
Abstract
Objective
To synthesize the effects of educational intervention on the screening rate of first-degree relatives of cancer patients.
Methods
A total of eight Chinese and English databases were searched (PubMed, Embase, Cochrane Library, CINAHL, Web of Science, Scopus, Medline and China Biology Medicine disc) from the time of library establishment to June 2023, for randomized controlled trials investigating the effects of educational intervention on screening rate of first-degree relatives of cancer patients. Two researchers independently screened and evaluated the quality of studies. RevMan 5.3 software was used to calculate the pooled effect size.
Results
Thirteen studies involving 5628 participants were chosen to include in the meta-analysis. The results revealed that health education can increase screening rate of first-degree relatives of cancer patients (RR = 1.39, 95% CI = 1.16–1.65, P = 0.0002). The effect shown after short-term follow-up (≤6 months) was insignificant in terms of improving screening rate (RR = 1.46, 95% CI = 0.94–2.26, P = 0.09), but after long-term follow-up (>6 months) the improvement was greater (RR = 1.37, 95% CI = 1.13–1.65, P = 0.002).
Conclusion
Health education is effective in increasing the screening rate of first-degree relatives of cancer patients. The effect is more evident after long-term than short-term follow-up.
Introduction
Cancer is predicted to become the leading cause of premature death globally in the twenty-first century
First-degree relatives (FDRs; parents, siblings, and children only) of cancer patients were considered as the target population for screening9,10; some studies have shown that FDRs of patients with breast cancer, 11 colorectal cancer (CRC), 12 gastric cancer, 13 skin cancer, 14 etc. should be screened regularly. Among FDRs of gastric cancer patients, the odds ratio for relative risk (RR) of gastric cancer development fluctuates between 2 and 10 across different races and regions, 13 and a global study found that about 25% of CRC patients had at least one FDR with the same disease. 15 Standardized monitoring according to clinical guidelines was recommended for the FDRs of CRC patients due to their risk of CRC being 2–4 times higher than that of the general population. 16 A biennial consultation with a total cutaneous examination was determined to be cost-effective for the FDRs of cutaneous melanoma patients in a computer simulation study conducted in the United States before the contemporary era of effective but expensive medical treatments for advanced cancer stages. 17 Currently, it is recommended that FDRs of CRC patients younger than 60 years old should undergo colonoscopy at age 40 or 10 years before the age of diagnosis of the first CRC patient in the family (e.g. the patient was diagnosed at 48 years old, so FDRs should undergo colonoscopy at 38 years old). The frequency of screening should not be less than once every 5 years. 18
Although routine screening for FDRs has been recommended, compliance remains low. The screening rate of FDRs of CRC patients has been reported as only 14%–40%, 19 and in an Australian study the self-reported lifetime screening adherence of FDRs at slightly above average risk was 47%. 20 Other studies21,22 have suggested that compared to people without a family history, FDRs are more likely to consent to engage in screening, but they are not more likely to comply with testing. One explanation for this low adherence was that previous participants appeared to have insufficient understanding of appropriate risk-based screening intervals. Only 22% of those with hereditary non-polyposis colon cancer and 52% of individuals with a familial history of CRC were aware of the recommended colonoscopy screening frequency based on their family background. 23 There were other influencing factors, including fear of cancer, lack of screening information, discomfort of examination, radioactivity of examination, no time to wait, lack of health insurance, low level of income, etc. 11 Low screening participation rates are a global issue, and it is important to find an effective approach to facilitate the screening of FDRs.
The World Health Organization promotes health education to improve the awareness and understanding of how to keep healthy and prevent disease, including information on available resources and the benefits of accessing services. 24 Health education should promote a healthy lifestyle and change unhealthy behaviour by changing people's cognition of disease, and thus improve health literacy. 25 It has been shown that health education can raise the aggregated demand of women for cervical cancer screening 26 and acceptance of the pap smear 27 ; it can also as increasing the screening rate of CRC. 28 However, some studies have given different results, such that health education was not likely to positively influence screening behaviour for FDRs of breast cancer or CRC patients.21,29
Information on cancer screening is delivered in various ways, which include telephone calls, educational brochures by post, peer education, counseling sessions, customized tutorials, face-to-face interviews, lectures, films, group discussion, etc. 24 Health education may be an effective way to improve screening acceptance among those at high risk such as FDRs of cancer patients. Although some scholars have begun to pay attention to this important group and carry out relevant research, difficulties are created in the screening management of FDRs by ambiguities in detailed strategy, intervention duration, etc., of the health education reported in these studies as well as the differences in results, and the strength of evidence is still not clear. Up to now, there has been no relevant systematic review published. The aim of this study was to explore the influence of health education on the screening rates of FDRs of cancer patients by the method of systematic review and meta-analysis, so as to provide useful information as the basis for future research.
Methods
Registration
This systematic review was registered at PROSPERO(CRD42023464678).
Search strategy
PubMed, Cochrane Library, Web of Science, CINAHL, Scopus, Embase, Medline, China Biology Medicine disc (CBMdisc) were systematically searched from establishment to June 17, 2023. The search strategy was set up by working with the librarian. The search adopted a combination of subject word and random word which included Neoplasms (i.e., neoplasms OR tumor OR cancer OR neoplas*), Screening (i.e., screening OR mass screening OR early detection of cancer), first degree relative* (i.e., first degree relative* OR relative OR family OR military family), and Randomized Controlled Trial (i.e., randomized controlled trial OR controlled clinical trial OR random*). A search alert was set to receive any updated studies after the search date.
Inclusion and exclusion criteria
The inclusion criteria included: (1) Participant: FDRs (only parents, children, and siblings) of cancer patient of 18 years or older; (2) Intervention: the types of health education intervention content were general knowledge of cancer, risk factors, family history, screening methods, screening recommendations, solutions to common screening barriers, etc. The intervention methods included telephone calls, peer education, customized tutorials, face-to-face interviews, lectures, etc. (the specific intervention methods were not restricted); (3) Comparators: the groups that received usual care;(4) Primary outcome indicators: the screening rate of cancer, the proportion of participants in cancer screening by the follow-up time, the main measuring method was self-report of FDRs with their inspection results; (5) Study type: randomized controlled trial; (6) Publication date: unlimited; (7) Publication language: English or Chinese.
The exclusion criteria included: (1) study subjects included both FDRs and second-degree relatives (uncle, aunt, cousin, etc.) but the data were mixed; (2) FDRs themselves are diagnosed with cancer; (3) books, editorials, comments, and meeting minutes without data.
Data extraction
Endnote X9 was used for data management. The first author selected titles and abstracts of the study, and the corresponding author reviewed them. The full text review was completed by the first author and the third author independently, and was discussed and confirmed with the second author in case of disagreement occurring. The two reviewers of full text performed information extraction independently by using a unified custom information extraction table. The information extraction table includes first author, publication year, country, cancer types, mean age, sample size, intervention, comparison, theoretical model, implementer, follow-up duration and outcome indicators.
Quality assessment
The quality assessment of included studies was conducted independently by two reviewers using the Cochrane Collaboration Risk of Bias Tool for randomized controlled trials. 30 Quality was appraised from seven aspects: random allocation, protocol concealment, blinding of subjects and researcher, blinding of outcome measures, selectivity reporting study findings, and other bias. The assessment levels included “low risk”, “possible risk” and “high risk”. Two researchers (the first author and the third author) discussed the evaluation. A third researcher (the second author) was consulted if there was a great discrepancy.
Statistical analysis
The Review Manager Software (Revman 5.3) was employed to carry out the meta-analysis. Individual study effect sizes were calculated using relative risk (RR), and the same outcome variables were utilized in the meta-analysis. To calculate the pooled effect, the overall RR and 95% confidence interval (CI) were employed. The studies’ heterogeneity was evaluated using the Chi-square and I-squared (I2) statistics. 31 Data analysis should implement meta-analysis of fixed effect model if I2 < 50%; when I2 ≥ 50%, it should find the source of heterogeneity by implementing subgroup analysis or sensitivity analysis, and it should implement meta-analysis of random effect model if the heterogeneity still cannot be reduced.
Results
Search results and study selection
A total of 5749 studies were retrieved; 1184 studies were excluded through EndNote and manual duplicate checking, 4540 through preliminary reading of titles and abstracts, and 12 through full text reading; so 13 studies were ultimately included in the review.14,32–43 The detailed screening process is shown in Figure 1.

The PRISMA flow chart of this review.
Characteristics of included studies
A total of 5628 cases of FDRs of cancer patients were included in the 13 studies, which contained 2825 cases in the experimental group and 2803 cases in the control group. All included studies were published during the period of 2006 to 2022. The cancer types involved were breast cancer, 32 CRC33–41 and melanoma.14,42,43 The trials were distributed in Australia, 37 China, 40 France,14,39 Iran 33 and USA.32,34–36,38,41–43 The intervention content contained general knowledge of related diseases, risk factors, family history, screening methods, screening recommendations, solutions of common screening barriers, etc. Intervention approaches included telephone interventions,32,33,36,41 individualized print intervention,35,37 face-to-face health consultation, 34 mail (letters) interventions, 41 network interventions,38,40,43 nurse-led interventions, 39 etc. The theories or models adopted included: Precaution Adoption Process Model (PAPM), 34 Health Belief Model (HBM),35,40 Transtheoretical Model/Stages of Change Theory (TTM), 35 Motivational Interviewing (MI), 33 Social Cognitive Theory, 42 Theory of Planned Behavior. 42 Detailed information is shown in Table 1.
The characteristics of included studies (n = 13).
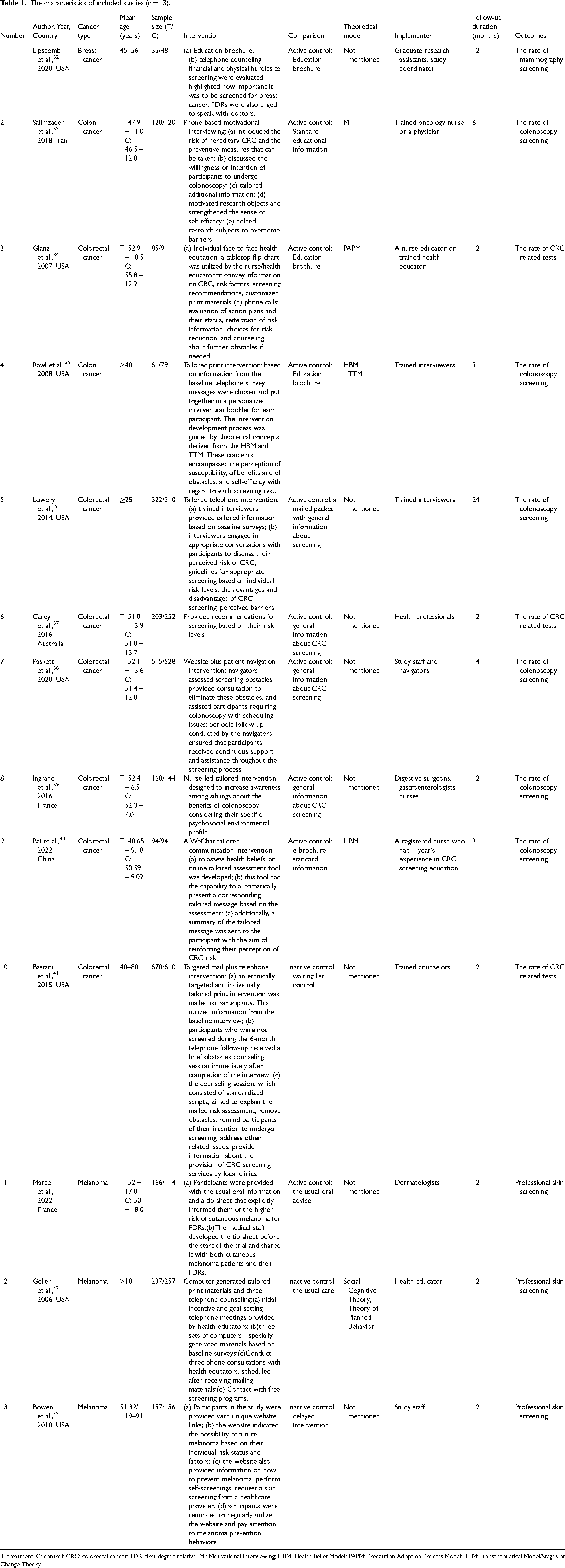
T: treatment; C: control; CRC: colorectal cancer; FDR: first-degree relative; MI: Motivational Interviewing; HBM: Health Belief Model: PAPM: Precaution Adoption Process Model; TTM: Transtheoretical Model/Stages of Change Theory.
Quality assessment of included studies
Of the 13 randomized controlled studies reviewed, 11 mentioned how the randomization was done and were rated as low risk of bias, but two studies32,34 didn’t expound the detailed generation methods of random allocation and so received an unclear risk of bias rating due to insufficient information. Only one study 40 gave information about the allocation concealment, which was indicated as having a low risk of bias; the remaining studies had an unclear risk of bias for this aspect. Only one study 37 mentioned how blinding of participants was implemented, and was rated as low risk of bias. Three studies33,38,43 explained the blinding method for surveyors, and were rated as low risk of bias. Because the main measuring method was self-reporting by FDRs with their inspection results, the surveyors would then verify the results with related medical institutions; therefore, the effect on results collection was small, whether surveyors used a blinding method or not. All the studies report the number of cases lost, but most did not implement ITT (intention-to-treat) analysis. All the studies report the outcome indicators in accordance with the proposal; the detailed results of quality evaluation are shown in Figures 2 and 3.

Risk of bias graph.

Risk of bias summary.
The effect of health education on screening rate of FDRs of cancer patients
The meta-analysis demonstrated a high degree of heterogeneity among studies in terms of screening rate (I2 = 85%, P < 0.001), and the random effects model was adopted. The findings indicated that health education had a beneficial effect on the screening rate of FDRs of cancer patients when compared to the control group (RR = 1.39, 95% CI: 1.16–1.65, P = 0.0002). The results are shown in Figure 4.
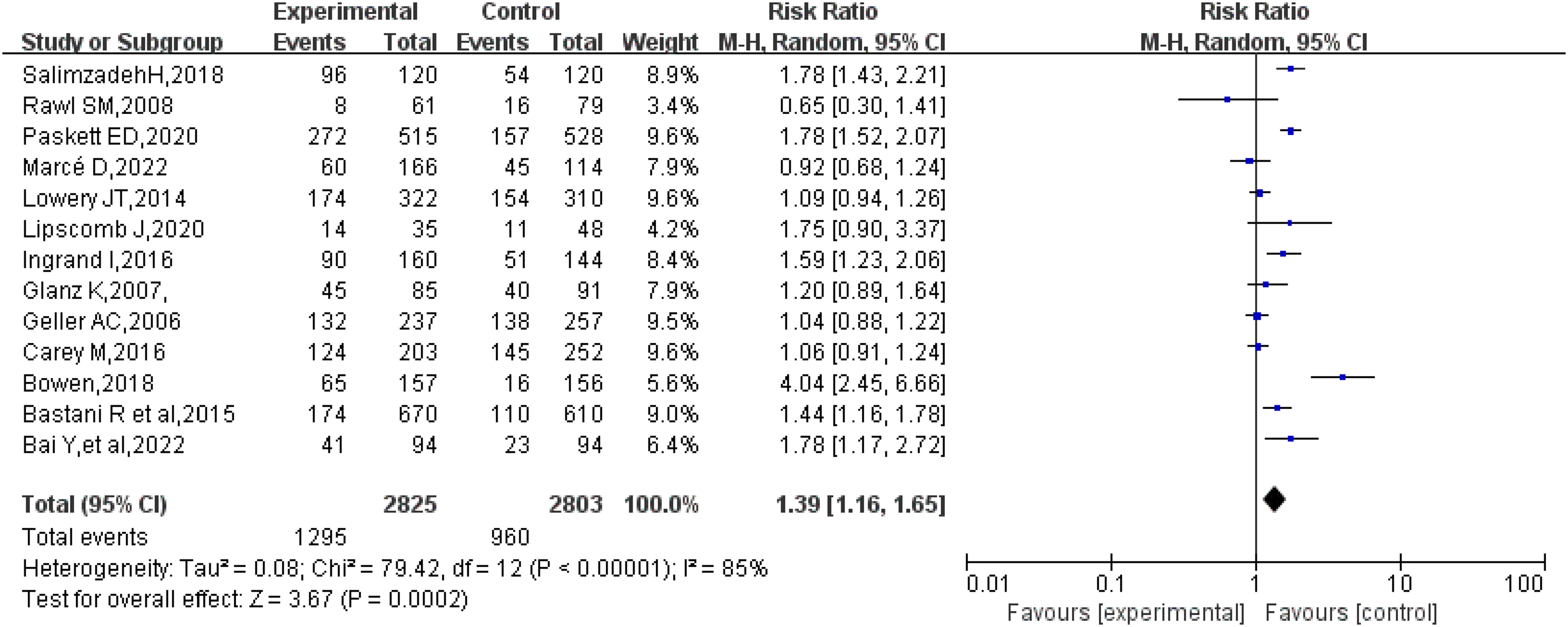
Effects of health education on the screening rate of FDRs of cancer patients.
The effect of follow-up duration on screening rate of FDRs of cancer patients
Considering that the duration of follow-up might be the reason for clinical heterogeneity, subgroup analysis was conducted separately for short-term (≤6months) and long-term (>6 months) follow-up. Random-effect analysis indicated that there was no effect after short-term follow-up (RR = 1.46, 95% CI: 0.94–2.26, P = 0.09). After long-term follow-up, the effect of promoting the screening rate was shown (RR = 1.37, 95% CI: 1.13–1.65, P = 0.002). Detailed results are shown in Figure 5.
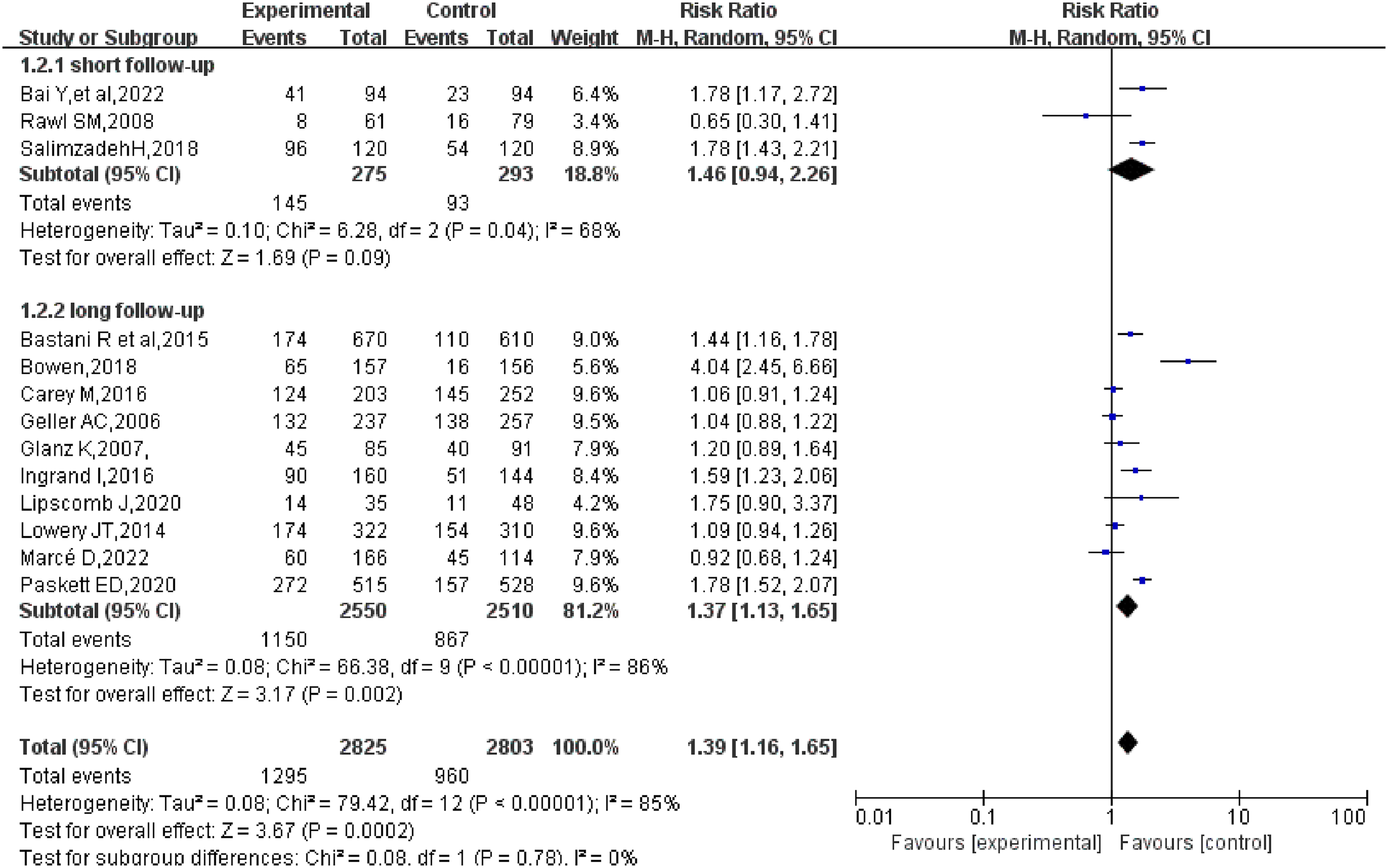
Effects of follow-up duration on screening rate of FDRs of cancer patients.
Discussion
Characteristics of studies included in systematic reviews
The 13 studies reviewed here were published between 2006 and 2022; three of them were published before 2010 and 10 after 2010. The increase is probably because more scholars started to pay attention to the issues of FDR screening in recent years, so more intervention strategies were used to improve screening rate. The main strands of health educational content were general knowledge of disease, risk factors, screening approaches, screening recommendations, the solutions of common screening barriers, etc. Most of the health educational methods were traditional, such as telephone interview, mail and print intervention, etc. Some studies had begun to implement intervention by adopting modern network technology; for instance, Bai 40 developed an online customized evaluation tool: after entering general demographic information, family history, health belief regarding examination of CRC and colonoscopy, and response of measuring instrument, this tool presents customized information automatically, so as to implement relevant health education for the individual participant. Lowery's study 36 indicated that counselling was conducted using Computer Assisted Telephone Interview software at the University of Colorado Cancer Center. The use of new technologies provides fresh ideas for intervention in future studies. The intervention implementers used in four studies33,34,39,40 gives an indication that nurses are the significant force in promoting early screening of cancer. This is consistent with previous research results,44,45 that nurse-led intervening measures play a positive role in the aspects of increasing acceptance rate of early cancer detection, cancer knowledge, belief in early detection, finding of precancerous lesions, etc. The important role of nurses in cancer screening and as promoters of health management should be further exploited in the future.
Health education is effective in improving screening rate of FDRs of cancer patients
There was no unified conclusion, among the studies reviewed, as to whether a health educational strategy can increase the screening rate of FDRs of cancer patients. Some studies23,32,38,46 indicated that health education was beneficial in increasing the screening rate of FDRs, while other studies11,21 reported that it had no effect on their screening rate. The results of meta-analysis showed that the screening rate of FDRs had increased, which was consistent with previous studies.23,47 The use of tailored health education attracted attention for its ability to enhance persuasiveness by conveying messages specifically targeted at individuals. This personally relevant approach increased the likelihood that the message would be read and cognitively processed by the participant. As a result, there was an increased chance of behavioural change with regard to screening. 40 Several studies14,32,36–38,41–43 indicated that working with families had been identified as a promising health education avenue for encouraging behaviour change. One method of achieving this was by identifying a case in the family and assisting with contact of other family members. Therefore, it was important for further research to identify possible mechanisms and ways in which familial attention to the problem could be increased. Additionally, exploring accessible conduits for working with families would be beneficial. The main reasons why health education promotes the screening rate of FDRs may include: (1) the FDRs could be influenced by health-care professionals in regard to perceptions of health and disease, which could encourage them to change their behaviour; in addition, specific obstacles to screening should have been resolved during the implementation process, and screening promotion accomplished as well. (2) The reported theoretical basis of many of the studies included in this systematic review gives a scientific guarantee of the validity of the intervention implementation. The theoretical models favoured included HBM, TTM, PAPM, Social Cognitive Theory, Theory of Planned Behavior, etc. It has been shown48,49 that these theories play positive roles in the aspects of health risk behaviour change, positive health behaviour adoption, and improved compliance with medical orders, and meanwhile can also improve the screening rate of cancer disease effectively.50,51 HBM was the model most used for promoting positive health behaviour of cancer patients; however, the method that combined other models with TTM was more effective than the others due to TTM being based on the stages of behaviour change, while other models showed the mechanism of creating behaviour; therefore, cancer education and health behavioural counseling based on the TTM model were beneficial to promoting healthy lifestyles. 52
The effect of follow-up duration on screening rate of FDRs of cancer patients
No effect after a short-term follow-up (≤6 months) is observed. This might be related to the small number of studies with short-term follow-up, being only three.33,35,40 It is also possible that changing the health behaviour is a long-term process 53 ; the studies of 3–6 months’ duration were insufficient in changing screening belief and overcoming screening barriers of FDRs adequately. Furthermore, 3 months may not be enough time to determine the level of screening participation adequately, with specialised screening methods such as colonoscopy. 35 Therefore, some researchers considered that the forward stage movement of TTM theory was an effective reference result beside the screening behaviour. 35 As the effectiveness of long-term follow-up has been proved,32,36,41 the expectation of future study is to implement short-term interventions with larger samples in order to verify its validity more accurately, as well as to provide strong evidence for subsequent intervention duration formulation.
Limitations
(1) The results of this study show considerable heterogeneity in spite of the implementation of subgroup analysis. Due to the commonality of screening experience, this study was not restricted to a specific type of cancer. The heterogeneity of the results is perhaps also related to the acceptability of different cancer screening requirements and the accessibility of resources. The outcome indicators for measurement were screening rates; however, different cancers require different screening programs. The screening requirement for FDRs of a melanoma patient was to implement a full-body skin examination by a professional, while the screening requirement for CRC was to implement colonoscopy, and mammography for breast cancer. Comparatively speaking, colonoscopy requires more mental and physical preparation, which would have a certain influence on screening rate. In addition, there are economic restrictions: the cost of colonoscopy was highest and the cost of mammography came second; however, the participants were allowed colonoscopy free of charge in one of the included studies, these factors perhaps contributed to the differences between the studies. Although agreement between studies was affected by many existing factors, the combined results still show that health education can generally promote the screening rate of FDRs of cancer patients. (2) Although the experimental data included in this study were all from randomized controlled trials, some of the studies didn’t further describe the allocation concealment scheme and the method of blinding intervention implementers, which might have an impact on the research conclusions of the article. (3) Since the studies were all published in English, there may be a degree of language and publication bias.
Clinical implications
Firstly, there are only three types of cancer included in this study, breast cancer, CRC and melanoma. The future expectation is to pay more attention to the screening of FDRs of patients with other types of cancer, and to explore more interventions that may promote screening in ways that are economical, scientific and efficient. Secondly, with the rapid development of social networking platforms, more and more people use We-Chat, WhatsApp, Facebook, etc. Internet-based communication channels are increasingly perceived as more convenient and cost-effective alternatives to telephone and print. Therefore, future studies could explore the use of new channels like the Internet and mobile devices, combining verbal and written information communication systems, to suit different situations. Thirdly, it is recommended that future studies should develop more specific assessment tools and response systems to examine how the evaluation of personal data influences the communication outcomes.
Conclusion
Despite the limitations mentioned above, our study provides a preliminary reference for promoting the screening of FDRs. Our research revealed that health education can improve the screening rate of FDRs of cancer patients, and the effect can be seen better after long-term than short-term follow-up. Further research involving larger samples is needed to explore more effective and convenient interventions that can improve screening rates.
Footnotes
Authors contributions
Jiaxun Kang, Jingna Yi, and Qiushi Zhang conducted the design of the entire study, Jiaxun Kang conducted the study retrieval and selection, and Qiushi Zhang reviewed the study selecting process. Jiaxun Kang and Jingna Yi conducted the selection of full text, Shanshan Wang took charge of the disagreements during the selecting process, Jiaxun Kang took charge of the article writing, Shanshan Wang, Jingna Yi and Qiushi Zhang revised the article repeatedly, and all authors confirmed the final draft.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by key R&D and promotion projects of Henan Provincial Science and Technology Department (Grant number: 232102310251).