
Abstract
During the H1N1 pandemic, governments tailored their communications plans in order to influence risk perception and promote public compliance with the public health plan measures. Considering the volume and the content of calls to flu information centres as indicators of the public risk perception, this mixed method study compares the relation between public communications, risk perception and immunization behaviour in Quebec and France. Results suggest that advocating for clear information and coordination between health authorities and the media promotes adherence to preventive behaviour. However, over-exaggerating the risks and minimizing the population’s agency may undermine health authority credibility.
1. Introduction
The 2009 swine flu outbreak, also known as the H1N1 pandemic, has massively mobilized political and health institutions. North American and European countries have implemented mass immunization programmes, with very different levels of success (Rubin et al., 2009). As in similar late modern epidemics, such as SARS (severe acute respiratory syndrome) or avian flu, information and communications processes have been central in the crisis management (Wallis and Nerlich, 2005). From the obstacles and successes encountered, the H1N1 crisis has revealed that these communications processes were complex not only because of the multiplicity of voices involved (governments, health institutions, traditional and new media) but also because of the relation between the content of the information, the relative credibility of its sources and the emotional and behavioural responses of the population (Atlani-Duault and Kendall, 2009; Goodwin et al., 2009; Jones and Salathé, 2009).
The influence of communications on risk perception and on health behaviours has been established by health crisis research during the last decade (Smith, 2006). This relation could be one of the determinants for the wide local and international differences in both risk perception and the adoption of preventive behaviours (De Zwart et al., 2009). Thus, understanding the relation between communications about a health risk, the lay public’s perceptions and understanding and the subsequent adoption of preventive measures is a cornerstone of health crisis intervention planning.
The aim of this paper is to compare the relation between communications about H1N1 in the public space, risk perceptions and immunization behaviour in two sites with strikingly different immunization rates: Quebec 57% and France 7%, in spite of a relatively similar cultural heritage.
The influence of the media on risk perception
Fear and the mobilization of social solidarities have always been powerful tools of social control and they appear to be at the forefront of the struggle against emerging diseases (Farmer, 2001; Tapiero and Carle, 2009; Ungar, 2001; Washer, 2011). Using a structural functionalist framework to analyse risk perception, Mary Douglas proposes that what is perceived as a risk is largely determined by the person’s cultural and social positioning, and in particular by specific social solidarity dynamics (Douglas and Wildavsky, 1983). According to Douglas, when social solidarity is shattered, people express their feelings of threat by evoking shared beliefs about impending disasters. Wilkinson (2001) argues that risk perception is simultaneously influenced by shifts in power and authority which may undermine social solidarities, by the emergence of a risk consciousness in industrial societies (Beck, 1999) and by a complex configuration of factors which contributes and shapes individual perceptions and agency (Tansey, 2004).
During the last decade, epidemics and emerging infectious disease researchers have shown that the media not only have been the main source of information for the public but are also considered as being the most trustworthy (Brug et al., 2004; Gaglia et al., 2008; Paek et al., 2008). Even if during these crises the media generally provided a good share of space for the national public health plans (Janssen et al., 2006), the direct role of the health services in disseminating information was minimal (Marinos et al., 2007). In recent years, news coverage of new infectious diseases and epidemics has been extensive (Young, Norman and Humphreys, 2008). SARS and the H1N1 pandemics reached peak levels of news coverage not only in traditional media like radio, television and the written press (Duncan, 2009) but also on the web (Pandey et al., 2010). The content and the quantity of information given by the media on a particular crisis influence the public’s risk perception (Leppin and Aro, 2009). Transnational similarities appear to be related to globalization communications strategies, while national variations may reflect local dynamics. In a survey of college students in the United States, Jones and Salathé (2009) documented a strong association between H1N1 related fears and those related to avian flu and to terrorism. Their observations confirm that the public may consider that the events most covered by the media are likely to have a greater degree of seriousness (Young et al., 2008), highlighting the increasing gap between the perceived threats and the problems in fact associated with an increased mortality or morbidity (Glass, 2004).
During the swine flu outbreak, the similarities between H1N1 and Spanish flu were emphasized to mobilize political leaders and to convince citizens to support the allocation of funding for pandemic preparedness (Giles-Vernick, Craddock and Gunn, 2010; Mathews et al., 2009; Stern, Cetron and Markel, 2009; Zylberman, 2010). The use of crude historical images and the evocation of massive morbidity and civil chaos were at the forefront (Barry, 2005; Crosby, 2003). Although the communications strategies were strongly related to the type of media and to their ideological and political orientations, a certain number of common features characterize the media information on H1N1. First, the media coverage always reflected, to a certain extent, the different discourses on the pandemic. It was the local balance between the official health authorities’ discourses and the voices opposing it, which varied widely from country to country. Second, the transmission of information was very rapid, in real time, with a continuous flux of information constituted of fragments of news (Aubert, 2003). This time dimension focuses the attention of the recipients on immediate events, without providing the tools to analyse the information (Bourdieu et al., 2002). Furthermore, the ongoing repetition of threatening information is likely to increase fear and confusion mimicking, in some way, traumatic symptomatology associated with the repetitive intrusion of vivid and frightening images (Duggal, Berezkin and John, 2002). If risk perception is strongly modulated by cultural and social influences, it is also associated with individual characteristics such as gender, the neuroticism index and psychological resiliency (Ibuka et al., 2010; Smith, 2006).
In spite of the importance of better understanding this considerable determinant of behaviour, local and national differences in risk perception have not been thoroughly studied. The relative credibility of the different discourses accessed through the media appears to be a major factor explaining some of these disparities (Elledge et al., 2008; Wagner-Egger et al., 2011).
Risk perceptions and the adoption of preventive behaviours
Overall, the increase in risk perception is associated with the adoption of preventive behaviours that are the core component of public health action plans (Hooker, 2010; Rubin et al., 2009). However, to feed public panic can also be very costly and have numerous negative consequences. First, panic is associated with avoidance behaviours, such as absenteeism, that have high social and economic costs (Bonneux and Van Damme, 2006; Young and Breslau, 2007). These avoidance behaviours may, in some cases, be related to increased mortality and morbidity as has been the case when Americans used road transportation rather than air travel after 9/11 (Gray and Ropeik, 2002). Second, the fear of being stigmatized may lead in certain cultures, to a denial or minimization of risks as has been well documented in rural Asian regions during the Asian flu (Kleinman et al., 2008). Third, research has shown that the security discourse can mobilize public opinion very efficiently through emotional upheaval, but that this can also be associated with an upsurge in psychological distress and sometimes even with the emergence of panic and post-traumatic disorders (Duggal et al., 2002; Rousseau and Machouf, 2005; Young and Breslau, 2007). Indirect exposure to stressful information through the media can have adverse effects for vulnerable populations, triggering or aggravating anxiety symptoms (Fremont, 2004). Finally, the repeated use of fear and the emergence of a risk society may undermine public trust in institutions which may be perceived as dramatizing minor risks or as being relatively helpless to respond to them (Larson et al., 2011; Poland, 2010; Ungar, 2001; Washer, 2011). Analysing Australia’s pandemic control strategies, Davis et al. (2011) described how the communications plan focussed on promoting public compliance with the public health plan measures without paying much attention to community perceptions and voices. The authors argue that the pandemic control planning relies on a restricted view of human agency. They propose that effective pandemic control requires a systematic dialogue with communities to avoid complacency or panic and to enhance public participation in prevention.
Using a mixed method approach, this paper proposes to consider the volume of calls to flu information and counselling call centres and the experience of the call centre counsellors and administrators during the H1N1 outbreak as indicators of the public risk perception in Quebec and in France during the autumn 2009 H1N1 pandemic outbreak.
It addresses the following questions:
What is the association between the intensity of newspaper coverage, the proportion of H1N1-positive tests and the call volume to H1N1 information lines in Quebec and in France?
What are the perceptions of the H1N1 information lines’ counsellors and administrators of the relations between public risk perception and media coverage? What factors influence the credibility of voices and messages? According to counsellors and administrators, what are possible differences between Quebec and France?
What are the subsequent immunization behaviours (2010–2011) for seasonal flu in at-risk groups and to what extent could they be related to the communications strategies during the H1N1 outbreak?
2. Method
Setting
France and Quebec are two francophone regions that share common historical and cultural roots, although their present social, political and health organizations are distinct. In Quebec, Info-Santé is a call centre set up by the Ministry of Health and Social Services (MHSS) to provide permanent access to medical information/consultation in a variety of non-emergency situations. Since the volume of calls concerning H1N1 flu increased dramatically, the MHSS implemented a phone line specifically dedicated to H1N1 on October 19, 2009. Throughout the pandemic, Info-Santé played a crucial role in the public health measures in Quebec by providing an accurate source of information in coordination with the MHSS.
In France, the Info-Grippe phone line was set up in 2005 by the Ministry of Health to implement prevention measures and to prepare for a possible flu pandemic. When the first cases of H1N1 were reported in the media, a private agency, specializing in medical phone lines, was responsible for organizing the call centres. As the volume of calls from the general population increased during the H1N1 pandemic, the number of counsellors was increased and the hours of operation were extended. As in the case of Info-Santé, the Ministry of Health provided the information to be delivered to the public and updated it regularly.
Quantitative data
Media coverage
For both sites, the weekly media coverage of H1N1 was estimated by the number of articles containing the terms “H1N1” or “swine flu” in the top five newspapers for each country. In France, the newspapers with the highest circulation were Ouest-France, Le Parisien, L’Equipe, Le Monde and La Voix du Nord. Although L’Equipe specializes in sports coverage, the number of articles concerning the flu was not significantly different than that of the sixth most circulated newspaper. In Quebec, the newspapers considered were The Gazette, Le Soleil, Le Devoir, La Presse and Le Nouvelliste. Le Journal de Montreal and Journal de Québec have higher circulations but were not accessible in the database. Circulation numbers were provided by the Editor and Publisher International Yearbook (2010: III-12–III-13, I-415–I-418).
Proportion of H1N1-positive tests
In both countries, the treating physicians sent cultures to their respective health agencies which were tested to identify the specific influenza strains. The weekly proportions of H1N1-positive tests were released by the MHSS in Quebec and in the reports of the Institut de veille sanitaire (INVS) in France. The INVS is a public health agency specializing in surveillance. Although these numbers are dependent on the amount of testing by the physicians, they are used to describe the weekly variation of H1N1 in both sites.
Volume of calls to medical information phone lines
The public request for health information/consultation about H1N1 was estimated by the volume of calls to the medical information phone lines (Info-Santé and Info-Grippe). This data is calculated per million population for comparison purposes.
The seasonal flu immunization data (and statistical inference) before and after the H1N1 outbreak was obtained from Statistics Canada in the annual Canadian Community Health Survey from the CANSIM database for Quebec and from the national survey on vaccine coverage for INVS in France (Guthmann et al., 2010).
Qualitative data
To document the perceptions of the call centre personnel (administrators and counsellors) of the relation between public discourses, coverage by the media and public risk perceptions, we investigated the experiences of the Info-Santé (Quebec) and Info-Grippe (France) personnel by means of focus groups and individual interviews.
In Quebec, two focus groups were held in the offices of Info-Santé, the first with administrators (n = 7) on March 30, 2011 and the second with nursing counsellors (n = 9) on March 31, 2011. The following themes were discussed: the turning points in the pandemic and their determinants (media events which were associated with more reactions), the public understanding of the pandemic and their emotional and behavioural responses to it, as revealed in the call content, and the experience of counsellors.
In France, because Info-Grippe employed many temporary counsellors during the H1N1 pandemic, it was impossible to organize a focus group with the discharged staff. The personnel that remained in the organization after the crisis were interviewed individually because their schedules and office locations made the organization of a focus group impossible. The counsellors (n = 5) and the administrators from the government (n = 4) and from the agency (n = 4) were interviewed with the same guide as used in the focus groups in Quebec.
Subsequently, the focus group responses and interviews were transcribed and submitted for thematic analysis (Quivy and Campenhoudt, 1995). Because of the potential importance of researchers’ subjectivity in the coding and analysis process (Paillé and Mucchielli, 2012), a team of three persons was involved in the coding and the analysis of the qualitative data. The members of the team first read all the material repeatedly. Then, passages (“unit of meaning”) were labelled with keywords to help identify not only recurring themes in line with the research questions, but also other emergent themes (Green and Thorogood, 2009). Subsequently a grid was constructed for the codification of the identified categories. The administrators’ interviews and focus group were first analysed separately from the counsellors’ interviews and focus group. Because there were no significant differences in the categories analysed in this paper, we merged the two sets of data together. Counsellors and administrators differed significantly, however, in their perceptions of the organization of the call centre and of the ethical challenges raised by this type of emergency intervention (Renaud, Caron-Bouchard and Rousseau, 2013). The Ethics Review Board of the CSSS de la Montagne approved the protocol and informed consent was obtained from all participants.
3. Results
Quantitative results
During the autumn outbreak, media coverage of the H1N1 pandemic in Quebec increased sharply (n = 45 articles in the week of October 10, 2009 versus n = 109 in the week of October 24, 2009) and reached a peak during the week of November 7, 2009 (n = 273) (Figure 1). The proportion of H1N1-positive tests followed a similar trend during this time period: 4.20% in the week of October 10, 24.20% in the week of October 24 and 49.30% in the week of November 14. The volume of calls to Info-Santé in Quebec followed the same pattern as both the media coverage and the H1N1-positive tests, with a peak during the week of November 14, 2009 (n = 1752 per million). The volume of calls to Info-Santé was slowly decreasing in December 2009 but there was still a large number of calls concerning H1N1. For example throughout the week of December 19, 2009, the volume of calls was elevated (n = 195 per million), even though media coverage of the H1N1 pandemic (n = 46 articles) and the proportion of positive tests (3.60%) had drastically decreased, suggesting a persistent fear and unrest among the population.
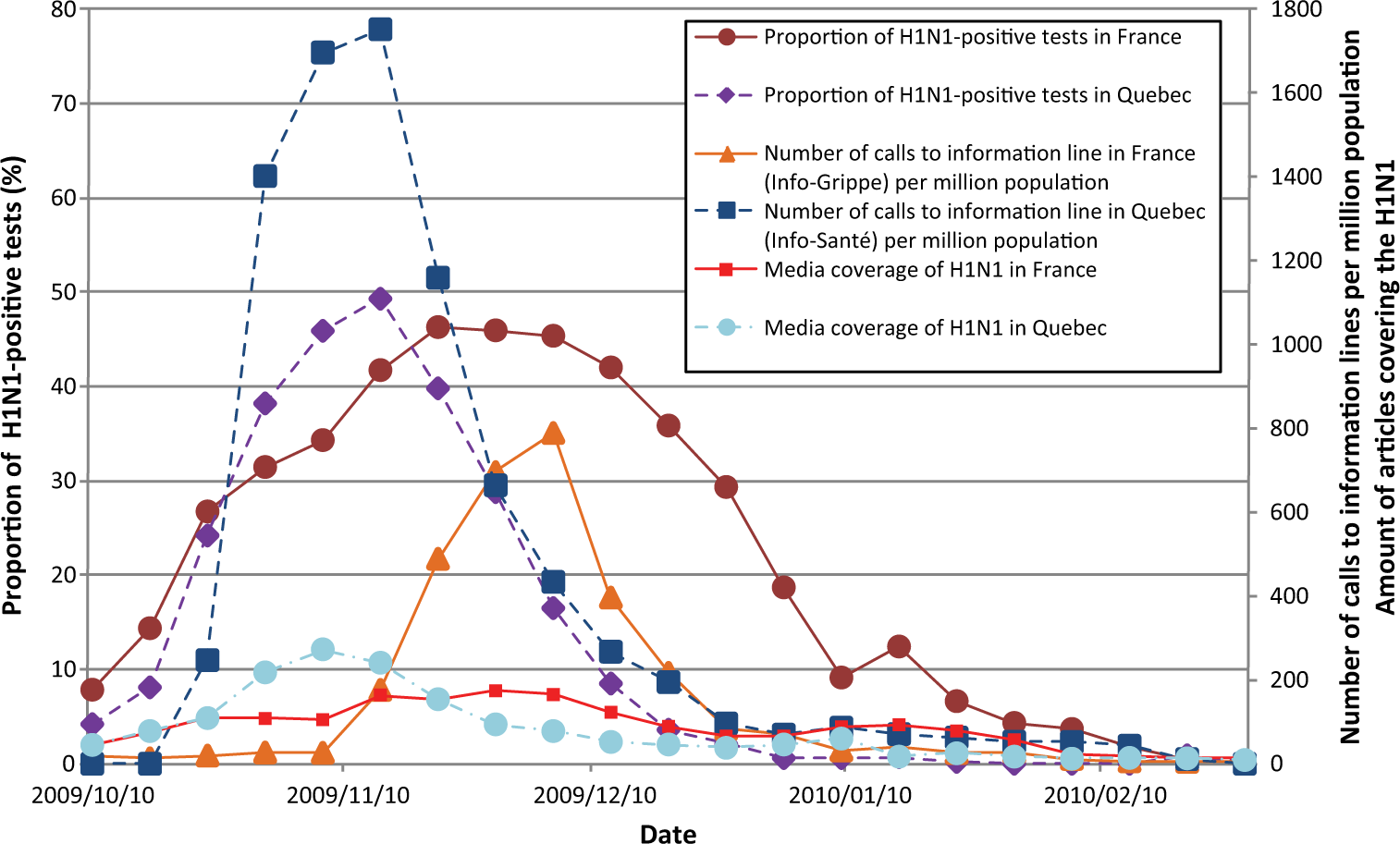
Comparison between the proportion of H1N1-positive tests, media coverage of H1N1 and call volume to information lines in France and in Quebec.
In France, the media coverage increased slowly, reached a plateau the week of November 14, 2009 (n = 164) and remained stationary until December 5, 2009 (n = 165). The proportion of H1N1-positive tests reached a peak in the same period (n = 46.30%; week of November 21, 2009) but started increasing before the media coverage and both then declined simultaneously. The number of calls to Info-Grippe increased sharply after November 7 (18-fold between the week of November 14 and November 21, 2009), at least one month after the rapid increase in H1N1-positive tests, and declined more rapidly than the proportion of positive tests, suggesting that the request for information was more linked to the public discourse about H1N1 than to the actual cases.
Seasonal flu immunization after H1N1
Within the senior population (aged 65 and older), the seasonal vaccination rate dropped significantly in Quebec following the H1N1 pandemic (60.5% to 40.9%; p < 0.05), while it had not undergone a significant drop in the French seniors (62.6% to 61%; p = 0.54) (Figure 2). In Quebec, the seasonal vaccination rate for the general population of 12 years and older dropped from 28.1% to 14.7% between 2009–2010 and 2010–2011 (p < 0.05) while it had never been lower than 25% since 2005. Figures for the general population are not available for France.
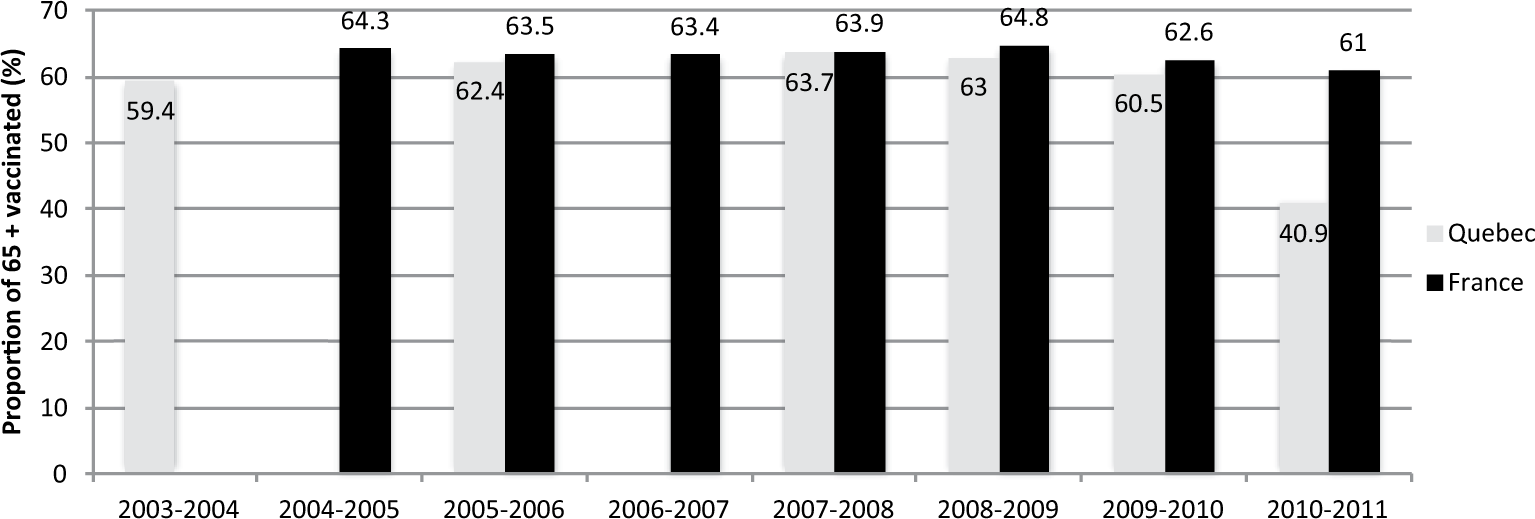
Proportion of population over 65 years vaccinated against seasonal influenza.
Qualitative results
H1N1, media and risk perception
According to the medical information phone line personnel, the number of calls received during the H1N1 spring and autumn outbreaks was directly linked to the information broadcast on radio and television. Both in Quebec and in France, the counsellors were unanimous in associating the upsurge of worry, and feelings of threat and panic with the release of H1N1 related information in the news. “Probably the media amplified the anxiety level among the public. Just to tell you, we were not able to keep up with the number of calls” (clinical counsellor, Quebec). “It was often because of the media that there were enormous waves of calls” (counsellor, France).
In both sites, the phone lines were flooded by the number of calls (up to 20,000 per day) and had to adjust their response strategies rapidly in order to meet the growing demands. The popular worries were numerous and often expressed with a range of significant emotions, from light anxiety to panic, from frustration to open anger. The events that triggered the feelings of threat were different in Quebec from those in France but remarkably, in both sites, geographically distant events elicited as much fear as did local ones and were often reported and discussed as if they had happened locally. For example, in France, the Mexican H1N1 outbreak was perceived as a very close event, geographically speaking, and provoked waves of anxiety related calls. This was not so much the case in Quebec, despite the relative greater geographical proximity. In Quebec, however, an adverse reaction to the vaccine which had occurred in the United States (a Guillain–Barré syndrome) was commented on and was discussed as if it had happened locally.
The events that triggered the most important waves of calls were related both to mortality and morbidity events and to concerns about the safety and availability of the vaccine. In Quebec, two mortality events covered widely by the media were turning points after which the Info-Santé line was overwhelmed: People’s worries increased after the death of the young boy [a 13-year-old Ontarian], when it was announced by the media […] people wanted to get immunized. At the beginning, it took time to get started [the vaccination campaign]; but when this death happened, suddenly, people panicked for their children and for themselves. (Quebec) What triggered the problem among pregnant women was the death of a woman in Vancouver. To my thinking, it was one of the triggers because not only was she in good health but she was also pregnant. It was because of this that there were so many questions about the vaccine for pregnant women: when would it arrive? These women’s anxiety considerably increased then. (Quebec).
According to the Info-Santé counsellors (Quebec), at least 50% of the calls came from people who were very anxious but did not have symptoms. The counsellors felt that the people who consulted them about symptoms, either for themselves or for their families, were often less anxious. The majority of the time, the reported symptoms were insignificant clinically. In France, the upsurge in anxiety was associated with the Mexican events that in fact took place before the spring outbreak: The images! There are images that are striking you know; they were showing people in Mexico, everybody with masks. This is a powerful image. Then you need to calm things down, they [the media] were feeding it … they were showing the hospitals and people waiting in lines, so, really it was something scary. (France)
During the autumn outbreak, the French counsellors estimated that 60% of the calls were criticizing the government’s choices. The callers considered that the counsellors represented the Ministry of Health and expressed their bitterness and fears related to the media debate about the risks associated with a rapidly produced vaccine, which had not undergone the standard tests. This appeared to be at the forefront of the French public’s worries.
In both sites, the phone line counsellors complained about the huge gap between the speed at which the media provided information and the relatively slow pace of response from the public health officials. In France, the Ministry of Health was sending a detailed press review to the counsellors daily. The phone line counsellors reported constantly watching television and reviewing the written press in order to prepare themselves to provide informed responses.
We stayed tuned to the more popular channels […] we were also watching when they were giving our telephone number, because we could receive 250 calls in the following 15 minutes […] we needed to have an idea of what was being said to be able to provide the appropriate answers. (France)
In Quebec, the counsellors also felt that the media had much more information than what they were given by the public health authorities.
At the beginning, we had a certain amount of information. But as the media were increasingly talking about it, often something would pop out in the media and we did not know anything about it. This would happen often. The public was then asking us questions and we would receive answers maybe 24 or 48 hours later. We needed to be honest and answer according to what we knew. But because we often did not know, people would sometimes be frustrated. (Quebec)
Time, thus, became a key issue both at the internal administrative level in order to be able to handle the volume of calls, and at an inter-institutional level, thereby challenging the communication speed and response capacities of public health and governmental agencies.
Credibility of voices and messages
Confronted with multiple sources of information on H1N1, the public had to try to make sense of all the things they read or heard in the media in order to choose a course of action that would protect themselves and their families. The relative credibility of those sources was at the forefront of the worry expressed to the counsellors. Major differences emerged between France and Quebec in the perceptions of who was in charge and who was credible. According to the Info-Grippe counsellors, the French public space was dominated by very heterogeneous and contradictory messages. First, public health and government representatives advocated for immunization, often referring to visual representations to convey their message: I remember that Mrs Roselyne Bachelot [Ministry of Health] did it in front of the cameras, to reassure people. And it’s true that the fact that she got the vaccine like that, live, on television, if there were people who did not believe in it, it calmed the French, because I felt we had fewer calls in the following days and people were much calmer on the phone.
The confusion was exacerbated by the fact that the communications between the call centre and the Ministry were very slow. For example, all the counsellors reported having learned about the French government immunization plan through the media and by the people who were calling in to the call centres to obtain information. Government spokespersons were not considered credible and numerous callers mentioned the Chernobyl catastrophe to justify their doubts about the official discourse, remembering that the government minimized the dangers associated with radiation: People were saying: the government will put us aside, as they did for Chernobyl, they told us at that time not to worry, and in the end, there were deaths and cancers. Now it is the same thing; they tell us it’s [the vaccine] innocuous! (France)
The Info-Grippe counsellors felt that, overall, the media conveyed very negative information about immunization. They gave a lot of space to experts who were strongly against immunizations.
From the beginning, there were experts on television who were saying “No, you should not get immunized” and a lot of doctors were saying the same thing. And the media would say that doctors were refusing the vaccine, when in fact, those working in hospitals were beginning to receive it. (France) My doctor was against it a week ago and now he is telling me I should get immunized. I do not know what I should do. (France)
In this chaotic information context, erroneous pieces of information were eliciting panic reactions. For example, many people called in regarding the shortage of Tamiflu, which had been wrongly announced in the French media. The rapid changes in immunization procedures and guidelines also fuelled distrust: for example, the shift from two doses to a single one for child immunizations. The fact that family doctors, who are traditionally in charge of immunization in France, were not involved in the H1N1 campaign further shattered the trust by the public in the government-established centres.
In Quebec, the press council decided to coordinate the dissemination of information, giving priority to the government-supported public health plan information. Very few divergent or critical voices were heard. Info-Santé counsellors emphasized that there was certain confusion but that it came mainly from shifts within the official discourse, as new information was emerging on who the at-risk groups were or on the relative safety of the vaccine for specific groups. People reported feeling that the media were dramatizing the situation while others reported distrust and doubt about the official discourse and strategy, alluding, in a few cases, to conspiracy theories. After the first few weeks, more calls were mentioning international sources of information usually obtained through the Internet, international media or family members living abroad. These pieces of information raised doubts about the national strategy: “People would say for example: ‘Why are people in France refusing to get the vaccine? Why should we get the vaccine? My sister-in-law in Paris said that she will not get it’” (Quebec).
In both sites, the H1N1 information lines were used extensively to confirm information or confront contradictory pieces of news. The confirmation of information appeared to be a way to resolve the relative confusion that dominated the public discourses on H1N1, even when all the players rallied around a common position, as happened in Quebec. In both sites, because of the multiple shifts in the public health implementation strategies of the immunization plans, it was not easy for the counsellors to reassure people, nor to convey a sense of clarity. Puzzled by distinctly varied sources of information, people were calling to express their dismay and, sometimes, their anger and to try to sort out the value of the divergent information.
In France, the overall confusion increased feelings of fear linked to uncertainty. As one of the counsellors reported “What they were seeing in the media was somehow shocking and they were asking: ‘Who is right?’” Another one commented: “Media were saying one thing and we, another. People did not know whom to believe anymore … It was very hard to try to counteract all these stupidities”. The people who called were often assigning the truth or the lie to one side or the other, in a climate of heightened anxiety.
In Quebec, although the majority would try to make sense of the homogeneous yet changing official positions, as time went on people began using international information and information gathered through the new social networks, to express their doubts about the seemingly very coherent official message conveyed by the media, thereby looking for alternatives.
4. Discussion
During the autumn outbreak of the pandemic, the proportion of H1N1-positive cases in Quebec and in France was similar but the volume of calls to the information line was very different. Indeed, in Quebec, there were proportionally more calls to the information line than in France. This difference could be explained by the local tradition associated with the use of medical information lines in each region. Although both regions adapted their phone line to respond to the increasing volume of calls, during the pandemic, Info-Santé (Quebec) was already a well known resource for the population who use it regularly for a variety of health issues while Info-Grippe (France) had a limited mandate only targeting flu prevention measures. This difference, which could explain the relative difference in the volume of calls, suggests that the effectiveness of call information centres may be related to the population’s familiarity with them.
As expected, the results confirm that media coverage of a health crisis is a major determinant of risk perception and of its associated emotional responses, mainly documented here through anxiety, discontent and information seeking behaviours. The relation between media coverage of specific emotionally laden events and waves of calls is present in both Quebec and France. The type of events associated with worry or panic reactions differed in the two sites. In Quebec, two mortality events (a 13-year-old youth and a pregnant woman) acted as the main triggers of the anxiety reactions. In France, the Mexican crisis (although more geographically distant than for Quebec) and the controversy around the vaccine safety (November 2009) were at the forefront. In both sites, the broadcasted information seemed to be, at first, taken at face value. But subsequently, feelings of confusion and uncertainty emerged. Beyond these similarities, the fact that key events for Quebec were mortality–morbidity-related may reflect the relative homogeneity of public discourse and media coverage of the crisis that converged in presenting H1N1 as a threat and in minimizing the potential problems associated with the vaccine. Rachul et al. (2011) analysed Canadian newspaper article content and documented that 71.8% of the articles provided reasons for getting vaccinated, whereas reasons against vaccination appeared in only 18.4% of articles. According to their results, Canadian newspaper coverage was largely supportive of the H1N1 vaccination programme and the associated high vaccine coverage supported the idea of a strong relation between media portrayals and vaccine uptake. Interestingly Massé et al. (2011), in an analysis of popular risk perceptions and expert discourses in Quebec during the H1N1 pandemic, emphasize rather the heterogeneity of local discourses. This apparent paradox suggests that the relative level of discourse, either homogeneity or heterogeneity, may be better appraised by both a comparative transnational perspective and an in-depth local analysis. A relative homogeneity might not exclude multiple forms of heterogeneity. Understanding which elements are related to this fine balance and influence preventive behaviours is a challenge.
In France, the more conflictual and heterogeneous public debate may have been associated with the shift from the H1N1 risk focus at the beginning of the crisis to a vaccine risk emphasis during the autumn outbreak (Bulifon et al., 2010). (Although the latter is also present in Quebec, it is minimal when compared to the French uproar.) Through a French public survey, Schwarzinger et al. (2010) confirm that although 37.1% of respondents were worried about H1N1 severity, 66.5% were concerned about vaccine safety and 78.8% refused the vaccine, feeling that the vaccination risks exceeded the benefits. It is to be noted that despite the low overall vaccination rate in France, vaccine uptake for at-risk children was relatively higher (31.8%) than for the rest of the population, suggesting that subgroups of a population may be using the circulating discourses in different ways (Weil-Olivier and Lina, 2011), although overall, the coverage rates for at-risk groups were deemed insufficient (Guthmann et al., 2010).
In both sites, the Internet and the new social media were also quite influential (Chew and Eysenbach, 2010; Larson et al., 2011). In France, they mirrored and fuelled the heated public debate. In Canada, as reported by the phone line counsellors, they provided a more critical forum in which key themes, often not aligned with official information, were discussed as relevant in the decision-making process (Henrich and Holmes, 2011).
The qualitative results suggest that the relative credibility of the different circulating discourses was directly linked to public trust in the vaccine. In Quebec, health professionals, experts and politicians, supported by the media, were relatively united around a consensual support for vaccination. This was also the case in Switzerland, where experts and political and health authorities were depicted as heroes and considered highly credible, while media and the pharmaceutical industry were distrusted (Wagner-Egger et al., 2011). In France, although family doctors were considered credible, they were not at the forefront of the vaccination campaign (Nougairède et al., 2010). Politicians and health authorities were generally distrusted. Interestingly, the main reason at the root of this distrust is the government’s previous minimization of the health hazards associated with Chernobyl, indicating that shattering public trust in different health-related issues may have a crossover effect years later when facing a pandemic. Exploring cross-cultural responses to the H1N1 pandemic, Poland (2010) demonstrated that trust in government and public health authorities is required to insure high vaccination rates. Levels of public trust are, however, highly variable and appear to be context-specific. Larson et al. (2011) argue that a thorough understanding of a population’s specific concerns, historical experiences, religious and political affiliations and socio-economic status is needed to plan an effective vaccination campaign.
In Quebec, the significant decrease in seasonal flu vaccination after the H1N1 pandemic validates Washer’s (2011) concerns about the potential danger of relentless and ever-increasing-pitch risk discourses. Exaggerated predictions of risk appear to lead to scepticism with people tuning out or becoming sceptical. Quite opposite media coverage strategies seem to have similar effects. In Quebec, the relative silencing of dissenting voices gave good results in terms of an immediate mass adhesion to the vaccination plan. In the aftermath, however, it may have undermined the health authorities’ credibility by giving the public the impression that they were manipulated and not given the appropriate information to make an informed choice (Davis et al., 2011). At the opposite end of the debate, in France, the relative innocuousness of the H1N1 outbreak may have reinforced the public discourses advocating against this particular vaccination, while it did not affect other well established preventive behaviours related to the seasonal flu immunization.
These observations raise important questions about the pros and cons of different communications strategies in times of health crisis. On one hand, advocating for clear, consistent and simple information and for coordination between public health officials, governments and the media appears to be effective in promoting a preventive behaviour (Kavanagh et al., 2011). On the other hand, considering the population’s heterogeneity and not minimizing their agency may also be essential, although complex. Contextualizing the information to assist the person in the understanding of personal relevance (Fogarty et al., 2011) and establishing a systematic dialogue with the public, in anticipation of such events, may be interesting avenues to explore (Davis et al., 2011). There is a clear lack of evidence about the validity of these diverse strategies and the present retrospective examination of the H1N1 experience invites one to be prudent, indicating that the balance between over-exaggeration and minimization is not easy to maintain and that both sides are associated with medium- and long-term effects which may have considerable consequences in the advent of a more serious health crisis.
5. Limitations
This paper has a number of limitations. First, because the same statistics were not available in both France and Quebec, the comparison of the subsequent immunization rates relies on indicators for an at-risk group. Second, the media coverage is estimated through an analysis of the coverage in the five top newspapers for each region (Quebec and France). This information identifies solely the newspapers with the highest readership and is not sensitive to regional variations. Nonetheless, this constitutes an indication of the variation in the media coverage over time. To complete this partial indicator, several articles concerning the media coverage were used in the literature review to analyse the content of the coverage and its impact on the population. Third, the information seeking behaviour is not a direct measure of risk perception. However, it may be a more objective measure of the level of perceived threat, than a direct question that will elicit a focussed emotional answer not necessarily related to actual fear-related behaviours. Fourth, Info-Santé recorded all the calls, but Info-Grippe did not. It was therefore impossible to compare the discourse of the subjects themselves and we had to rely on the counsellors’ and administrators’ reports which were not collected by the same method in both Quebec and France. Fifth, independently from communications strategies, wide differences in the organization of immunization campaigns may also have contributed to the widely different immunization rates, but the analysis of these organizational differences was beyond the scope of this study. Finally, the socio-demographic profile of the persons who receive seasonal immunizations may differ significantly from those who received the H1N1 vaccine. The decrease in seasonal immunization rates in Quebec may thus be related to other factors than the H1N1 impact on public perceptions.
In spite of these limitations, the results of this study suggest that public risk perception is constructed both locally and globally through social media and that the use of fear to influence health behaviours may be a double-edged sword. Further studies will need to examine carefully the trade-off between public mobilization and its impact on the future trust in health authorities.
Footnotes
Acknowledgements
We want to thank, in Québec, Rosane Lachance and the personnel of Info-Santé and, in France, Maurice Quéré, Antoine Siossac, Gerard Dhesse, Bernadette Murgue and the personnel of Info-Grippe.
Funding
This study was supported by a grant from the French Institut de Microbiologie et Maladies Infectieuses – Programme de Recherche A (H1N1), and was carried out under the coordination of the CNRS Laboratoire d’Ethnologie et de Sociologie comparative, France.