effects).
— Give clear verbal instructions and reinforce verbal instructions with written instructions if the regime is complex, the patient is elderly or the understanding of the patient is in doubt.
— Deal with any questions the patient has.
— Repeat information yourself and also ask patients to repeat information back to you to reinforce information.
— If necessary arrange a review within a short time of starting treatment to discuss progress or queries. Alternatively arrange follow up by another member of the primary healthcare team (e.g. asthma nurse to check inhaler technique 2–3 weeks after starting an inhaler).
— Address further patient questions and practical difficulties at follow up.
— Monitor repeat prescriptions.
Prescribing rates
There are wide variations in prescribing rates, e.g. variation in the rate of statin prescription cannot be accounted for by population characteristics; prescription rates for antibiotics for minor illness vary widely between GPs. Whether and how these reflect quality of care is controversial. Monitoring of prescribing using PACT data is described on page 10-08. Many Clinical Commissioning Groups (CCGs) have prescribing incentive schemes using this data to encourage more cost-effective prescribing.
Patient recall
Many studies suggest that more than half (and some estimate up to 90%) of information has been forgotten within a few minutes of leaving the surgery. One measure of quality is to gauge how much information has been retained by the patients. Characteristics of memorable information include that (Oxford Handbook of General Practice, 2014 (4 edn.) (4 ed.) Chantal Simon, Hazel Everitt, Francoise van Dorp, and Matt Burkes):
— the patient perceives it as important
— the patient understands it (avoid the use of jargon and medical terms, keep language brief and simple, support information with sketches/diagrams and patient information sheets)
— the information is given early in the consultation
— the information is given in small chunks (not too much at once).
Referral rates
There are wide variations in referral rates not accounted for by population characteristics (http://www.kingsfund.org.uk/sites/files/kf/Diagnosis%20and%20referral.pdf). Referral rates are not related to age or GP experience, use of investigations or postgraduate qualifications. Experience in a specialty increases referrals to that specialty, implying high referrers are not necessarily inadequate.
It is now common practice in primary care for referrals to be peer reviewed for appropriateness either by fellow colleagues in and outside the practice or in more independent Referral Management Centres. The criteria for ‘appropriateness’ differ widely. However, the value of this is debatable as the assessor is often not aware of the full circumstances of the referral. For example, it is appropriate to refer a child for a paediatric opinion purely to allay parental anxiety, but the referral might be deemed inappropriate on clinical grounds. Such Referral Management Schemes have had mixed success in lowering GP referral rates and are often mistrusted by GPs, who see them as questioning their automony (http://www.kingsfund.org.uk/sites/files/kf/Referral-management-lessons-for-success-Candace-Imison-Chris-Naylor-Kings-Fund-August2010.pdf.). However, simply looking at referral rates within the practice itself, which can be easy to identify by clear coding practices, can lead to constructive conversations on the learning needs of the practice and individual clinicians.
Doctors’ ability to detect illness
There are wide variations among GPs in their ability to detect certain illnesses, for exam-ple mental illness. GPs adept at identifying mental health have empathy, early eye contact, use directive rather than closed questioning, clarify the complaint at an early stage. Whether this is a marker of quality of care or just reflects the diversity of general practice is debat-able. It is also quite difficult to measure and assess, as sometimes medicine is complex and subjective. Having regular clinical meetings to discuss interesting cases and significant events analysis (SEAs) can be a non-judgemental way to bring up such issues.
Performance against pre-set targets
The introduction of the QOF in 2004 meant that all practices are assessed for quality in both clinical areas and management, against pre-set criteria or quality targets. This is covered in depth in section 3.
Comparisons of outcome, such as inadequate smear rates, diabetic outcome measures, or immu-nisation rates between practices can be a way to identify practices or GPs clearly performing less well than others. The reasons for the discrepancy must then be investigated. As part of the government drive towards transparency, much like the GP patient survey above, QOF achievement data is available to the public through the Information Centre for Health and Social Care (http://www.qof.ic.nhs.uk). This drive is connected to the aforementioned consumer making an informed choice of which practice to register with, the theory being that high performing practices will register more patients, hence will receive more income; this will then act as a lever for poorly performing practices to raise their standards. However, many argue that various aspects of general practice such as communication skills and empathy cannot be measured, and that using limited process measures like the QOF is not a true sign of quality.
Audit
Audit is a form of quality control. There are many different types of audit but they all involve:
examining, evaluating and reporting on findings within the organisation being audited
ensuring things are done the best way
examining the use of resources
time, effort and careful planning
comparing actual practice with quality standards.
Financial audit
When people first hear the word ‘audit’ they usually think of finance. Financial audit is about looking at accounts to see if they give a true and fair view of the organisation’s financial position at a given time. It is usually performed by external auditors, e.g. accountants.
Non-clinical audit
NHS organisations, from practice level to hospitals, are involved in tracing non-clinical activi-ties or systems along ‘audit paths’ to see whether things have happened the way that they should have. For example, an internal audit in a practice might be the tracing of a patient complaint from the initial letter of complaint through to resolution – was the practice complaints policy followed? Alternatively, an internal audit might involve ringing the practice at 8.30 every morning for a week and discovering how long it takes to get through. Reports from internal audit projects usually lead to recommendations for changes in the way procedures or systems within that organisation are run.
Organisational audit
This is an external, independent and voluntary audit of a whole organisation, based on a framework of explicit standards. An example of this is the RCGP Practice Accreditation and Quality Practice Award Schemes.
Clinical audit
Clinical audit was introduced to the NHS in 1993. It is defined as: ‘a quality improvement process that seeks to improve patient care and outcomes through systematic review of care against explicit criteria and the implementation of change’ (NICE, 2002) (National Institute for Clinical Excellence (2002) Principles for Best Practice in Clinical Audit. Oxford: Radcliffe Medical Press).
All practices in the UK are involved in audit in some way. It is a continual process and an integral part of clinical governance. Its purpose is to appraise current practice (What is happen-ing?) by measuring it against pre-selected standards (What should be happening?), to identify and implement areas for change (What changes are needed?) with the aims of:
improving care of patients
enhancing professionalism of staff
promoting efficient use of resources
assisting in continuing education
assisting administration
providing accountability to those outside the profession.
Types of audit
Criterion-based audit – A cycle which involves defining standards, collecting data to measure current practice against those standards and implementing any changes deemed necessary (see below).
Adverse occurrence screening and critical incident monitoring – this is often used to peer review cases that have caused concern or from which there was an unexpected outcome. The multidisciplinary team discusses individual anonymous cases to reflect upon the way the team functioned and to learn for the future. In the primary care setting, this is described as a ‘significant event analysis’.
Patient surveys and focus groups – these are methods used to obtain users’ views about the quality of care that they have received (see patient satisfaction, page 6-07).
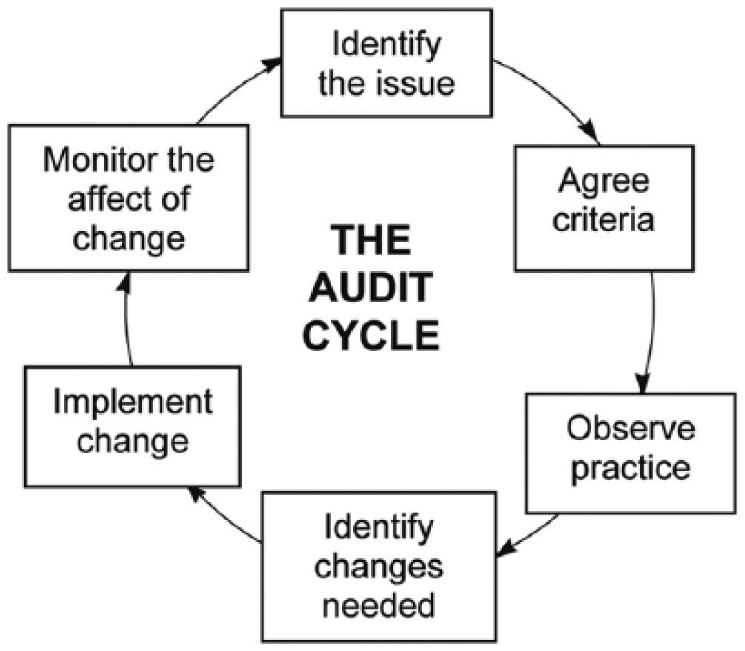
Criterion-based audit – the audit cycle
The audit cycle is the process of identifying areas of care to be audited, implementing any necessary changes, and then periodically reviewing the same issues (Figure 6.2).
The audit cycle
The stages of the audit cycle are as follows:
Choosing a topic: Any clinical practice matter is appropriate. Technically non-clinical matters fall under the umbrella of organisational audit, but the same principles can be used for clinical and non-clinical topics. Make sure the topic is important, manageable, clearly defined and data is available to assess the criteria chosen. Good starting points are significant events, QOF targets, complaints, National Service Framework or clinical guideline topics, or personal observations.
Choosing criteria: Criteria are specific statements of what should be happening. Criteria might be those laid down for quality payments, ‘gold standard’ care as defined in guidelines, or standards generated within the practice. Use evidence-based criteria wherever possible. All criteria have to be measurable – ideally with data already collected.
Setting standards: Standards are minimum levels of acceptable performance for a criterion. One hundred per cent achievement of standards is unusual, so set realistic standards based on quality framework levels, standards achieved by other practices (such as comparative practice data and audits from other practices), or previous audits within your own practice.
Observing practice: Information can be collected from computer registers, medical records, questionnaires of views of patients or staff, or data collection sheets (e.g. audits to check drugs in doctors’ bags are all in date).
Comparing results with standards: Consider why standards have not been met. What should be done? Who’s going to do it? When? How?
Repeating the audit cycle: This ensures that any action taken is effective.
Little Yarmouth practice is doing an audit. The flu vaccination targets were not met this year but more vaccines were given than were recorded in patient notes. That means that vaccinations were being given but not recorded, affecting payments received by the practice.
It was decided that an audit was the best way of determining who was getting vaccinated and who was being missed and where the unrecorded vaccines were going.
Dr Busby and the practice nurse were in charge of creating the standards. After some discussion, they decided to extract a list from the practice computer of all those in high-risk groups who should have been vaccinated. The criteria set were:
— Had all those at high risk, who had not specifically declined vaccination, been vaccinated? A target of 70% was set.
— Of those not vaccinated, what were the reasons for them not being vaccinated?
— How many people not in high-risk groups had been vaccinated and why?
The criteria for audit were agreed in the practice. Those in the high-risk group who had a note on their records that they had declined vaccination were then excluded from the ‘high-risk’ list. The remainder were split into a list of those who had received the vaccination and those who had not. Of those at high risk who had been vaccinated, 98% had been vaccinated by the practice nurses in flu clinics. Examination of the notes of those who had not been vaccinated showed that many had in fact received vaccination, but this was not recorded properly in their notes. These patients had all been vaccinated opportunistically in either GP surgeries, or in nurse appointments for other matters.
The problem was clearly one of recording. The notes of those patients without the correct Read codes that they had received a flu vaccination were amended and, after discussion with the whole practice, the policy was changed for the following year. It was decided that opportunistically giving flu vaccinations was good, but that it was easy to forget to record that a vaccination had been given, or to record it incorrectly so that it was not picked up
for QOF purposes. In future, a list would be kept in each consulting room. All the clinician would need to do would be to record the name of the patient and batch number of the vaccine and one individual would be responsible for entering all opportunistic vaccinations onto the computer. The following year the audit would be repeated to check the new procedure was working properly.
Significant Event Analysis
Significant Event Analysis is a recognised methodology for reflecting on important events in a practice. It is a form of peer review. Such events can be clinical or non-clinical.
Discussion of specific events can identify learning objectives and provoke emotions that can be harnessed to achieve change. For it to be effective, it must be practised in a culture that avoids blame and involves all disciplines, and should be expertly lead. There are seven steps, as outlined by the National Patient Safety Agency (http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=61501):
Staff should be confident in their ability to identify and prioritise a significant event when it happens.
The practice should be fully committed to the routine and regular analysis of significant events.
Collect and collate as much factual information on the event as possible from personal testimonies, written records and other healthcare documentation. For more complex events, an in-depth analysis will be required to fully understand causal factors.
The team should appoint a facilitator who will structure the meeting, maintain basic ground rules and help with the analysis of each event. The team should meet regularly to discuss, investigate and analyse events. These meetings are often the key function in co-ordinating the SEA process and they should be held in a fair, open, honest and non-threatening atmosphere.
Agree any ground rules before the meeting starts to reinforce the educational spirit of the SEA and ensure opinions are respected and individuals are not ‘blamed’.
Minutes of the meeting should be taken and action points noted. These should be sent to all staff, including those unable to attend the meeting.
An effective SEA should involve detailed discussion of each event, demonstration of insightful analysis, the identification of learning needs and agreement on any action to be taken.
The analysis of a significant event can be guided by answering four questions:
What happened?
Why did it happen?
What has been learned?
What has been changed or actioned?
The possible outcomes may include:
no action required;
a celebration of excellent care;
identification of a learning need;
a conventional analysis is required;
immediate action is required;
a further investigation is needed;
sharing the learning.
Any agreed action should be implemented by staff designated to co-ordinate and monitor change in the same way the practice would act on the results of ‘traditional’ analysis.
Progress with the implementation of necessary change should always be monitored by placing it on the agenda for future team or significant event meetings.
Where appropriate, the effective implementation and review of change is vital to the SEA process. To test how well the SEA process has gone, practices should ask themselves ‘What is the chance of this event happening again?’.
It is important to keep a comprehensive, anonymised, written record of every SEA, as external bodies will require evidence that the SEA was undertaken to a satisfactory standard. The SEA report is a written record of how effectively the significant event was analysed.
Reporting when things go wrong is essential in general practice. The practice should formally report (either to the National Reporting and Learning Service, or via the PCO/healthcare organisation) those events where patient safety has, or could have been, compromised.
Where a mechanism exists, practices should share knowledge of important significant events with local clinical governance leaders so that others may learn from these.
Clinical audit and research
‘Research is concerned with discovering the right thing to do; audit with ensuring that it is done right.’ Smith R. Audit & Research. BMJ 1992; 305: 905–6.
Research helps to answer the question, ‘What is best practice?’. It is concerned with creating new knowledge about which treatments work in given clinical situations, and forms the foun-dations of consensus about care that we should be providing. Clinical audit answers the ques-tion, ‘Are we following agreed best practice?’. However, research and audit are closely linked. Without research it is impossible to know what best practice is; without audit it is impossible to know whether we are following best practice. Differences between clinical audit and research are summarised in Table 6.1
Differences between clinical audit and research

Note: where new models of care are being audited, particularly if being compared against other models of care, the distinction between audit and research can become blurred. If in doubt, take advice from your local research ethics committee as research requires ethics approval. To perform research without ethics approval is a disciplinary matter.
Further information:
— National Institute for Clinical Excellence (2002) Principles for Best Practice in Clinical Audit. Oxford: Radcliffe Medical Press.
— Copeland G. A Practical Handbook for Clinical Audit. http://webarchive.nationalarchives.gov.uk/20060509091221/cgsupport.nhs.uk/resources/clinical_audit/1@introduction_and_contents.asp
Clinical guidelines, protocols and integrated care pathways
Clinical guidelines
Clinical guidelines are defined as ‘user-friendly statements that bring together the best external evidence and other knowledge necessary for decision making about a specific health problem’. Over recent years there has been a dramatic increase in the publication of guidelines.
These have been produced:
internationally – such as international guidelines on diabetes
nationally – through the National Institute of Health & Care Excellence (NICE), the Royal Colleges and many smaller specialist groups
locally – both at hospital level, such as local referral guidelines or shared care guidelines for chronic disease, and at practice level.
Good clinical guidelines have three properties. They:
define practice questions and identify all their decision options and outcomes
identify, appraise and summarise best evidence about prevention, diagnosis, prognosis, therapy, harm and cost-effectiveness
identify the decision points at which the evidence needs to be integrated with individual clinical experience and clinical circumstances in deciding a course of action.
Advantages of guidelines:
— they provide easily accessible guidance for busy clinicians and are a consistent basis for decision making
— they provide a practical framework for management of common problems and chronic disease
— they summarise the available research evidence
— they can be used as a basis for continuing medical education
— they may provide justification for expenditure as they can aid cost-effective use of limited resources
— they facilitate the audit cycle.
Disadvantages of guidelines:
— poor quality guidelines can reinforce poor practice
— lack of certainty of evidence – evidence is often not absolute; integrating best evidence into guidelines is frequently a matter of opinion about that evidence
— lack of relevance of the guidelines to the clinical setting – much of the ‘evidence’ used to develop guidelines comes from secondary care and may not reflect the situation in primary care
— the tendency towards uniformity can stifle innovation
— resistance to change – new research evidence or methods of care may not be considered until a new guideline is produced
— increased risk of litigation if an established guideline is not followed
— cost – time consuming to develop and update.
— lack of ownership – if developed by others may not feel, or be, relevant
— difficulties in implementation – guidelines that are not user-friendly and well disseminated will not be used.
As guidelines are time consuming to develop, it is usually better to use a guideline developed by a recognised guideline-producing body such as NICE or SIGN, rather than trying to develop your own in-house guidelines. Before starting to use a guideline, always ask ‘Is this guideline valid, important and applicable in my practice?’. If the answer is yes, then look at the barriers that prevent implementation and how they can be overcome. For example, are there areas of service provision that must be changed, or is there an educational deficit that needs to be addressed? Ensure that there is collaboration and engagement with all the key colleagues/stake-holders needed to implement the guideline.
Protocols
Protocol is the term reserved for guidelines at the more rigid end of the spectrum. These are very specific guidelines that are expected to be followed in detail, with little scope for vari-ation, for example resuscitation protocols.
Integrated care pathways
Integrated care pathways (ICPs) amalgamate all the anticipated elements of care and treat-ment of the multidisciplinary team, for a particular patient group in order to achieve agreed outcomes. Any deviation from the plan is documented as variance – the analysis of which provides information for the review of current practice.
ICPs aim to:
facilitate introduction of guidelines and systemic audit into clinical practice
improve multidisciplinary communication and care planning
reach or exceed existing standards
decrease unwanted practice variation
improve clinician–patient communication and patient satisfaction (in addition to clinician–clinician communication)
identify research and development questions
cross the interface between primary, secondary and social care.
Grading and classification of evidence for the purpose of constructing guidelines, protocols and ICPs
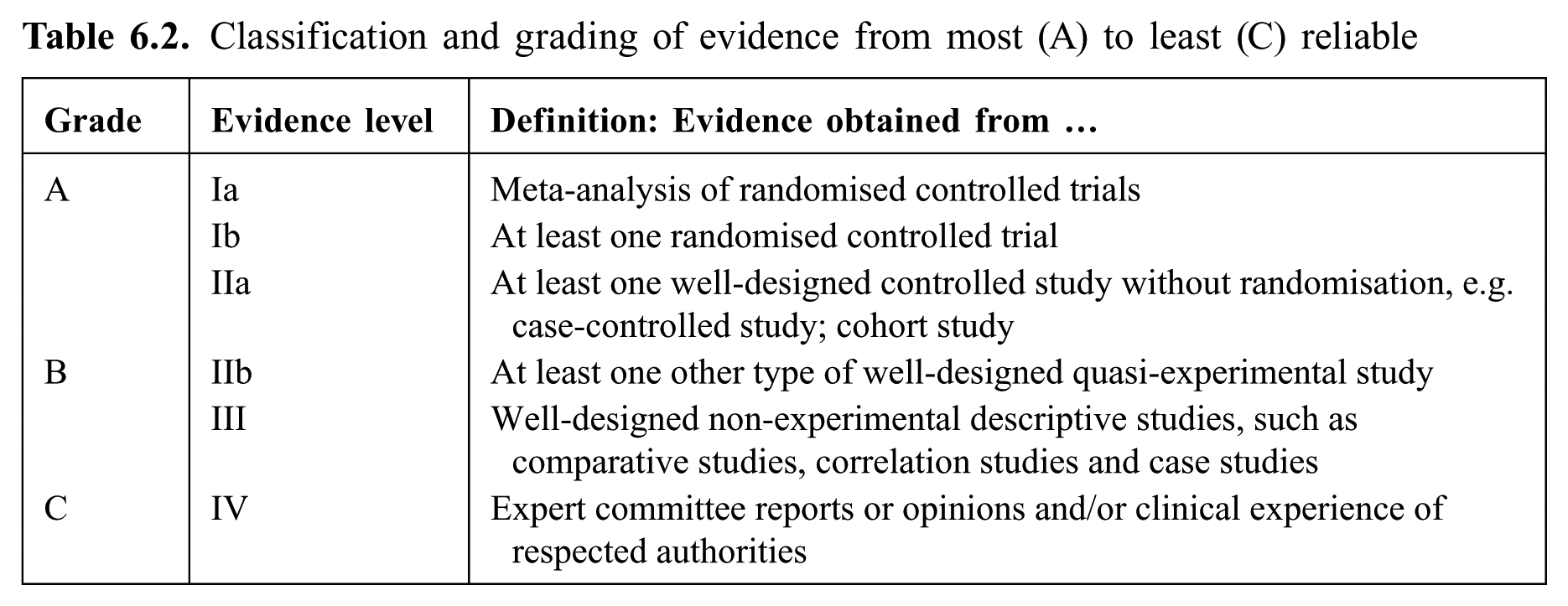
Constructing guidelines, protocols and ICPs involves integrating clinical expertise with the best available external clinical evidence from systematic research. Critical appraisal is the process of assessing and interpreting evidence by systematically considering its validity, results and relevance. It is essential to avoid misinterpretation and misuse of evidence in practice. For most points made in clinical guidelines, a level of evidence is quoted, intended to give the reader some idea of how reliable the point is. The most commonly used grading system is summarised in Table 6.2.
Classification and grading of evidence from most (A) to least (C) reliable
Further information:
— National Electronic Library for Health: guidelines database, integrated care pathways database and useful information on development of guidelines. www.evidence.nhs.uk
— NICE: http://www.nice.org.uk/
— Scottish Intercollegiate Guidelines Network: www.sign.ac.uk
— eGuidelines: www.eguidelines.co.uk (free registration required)
Central Alerting System
Patient safety alerts are a crucial part of NHS England’s work to rapidly alert the healthcare system to risks and provide guidance on preventing potential incidents that may lead to harm or death. These incidents are identified using the National Patient Safety Agency reporting system to spot emerging patterns at a national level, so that appropriate guidance can be developed and issued to protect patients from harm.
Patient safety alerts are issued via the Central Alerting System (CAS), a web-based cascading system for issuing alerts, important public health messages and other safety critical information and guidance to the NHS and other organisations, including independent providers of health and social care.
The lead partner and practice manager will be emailed with such alerts relevant to primary care. An example of such an alert would be faulty insulin pens, which would require practices to search for patients on such pens and contact them to ensure appropriate action is required. In CQC inspections evidence is often sought on how practices deal with central alerts and what record is kept of action taken. For further information see:
Risk management
Definition and importance
Risk can be defined as the threat or probability that an action or event will adversely or beneficially affect an organisation’s ability to achieve its objectives. In general usage, the convention is to focus only on potential negative impact.
Risk management may simply be defined as ‘doing it wrong, less often’ and therefore involves recognising and reducing the opportunity for risks to occur. In general practice, traditionally the term ‘risk management’ has been used to describe risk to the patient. Clinical risk manage-ment, or patient safety, aims to ensure a safe and high quality service to patients by working closely with other practice staff and GPs to identify and assess clinical risks inherent in day-to-day practice, and then taking action to eliminate or minimise their impact.
However, there are also other risks that should be considered, for example risks to employees and other staff working in the practice, and financial risks inherent in running a small busi-ness. Risk is part of life, particularly for GPs, since their job entails bearing risk: the chance that any one of the patients they see with common and probably mild and self-limiting illness could have a life-threatening disease. That does not reduce the importance of taking steps to ensure that neither doctor nor patient slips on the wet floor when walking to the consulting room.
We are all good at spotting a risk outside our own environment – the loose slates on the neighbour’s roof, faulty electrical sockets, the unguarded hole in the pavement – and saying that ‘they’ should do something about it. We tend not to see the risks in our own home and workplace, and if they are pointed out may take a casual attitude to dealing with them. Other risks are more difficult to recognise: contaminated surfaces; a mistake during a rushed staff handover; medication allergies; or common practice to make something quicker or easier that raises the risk of something going wrong.
A team training session was devoted to risk management. The team was divided into groups of three, each with a doctor or nurse, a receptionist and a member of the admin team, and they were asked to go around the building looking at it as if they were a patient or visitor. At the end they shared their impressions. They realised how much they just didn’t see –
not just scuffed paintwork in the waiting room, but also loose flexes in consulting rooms and computer screens visible to the public – and made a plan to repeat the exercise regularly.
Visitors notice things. Locums are a valuable source of comment as they see many practices and different ways of doing things, and other practice managers can provide very useful feedback. Outside contractors working in the premises may have comments on risks in their area of expertise.
Contrary attitudes about ‘the nanny state’ and over-regulation contribute to a ‘laissez-faire’ approach to risk management. Since the problems with children’s cardiac surgery services in Bristol in the 1990s, secondary care has become much more conscious of the penalties of not managing risk, and the NHS has learned from the practice of the airline industry. Risks in primary care may rarely carry quite such high penalties, but general practices that manage risks properly reduce the number of complaints and liability claims, improve patient care, and as a result are likely to be more financially stable and to have a confident team.
There are avoidable risks and unavoidable ones. Risk management is about avoiding the former and reducing the impact of the latter.
Risk management is a systematic, proactive approach consisting of four main principles:
Identify the risk.
Analyse the risk.
Control the risk.
Cost the risk.
The benefits of good risk management for the practice include:
improved patient care
increased patient satisfaction and therefore reduced likelihood of complaint
reduced likelihood of adverse outcomes
reduced stress from being sued or disciplined
professional and practice/business personal and satisfaction.
For example: although the risk of fire is moderate, the penalty if a fire occurs can be very high. The box below illustrates a systematic approach to managing the risk.
Fire risk management
Ensure that the practice has adequate fire insurance
Reduce the risk of a fire starting
Ensure that there are functioning fire and smoke alarms
Ensure that staff know how to respond if an alarm goes off and what to do thereafter
Check that exit and escape routes are signed, are adequate and are not obstructed
Install and check fire extinguishers and train staff on their use
Practise safe evacuation of people from the building
Have a programme for recovery from the disaster of loss of building, equipment and records
Take steps to ensure that alarm testing is not mistaken for the real thing, and vice versa
Risk management in practice
Research into risk management has demonstrated that adverse events predominantly occur as a result of human error. Additionally, it has been noted that errors occur due to the failure of defence mechanisms designed to prevent adverse events.
Risks which are brought to someone’s attention are usually managed, but since we tend not to notice areas of risk, a proactive as well as a reactive approach is essential. A systematic programme should be combined with vigilance, i.e. actively seeking out potential problems, combined with effective review and modification of procedures when something goes wrong.
The practice manager usually takes the responsibility of being the practice’s risk manager. This involves identifying risks, assessing their importance (frequency and severity), organising the necessary steps to reduce or eliminate the risk, and checking that those steps have been taken. Attitude is all-important.
The National Patient Safety Agency describe seven steps to patient safety (Figure 6.3). http://www.nrls.npsa.nhs.uk/resources/collections/seven-steps-to-patient-safety/

The seven steps to patient safety
Systematic approach to identification of risk
The medical indemnity organisations all offer risk management advice (see ‘Further informa-tion’ below). Their experience covers non-clinical as well as clinical areas and can provide a systematic structure for managing risk.
Managing risk is a continuous process of evaluation, action and re-evaluation, rather than a static process (Figure 6.4). Undertaking a risk assessment is an important step in identifying areas where practices are performing well and areas where changes might be beneficial.
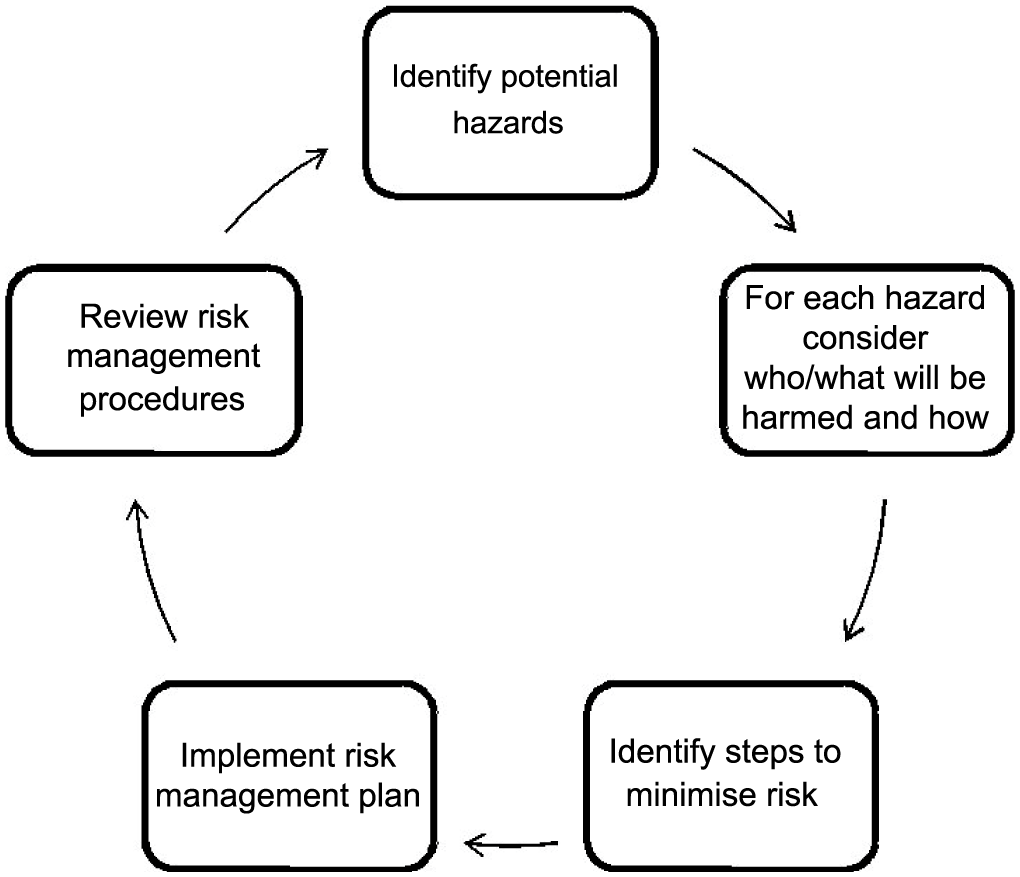
The risk assessment cycle
Risk assessment involves understanding and knowing what to do if the risk occurs by identify-ing in advance potential hazards and risks. For each potential hazard, it is important to consider who or what might be harmed and how, and evaluate the risks to decide whether the existing precautions are adequate or whether further action is needed. Regular reviews of the assess-ment should be performed, revising it if necessary.
Once a practice has undertaken a risk assessment report they are encouraged to use the report to compile a risk register (action plan) in order to address these identified risks.
Risk register
A risk register is part of the process of recording how risk is managed in an organisation. Each risk identified should be recorded in a register that summarises:
description of the risk, its cause and impact
existing controls for the risk
assessment of the consequences and likelihood of the risk happening with the existing controls
risk rating: low, medium, high or very high
overall priority of the risk.
Once the risk register is completed it is a tool by which practices can manage or treat risk by recording the priority and options in an action plan. Keeping a record of risks will aid in reviews and check whether risks have changed or new risk needs to be added.
Vigilance
Staff attitudes are crucial to successful risk management. Staff should feel both motivated and accountable, and they should know what to do. Organisations that manage risk well have a higher rate of reporting of errors, and staff members feel able to introduce ideas.
Risk management should be part of induction and ongoing training, and there should be plenty of opportunities for staff to put forward and analyse proposals. If there is a staff member who appears to take avoidable risks, this can be raised at appraisal.
A new receptionist heard the fire alarm and assumed it was another test. She had not been given any training so she carried on with answering the phone. Unfortunately it was not a test: a kettle had burned out in the kitchen. By the time the fire brigade had been called, the fire had caused a lot of damage.
Learning when things go wrong
The important thing is to learn from the experience. Certainly, what most people who have been on the end of a bad experience want is not vengeance or money, but to feel that others will not suffer the same way in the future. All significant or major complaints and other problems or mistakes should be put through significant event analysis (see page 6-17).
Dr Smithfield reported to the practice manager that he had averted a nasty incident by catching an elderly patient who had fallen off the small stool provided to climb onto the examination couch in his consulting room.
A review of all the consulting rooms revealed that there were various stools and boxes being used to aid patients to climb onto examination couches, none of which were designed for the purpose. The practice manager raised the issue at the next practice meeting.
Dr Inago suggested that the practice should replace the old static couches and invest in new examination couches that could be raised and lowered as required. Although everyone agreed that this would be the ideal, at £5000 per couch, and with eight couches to replace, this was not seen as a realistic short-term proposition. Instead, the practice replaced the collection of stools and boxes that were in use with steps that elderly or disabled patients could manage with much less risk of a fall.
Patient feedback
Patients are an underused source of feedback and comment – see page 8-52. For advice on complaints see page 8-68.
Areas of risk
The list is not exhaustive, but highlights areas which commonly cause problems:
clinical care (including: test results, referrals)
prescribing
confidentiality(including: medical records)
health and safety
staff (including: complaints, incident reporting, practice guidelines)
communication
organisational
financial.
Clinical care
Clinicians’ clinical competence: Are all clinicians keeping up to date? Is their health or any other factor affecting their performance? For advice on poorly performing doctors see page 2-09.
Test results: Does the practice have a clear policy on how patients obtain test results, especially where the result is clinically important, and do all clinicians, including new, part-time and temporary doctors and all nurses, follow it?
Are promised referrals being made? Proformas to record referrals made during consultations provide one possible solution.
Clinical governance – see page 6-02.
Prescribing
There is an error in up to 5% of all prescriptions and medication problems which causes 10% of admissions – see section 10.
Common reasons for problems with repeat prescribing include:
no repeat-prescribing protocol
no designated receptionist to record or generate repeat prescriptions – these are generated in the reception on an ad hoc basis, i.e. when time permits throughout the day
untrained staff are adding medication to the computer acute and repeat prescribing systems
medication reviews are undertaken on an ad hoc basis; no review dates are set on the computer
no system for recalling patients on long-term medication, e.g. lithium, thyroxine or anti-convulsants
medication suggested by secondary care practitioners is instigated without written confirmation
Confidentiality
This is a growing area of risk. These are some of the questions to ask.
Are electronic and paper notes adequately safeguarded? For example, is all hard-copy patient identifiable information that is disposed of being shredded? Are patient notes securely stored?
Can patients see screens with confidential information about other people?
Are computers being left unattended?
Do staff and doctors respect patients’ confidentiality in their conversations inside and outside the practice? Breaches of confidentiality in waiting rooms and reception areas are easy to make. It is important that staff contracts include a clause covering confidentiality post-employment.
Do all staff take appropriate steps when asked by outside organisations for information about patients?
Is the confidentiality of children and other vulnerable groups respected? See section 8 and 12-15.
Are the Caldicott principles being followed?
Justify the purpose: Patients may voluntarily agree to identifiable information about themselves being released to specific individuals for known purposes. Implied consent occurs when a patient who is aware that their personal information may be shared and of their right to refuse, but makes no objection. Patients must have had a realistic opportunity to refuse. If patients refuse, it should be clearly documented and respected.
Do not use patient identifiable information unless it is absolutely necessary: It is not necessary to seek consent to use anonymous information. If in doubt seek advice from the BMA or your defence organisation. Health information used for secondary purposes, e.g. planning, teaching, audit, should – wherever possible – be anonymous.
Use the minimum necessary patient identifiable information.
Access to patient identifiable information should be on a strict ‘need to know basis’.
Everyone should be aware of their responsibilities.
Understand and comply with the law.
Health and safety
The aim of health and safety risk management is to minimise incidents and injuries to staff, patients and the public.
Employer’s liability and health and safety is covered in page 4-07
Control of substances hazardous to health, see page 4-09
Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR), see page 4-11
Fire, see page 11-25
Infection control, see below.
A temporary doctor sustained a needlestick injury. She correctly discussed this with the patient’s regular GP, but no-one knew how needlestick injuries should be handled. The temporary doctor later presented the incident at a significant event analysis meeting and the instructions were put up in appropriate places on the wall and on the practice intranet.
Staff
Are staff able to do their jobs? This involves consideration of their skills and health as well as the provision of adequate time and resources. See page 2-60 (appraisal) and section 5 (education).
Are staff committed to risk management?
Are staff workplaces user-friendly? See section 4.
Are staff protected from violence? See page 8-32.
Are staff protected from other hazards, e.g. hepatitis B? See page 4-08.
Is there an adequate orientation process for new and temporary staff (see page 4-07), including: — familiarity with practice policies and protocols — emergency procedures — privacy — security — roles and responsibilities — knowledge management.
At the end of a very stressful day – high patient demand, clinicians and receptionists off sick, computer problems, a patient collapsing in the waiting room – the member of staff responsible for ensuring that the computer was backed up was so overloaded with ‘must dos’ from all sides that she didn’t ensure the computer back up. To her knowledge it had never failed before. Unfortunately the day’s computer problems were a symptom of a serious fault. Next morning the computer crashed and the day’s records were lost. After a significant event analysis the practice decided that an overhaul of the computer system was needed, and that staff needed to be confident that if they were struggling they could say so and would be listened to.
Communication and message-taking
Poor communication or misplacement of messages are common causes of problems.
Is there a standard messaging system that is reliable and accountable? Are verbal, phone, written and electronic messages properly taken, recorded and passed on?
Do patients know what to expect when they leave a message? See page 12-03.
Are there regular practice meetings?
Are there regular meetings of the whole primary care team?
If information received from elsewhere is illegible or in any other way uninterpretable, is there a procedure in place to obtain replacement information?
Organisational
Does the practice culture support risk reduction in the way it recruits, inducts, trains and appraises staff? See Sections 2, 4 and 5.
Do staff work as a team? See page 7-17.
Does the induction of new staff cover risk management? See page 4-07.
Does the practice have an up-to-date disaster recovery plan? See Appendix page 35.
Are guidelines, policies and other sources of information easily available, even to new and temporary staff, e.g. through a practice intranet?
Are home visit consultations always recorded on the computer?
Is handwriting legible on written records?
Is there a process to ensure that electronic data are inputted to the correct records (e.g. scanned letters and results)?
Is telephone advice always recorded?
Is there a process for tracking medical records?
Financial risk
Financial risk is becoming an increasing concern in general practice. Threats from new pro-viders to list size and service provision in existing practices means that income cannot be guaranteed on an ongoing basis. This has led to difficult decisions for practices about invest-ment in new services, initiatives and staff.
The Tudor Practice has recently lost a salaried GP who moved to another practice. The partners have decided that an additional partner would be a better investment as the existing partners feel overburdened with administrative and management tasks that they could not ask a salaried GP to share. However, a new health centre has just opened in the vicinity. They are not yet sure what impact that is likely to have on their income (e.g. effect on list size). After considerable discussion, they decide that they cannot take the financial risk of appointing a new partner, and re-advertise for a salaried sessional doctor.
Further information:
— The National Patient Safety Agency (Special Health Authority created to coordinate the efforts of all those involved in healthcare, and more importantly, to learn from adverse incidents occurring in the NHS) aims to improve the safety and quality of care through reporting, analysing and learning from patient safety incidents and ‘near misses’ involving NHS patients. www.npsa.nhs.uk
— Medical Protection Society. http://www.medicalprotection.org/uk/
— Medical Defence Union. http://www.themdu.com
— The Medical and Dental Defence Union of Scotland. www.mddus.com — Haynes K and Thomas M. Clinical Risk Management in Primary Care. Oxford: Radcliffe, 2005 (a comprehensive look at all aspects of the subject).
Example of a standard operating procedure (SOP) for cold chain (items requiring refrigeration)
The below is an example of a Cold Chain Policy. When developing one for your own practice take into account any local procedures that may differ.
Insert practice address
This SOP should be used in conjunction with the SOP for non-controlled drugs, controlled drugs (CDs), prescription (controlled stationery) SOP.
The following additional principles apply to the items requiring refrigeration. For practices this will mainly be vaccines, so the rest of the document will refer to vaccines, but is similarly valid for other medicines requiring refrigeration.
It is essential that all those handling vaccines follow policies to ensure cold chain compliance.
Guidance is given in chapter 3 [storage, distribution and disposal of vaccines] of Immunisation against infectious disease (Green Book) 2006 edition. https://www.gov.uk/government/collections/immunisation-against-infectious-disease-the-green-book
Vaccines are temperature sensitive. If they are exposed to temperatures outside the recommended range of 2–8°C their potency can be reduced, meaning patients won’t get the correct level of protection from disease.
Cold chain is the term used for keeping vaccines at the right temperature from the moment they are manufactured up to the moment they are given to a patient. If their temperature goes above or below the recommended range the cold chain has been broken.
Each practice should have one trained individual, with at least one trained deputy, responsible for the receipt and storage of refrigerated items and the recording of refrigerator temperatures. These individuals should be familiar with the above guidance and the following practice points based on it.
Insert name…., insert position held…is responsible and Insert name…., insert position held…is the deputy.
Vaccines must be refrigerated immediately on receipt and must not be left at room temperature.
Vaccine types, brands, quantities, batch numbers and expiry dates should be recorded with date and time of receipt.
Specialised vaccine/pharmacy refrigerators should only be used for medicines. No food, drink or clinical specimens must be kept in this fridge.
Refrigerators must ideally be lockable or at least within a room that is locked when unoc-cupied by a member of staff.
Opening of the refrigerator door should be kept to a minimum.
Over-ordering or stockpiling should be avoided. Ideally the refrigerator should be filled to 50% of capacity to encourage air to circulate freely. The fridge should not be filled beyond 75% of capacity (see ‘the dangers of an over-packed fridge’ below).
Vaccine stocks should be placed within the refrigerator so that those with shorter expiry dates are used first.
Any out-of-date stock should be clearly marked and removed from the refrigerator for disposal by local procedures.
The accidental interruption of the electricity supply can be prevented by using a switchless socket (preferable to cautionary notices).
Three refrigerator thermometer readings (current, minimum and maximum temperatures) should be monitored and recorded at least once each working day and documented on a chart (example on p. 24 of Green Book 2006/HPA website, see below).
Thermometers should be reset and replaced according to the manufacturer’s guidance.
Thermometers should be recalibrated annually.
Records should be retained for a minimum of one year from date of last entry.
Regular audit of practice (at least annually) should be undertaken.
It is recommended that the following poster be affixed to the outside door of the medicine fridge.
Insert practice address
STORE VACCINES IN RANGE 2–8°C
REPORT DEVIATIONS FROM THIS RANGE
For advice contact a member of the CCG Pharmacy Team on (Tel) XXXX-XXX-XXXX or (Email)
MONITOR AND RECORD: CURRENT, MAXIMUM AND MINIMUM TEMPERATURES
EACH WORKING DAY
RESET THE THERMOMETER EACH TIME AFTER TAKING TEMPERATURE READINGS
NAMES OF TRAINED INDIVIDUAL RESPONSIBLE FOR MONITORING AND TRAINED
DEPUT(Y/IES):
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . insert names
The dangers of an over-packed fridge:
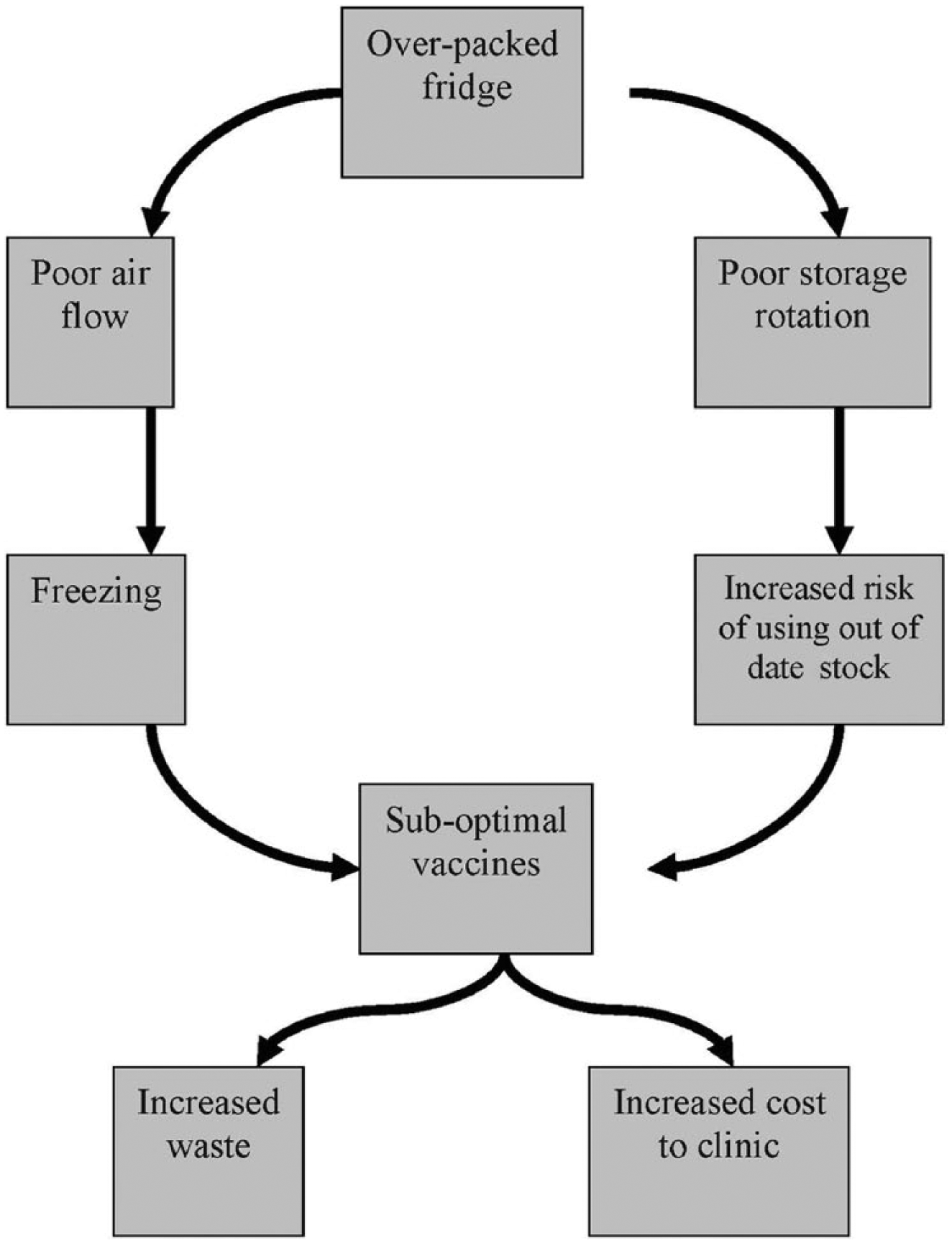
Footnotes
Appendix 1 – Example refrigerator temperature record sheet
Insert practice address MONTH ………………………
Insert Store ID / location – e.g. nurses room 1
Temperature should be within the range of 2–8°C. If the temperatures are outside the recommended range take appropriate action as indicated in the written procedure.
Appendix 2 – Example sign off sheet
Insert practice address
With thanks to the pharmacy team at XXX CCG.
Written by: Insert name and position
Date written: e.g. x.x.2008 Review date: e.g. x.x.2013