
Abstract
Background:
Homeless persons in the United States have disproportionately high rates of illness, injury, and mortality and tend to believe that the quality of their end-of-life care will be poor. No studies were found as to whether nurses or nursing students require moral courage to help homeless persons or members of any other demographic complete advance directives.
Research hypothesis:
We hypothesized that baccalaureate nursing students require moral courage to help homeless persons complete advance directives. Moral courage was defined as a trait of a person or an action that overcomes fears or other challenges to achieve something of great moral worth.
Research design:
The hypothesis was investigated through a qualitative descriptive study. Aside from the pre-selection of a single variable to study (i.e. moral courage), our investigation was a naturalistic inquiry with narrative hues insofar as it attended to specific words and phrases in the data that were associated with that variable.
Participants and research context:
A total of 15 baccalaureate nursing students at a public university in the United States responded to questionnaires that sought to elicit fears and other challenges that they both expected to experience and actually experienced while helping homeless persons complete advance directives at a local, non-profit service agency.
Ethical considerations:
The study was approved by the Internal Review Board of the authors’ university, and each participant signed an informed consent form, which stated that the study involved no reasonably foreseeable risks and that participation was voluntary.
Findings:
Before meeting with homeless persons, participants reported that they expected to experience two fears and a challenge: fear of behaving in ways that a homeless person would deem inappropriate, fear of discussing a homeless person’s dying and death, and the challenge of adequately conveying the advance directive’s meaning and accurately recording a homeless person’s end-of-life wishes. In contrast, after their meetings with homeless persons, relatively few participants reported having encountered those obstacles. So, while participants required moral courage to assist homeless persons with advance directives, they required greater moral courage as they anticipated their meetings than during those meetings.
Discussion:
Our study breaks new ground at the intersection of nursing, moral courage, and advance directives. It might also have important implications for how to improve the training that US nursing students receive before they provide this service.
Conclusion:
Our results cannot be generalized, but portions of our approach are likely to be transferable to similar social contexts. For example, because homeless persons are misunderstood and marginalized throughout the United States, our design for training nursing students to provide this service is also likely to be useful across the United States. Internationally, however, it is not yet known whether our participants’ fears and the challenge they faced are also experienced by those who assist homeless persons or members of other vulnerable populations in documenting healthcare wishes.
Introduction and background
In the United States, homeless persons face enormous obstacles to healthcare, 1,2 and they have disproportionately high rates of illness, injury, and mortality. 3 –6 Furthermore, they tend to believe that the quality of their end-of-life (EOL) care will be poor. 7 In light of those findings, it is not surprising that some homeless persons show a strong interest in discussing EOL questions and engaging in advance care planning. 8 However, their limited access to primary care facilities suggests that they have few opportunities to complete advance directives (ADs). Additionally, efforts to assist them with ADs appear to be rare. Why might that be?
Our study began with the assumption that, for nurses and many others who are not homeless, helping a homeless person complete an AD can be accompanied by identifiable fears or other challenges. For example, it is common knowledge that, in the United States, homeless persons are deeply stigmatized and negatively stereotyped. As a result, many who are not stigmatized risk some degree of disrepute by having extended interactions with them. Because such disrepute—even if minor and temporary—is fearful and otherwise unsettling, it can form a barrier to interacting with homeless persons. Furthermore, many people are frightened by thoughts of death and scared to initiate conversations about it, especially during an initial encounter with another person. But helping a homeless person complete an AD can include precisely these experiences—added barriers to providing such assistance. So, because it can involve overcoming these fears, helping a homeless person complete an AD might require courage, we assumed. But not simply courage; it can demand specifically moral courage, we hypothesized. Before explaining that contention, let us survey how various scholars have spoken of “moral courage.”
In both philosophical literature and recent nursing research, “courage” has been understood in a variety of ways. Philosophers recognize that “courage” is a broad concept that denotes the surmounting of fear, but they often use the term in a specific, moral sense. They speak of “moral courage” as a component of virtuous character, for example, or as a property of certain actions that renders those behaviors morally good or right. 9 Taking their cue from these ways of articulating the concept, nursing researchers have studied the roles of moral courage in nurses’ character and practices. Treating moral courage as a virtue, Spence and Smythe, 10 for example, link it to other character traits, such as nurses’ possession of confidence in their clinical knowledge, a sustained commitment during times of strain, and the hope that things can always be made better. Similarly, Storch et al. 11 regard moral courage as a character trait that nursing leaders require to be self-reflective and to identify their own moral distress, while Arman 12 finds that moral courage is “a prerequisite inner quality” that nurses must possess before they can enter profound, caring relationships with patients. In contrast, some researchers seem to speak of moral courage as a property of an action that helps to make that act morally good or right. According to Thorup et al., 13 part of what makes it admirable for nurses to confront ethical dilemmas, for example, or to bear witness to patients’ suffering is that such acts exhibit moral courage. Such acts contribute to the ethical formation of the nurses who perform them, these researchers found, giving them moral courage to repeat such acts.
Prior to our investigation, there had been no studies as to whether nurses or nursing students require moral courage to help homeless persons or members of any other demographic complete ADs. We investigated whether baccalaureate nursing students required moral courage to help homeless persons complete ADs. This study is important for several reasons. First, for nursing students, helping homeless persons complete ADs is consistent with some of the responsibilities of the profession to which they aspire, such as preventing suffering and mitigating the social conditions that give rise to health-related inequalities. 14 In this respect, our study was not only concerned with instilling moral courage in students; it was also concerned with showing them the importance of social justice and demonstrating their power to promote it. Second, as some of the studies discussed earlier suggest, moral courage is a trait or behavior that can be learned and that is essential for success in nursing practice. 15 –17 Accordingly, by intentionally giving students an opportunity to practice moral courage, our study made a unique contribution to their professional preparation, for, in nursing curricula, such opportunities appear to be rare. 18,19 Similarly, students also engaged in professional preparation by caring for members of a vulnerable population, as they might be expected to do in their careers. 20,21 Furthermore, students learned about ADs and acquired skills that are likely to prove useful in their nursing careers when they help patients complete such documents—a task that, in practice, is often performed by nurses. 22 –24 Finally, as they learned about ADs and helped homeless persons complete them, students also learned about the value of facilitating another’s autonomy in relationship to EOL care. In connection with his father’s decisions and priorities near the end of life, surgeon Atul Gawande 25 writes, “This is what it means to have autonomy—you may not control life’s circumstances, but getting to be the author of your life means getting to control what you do with them.” An AD is a vehicle for such control when one no longer has the capacity to respond to one’s circumstances directly.
By design, our study avoided taking a side in the aforementioned debate as to whether “moral courage” is best understood as a worthy character trait or a property of certain admirable actions. Instead, adopting a broad, common sense understanding of the concept, we defined “moral courage” as a trait of a person or an action that overcomes fears or other challenges to achieve something of great moral worth. Other researchers have employed very similar definitions.
26
–28
We also assumed that, in general, articulating one’s EOL wishes (e.g. by completing an AD) is something of great moral worth, for, among other things, it is exercising one’s autonomy in an important area of life and healthcare, as noted above. Therefore, if a person overcomes fears or other challenges (e.g. fear of discussing death) to help another complete an AD, that person has demonstrated moral courage. More specifically, to explore the ways in which the nursing students’ participation in this project might have involved moral courage, we investigated two questions: Which fears or other challenges did nursing students anticipate they would face while helping homeless persons complete ADs? Which of those obstacles did nursing students actually face?
The distinction between these questions is significant. Before a person can engage in a certain action (e.g. skydiving), she might have to overcome fears or other challenges associated with her anticipation of what that action will be like, even if some aspects of that anticipation are misguided (e.g. the mistaken belief that she is very likely to be injured while skydiving). So, seeking a broad picture of the students’ experience, we sought to identify fears or other challenges that they encountered not just as they helped homeless persons complete ADs, but also before they provided that help, even if some of those fears or challenges were misguided or, in hindsight, could have been avoided. That broad picture of the students’ experience reveals much about what should be involved in training them to provide this service, as we will discuss.
Participants and methods
Our study followed a qualitative descriptive design 29,30 to investigate whether baccalaureate nursing students required moral courage to help homeless persons complete ADs. Aside from the pre-selection of a single variable to study (i.e. moral courage), our investigation was a naturalistic inquiry with narrative hues insofar as it attended to specific words and phrases in the data that were associated with that variable (e.g. “fear,” “challenge”). 29 Nursing students were the research participants, and questionnaires were used to collect data from them. Their responses were analyzed using thematic content analysis, as discussed below.
Ethical considerations
The study was approved by the Internal Review Board of the authors’ university, and each participant signed an informed consent form, which stated that the study involved no reasonably foreseeable risks and that participation was voluntary.
Participants
All of the baccalaureate nursing students enrolled in the honors sections of two courses, Community Health Nursing and Transcultural Nursing, fulfilled one of their honors requirements by first attending a training session and then helping a homeless person complete an AD at an AD Workshop. Additionally, students received an email inviting their voluntary participation in our study, which involved their completing pre- and post-Workshop questionnaires. Students were not required to participate in the study, nor did they receive credit or compensation for their participation. A total of 15 female students self-selected into the study, and all of them completed and returned the questionnaires.
The training session was held on the students’ campus and was led by the authors. During the session, students received health-related and other demographic information about homeless persons. Students also received general information about ADs and their uses in healthcare settings. The authors discussed possible treatment options that surface when ADs are completed, such as tube feedings and mechanical ventilation. The authors with ethics expertise summarized all of that information in a PowerPoint and then introduced students to the AD that they would be using during the Workshop—a form designed by Song et al. 31 specifically to accommodate many needs and concerns that are somewhat unique to homeless persons. Next, two of the authors illustrated the kind of encounter that each student would have with a homeless person at the AD Workshop by role-playing the completion of an AD, with the first author (W.N.) playing the part of a nursing student-interviewer, while the medical center ethicist portrayed the character of a specific, imaginary homeless person. Students then paired off to practice the completion of an AD, with one student serving as interviewer and the other answering the AD’s questions either in her own voice or, if she preferred, in the voice of an imaginary character. The training ended with the group’s reconvening to discuss the students’ paired-off experiences, which gave the authors an opportunity to clarify points and to address the students’ further questions about their role as interviewers and the role of a nurse in assisting persons to complete ADs.
A few days later, students were given an orientation to a private agency that delivers a variety of services (e.g. case management, meals) to many homeless persons in their area. While there, students mingled with the agency’s homeless clients and received general information about them and the services they receive at the agency. Then, 1 week after the training session, that agency hosted the AD Workshop.
Procedure/questionnaire
Before the training session, the 15 participants submitted their signed informed consent forms to W.N. After the training session, participants received a paper copy of the pre-Workshop questionnaire, which also included instructions that they were to submit their answers by email to W.N. any time before they attended the orientation to the agency that serves homeless persons. Participants were informed that they were free to respond at whatever length they wished to the items on the questionnaire. The pre-Workshop questionnaire included the following items: Is there anything about the prospect of meeting with a homeless person to help him or her with an AD that makes you apprehensive (e.g. nervous, afraid)? If so, please state, as specifically as possible, what it is that makes you apprehensive. If you do not feel apprehensive in any way, please articulate your thoughts and/or feelings about the prospect of meeting with a homeless person to help him or her with an AD. Is there anything about your participating in the AD Workshop that might be challenging for you? If so, please be specific in identifying the aspect(s) of the experience that might be challenging. Also, if possible, explain why you might find that/those aspect(s) of the experience challenging. (If you do not think you will find anything about the experience challenging, please ignore this question.)
At the Workshop, homeless persons who wished to complete an AD were screened for decision-making capacity. Next, each student met face-to-face with at least one homeless person, providing him or her with various levels of help to complete an AD (e.g. reading the form, serving as scribe, discussing EOL scenarios and examples of medical interventions). The authors were present and available during the Workshop to clarify aspects of the AD and to answer participants’ and homeless persons’ questions, as needed.
Immediately after the Workshop, the participants received an email that contained the post-Workshop questionnaire. They were asked to submit their answers by email to W.N. within 72 h. The questionnaire included the following items, which closely mirror those in the pre-Workshop questionnaire: During your participation in the AD Workshop, was there anything that made you apprehensive (e.g. nervous, afraid)? (If you had no such experiences, please skip to the next prompt.) If so, please state, as specifically as possible, what it was that made you apprehensive. Also, were you able to overcome your experience(s) of apprehension? If so, how? If not, what do you think might have helped you to overcome that/those experience(s) of apprehension? Was there anything about your participating in the AD Workshop that you found to be challenging (e.g. difficult, frustrating, complicated)? If so, please be specific in identifying the challenging aspect(s) of the experience and explain why they were challenging. Also, were you able to overcome that/those challenge(s)? If so, how? If not, what do you think might have helped you to overcome that/those challenge(s)?
After receiving responses from all 15 participants, W.N. paired each participant’s pre- and post-Workshop answers to illuminate similarities and differences, as discussed below.
Analysis
The participants’ responses to the pre- and post-Workshop questionnaires were analyzed using thematic content analysis, which involved examining the data for themes or patterns that might emerge across participants’ responses. 30 If such themes were discovered, the authors intended to represent the data in terms of those themes and to arrange them by time (i.e. as pre-Workshop and post-Workshop themes).
Each participant’s pre- and post-Workshop responses were paired, read multiple times by W.N., and analyzed in terms of both fears and challenges identified by that participant. This pairing technique proved helpful in that some participants sought to clarify or elaborate on their pre-Workshop responses as they answered post-Workshop questions. This first step of analysis was facilitated by each participant numbering each section of her text in relationship to the item on the questionnaire to which that section of her text responded. After each participant’s responses had been analyzed separately, those individual analyses were assembled and examined for similarities. Through that search for patterns across participants’ responses, three dominant themes emerged from the pre-Workshop responses. The same three themes were found in the post-Workshop responses, where they occurred less frequently.
Finally, the authors presented their findings in a participant debriefing session, during which participants confirmed the presence of the three themes and offered other insights into their experiences as participants. This way of applying the confirmability criterion (i.e. gaining assurance from the participants that the findings reflected their voices) strengthened the study’s trustworthiness. 30 During that debriefing session, the authors also disclosed to the participants that moral courage had been the experience and concept under investigation. That information was not revealed earlier because the authors wished to avoid the possibility that such knowledge would somehow bias participants’ responses to the questionnaires.
Results
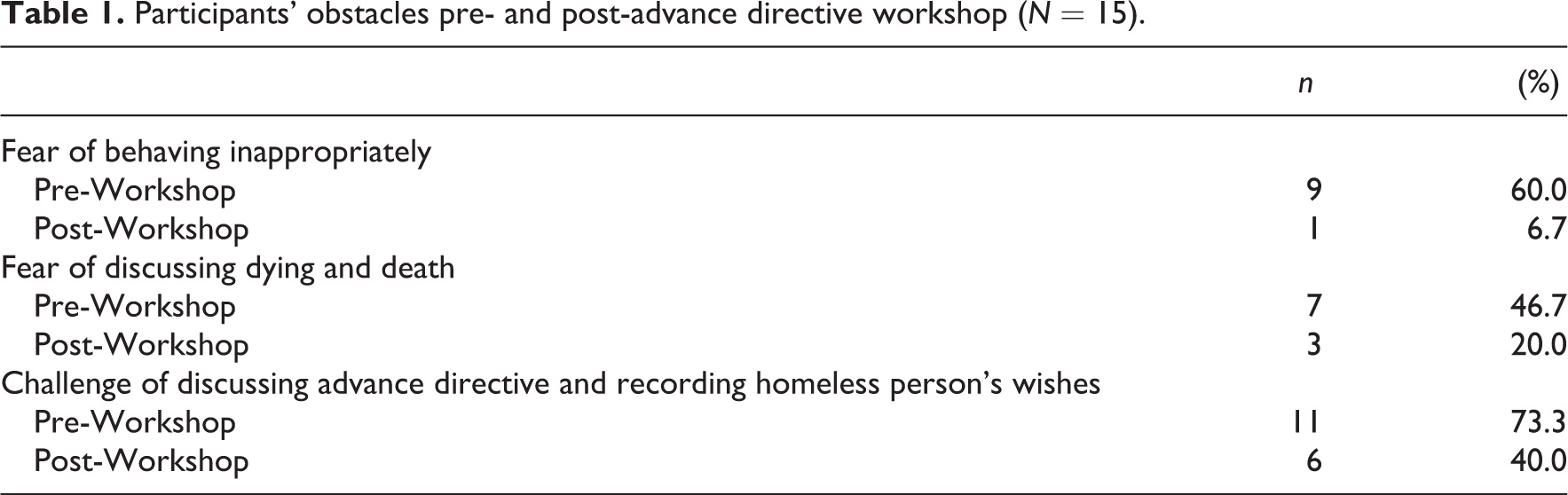
From the content analysis, three themes emerged, which can be categorized as two fears and a challenge. Prior to the AD Workshop, participants expressed fear that, during the Workshop, they would behave in ways that would be regarded as inappropriate by the homeless persons they would be assisting. Second, participants were afraid to broach the subject of a homeless person’s dying and death—a topic some participants characterized as “morbid” or “taboo.” Third, participants expected to be challenged by the tasks of adequately explaining the AD’s content, answering homeless persons’ questions related to that content, and accurately recording their wishes on the AD. However, each of these themes was found less frequently among participants’ post-Workshop responses (Table 1), indicating that, as a group, participants believed the Workshop would be more frightening and challenging than it turned out to be. In other words, while moral courage was required to participate in this project, participants required greater moral courage as they anticipated the Workshop (i.e. as they remained committed to providing the upcoming service) than during their actual experience of the Workshop. In relationship to each theme, participants suggested several intriguing explanations for the difference between their anticipation and actual experience of the Workshop.
Participants’ obstacles pre- and post-advance directive workshop (N = 15).
Fear of behaving in inappropriate ways
In their responses to the pre-Workshop questionnaire, 9 of 15 participants expressed apprehension about ways they might behave during the AD Workshop. They were especially fearful that the homeless persons might perceive their actions as judgmental or condescending. For example, one participant claimed to be “scared of saying something offensive. […] I don’t want to appear snooty or flashy, and I am afraid of being judgmental even if I don’t intend or want to be.” Similarly, another participant worried that she would fail to be “non-judgmental and patient” or would not be viewed “as an understanding and patient agent,” leading her to lose rapport with the homeless person.
In stark contrast, in their post-Workshop responses, only one participant recalled having experienced behavior-related fears during the Workshop. However, she was quick to make it clear that such fears did not persist: “I was able to overcome my experiences of apprehension after sitting with the neighbors for a little while and getting to know them.” Similarly, the participant who had worried prior to the Workshop that she might not be viewed as “understanding and patient” found that face-to-face interactions made the difference: “I think I was able to overcome these anxieties upon actually interacting with the [homeless woman]. She was very smart and independent, reading the form aloud to us both and writing her wishes herself.”
In addition to the role that face-to-face interactions played in reducing participants’ fears, four participants highlighted the value of the orientation they received to the agency that hosted the Workshop. One participant recalled that, after training, she had been “apprehensive about appearing judgmental or intimidating. However, after I attended orientation at the [agency], this apprehension seemed to dissipate.” Another participant remarked, “Touring the [agency], meeting some of the staff, and hearing the story behind the [agency] calmed my initial nerves.”
Fear of discussing a homeless person’s dying and death
In their pre-Workshop responses, 7 of 15 participants acknowledged a fear of speaking about the dying and death of the homeless persons they would be assisting. One participant commented, “Talking with a person about such morbid topics can also be challenging but I think that I will be fine as long as I build and [sic] adequate rapport with them from the beginning.” Perhaps the time allotted during training for participants to practice helping one another complete ADs played a role in preventing this fear from arising during the Workshop, for, in their post-Workshop responses, only 3 of the 15 noted that they experienced this fear during the Workshop. One of those who had been afraid before the Workshop explained that being able to “relate” to and “connect” with the homeless person helped her overcome her prior apprehensions: I was surprised at how easily the conversation flowed and how simple it was to listen and understand her story, and it turned out that I could relate to the person whom I was assigned to. She was a recently sober methadone addict, and having an addict in my family and knowing the experience allowed me to relate and understand what she was feeling when she was telling me how to fill out the “preserving dignity” pages and how she wanted to be remembered, as well as what she wanted her friends and family to know if something were to happen tomorrow. We were also able to connect on the basis of our faith, which is what she heavily relies on daily and uses Christianity as an example for her way of life.
It seems likely that the participants’ ability to establish such connections was strengthened by their having practiced conversing about ADs with one another during their training session, for each interviewer was encouraged to introduce herself and ask unobtrusive questions about the interviewee’s past (e.g. where she was born).
Challenge of explaining the AD’s content and recording the homeless persons’ wishes
In their pre-Workshop responses, 11 of 15 participants noted that they expected to find it challenging to explain the AD’s content clearly, offer adequate answers to homeless persons’ questions related to that content, and/or accurately capture homeless persons’ wishes on the AD. For example, one participant stated, I think the biggest challenge I will experience is having confidence in myself to properly explain and fill out the Advance Directive documents. I am worried that I will not have enough knowledge to further explain or give examples if the person needs them.
Similarly, another participant commented, I am most apprehensive about my ability to help the people who come to the [Workshop] complete the advanced directive correctly. I realize that this document has the potential to be signed and made permanent, leading to identifiable consequences. I fear that my ability, or lack of, to accurately describe in an educated and straightforward way all the options to the man or woman I am working with could lead them to make an ill-informed decision.
In their post-Workshop responses, 6 of the 11 participants who had anticipated this challenge reported that the Workshop had been very difficult in this respect, just as they had expected. Among these six participants, a common theme was the desire to have had examples of EOL interventions and their potential side effects at their disposal during the Workshop. One participant articulated that desire in this way: It was a little bit challenging finding the right ways to discuss such issues as end-of-life care. I wish I had been prepared with a few more examples of what some of the questions were asking […]. I think that some suggested stories would be helpful in filling out those parts [of the AD].
Another participant remarked, “The most challenging aspect of the [Workshop] was adequately explaining and giving examples for each question asked. […] I still struggled explaining the range of life sustaining treatments and their side effects in a concise way.”
In contrast with these responses, 9 of the 15 participants did not refer to these aspects of helping another person complete an AD as a serious challenge. Four participants shed light on a reason that, for them, this challenge was either mitigated or did not arise. The authors were present during the Workshop, these participants noted, and they could be called upon, if needed, to clarify portions of the AD or to answer questions related to its content. As a result, these participants experienced no serious obstacles in their conversations related to the AD’s content.
Discussion
As the first study to consider the place of moral courage at the intersection of nursing and ADs, we followed a qualitative descriptive design to investigate whether baccalaureate nursing students required moral courage to help homeless persons complete ADs. Prior to the Workshop during which they provided that assistance, participants reported that they expected to experience two fears and a challenge during the Workshop. However, after the Workshop, relatively few participants reported having encountered those obstacles. So, while moral courage was required to participate in this project, participants required greater moral courage as they anticipated the Workshop than during their actual experience of it. These findings might have important implications for how to improve the training nursing students receive before they provide this service.
Our findings indicate that, for the most part, the fears and challenge that participants experienced prior to the Workshop can be addressed easily. Most participants did not encounter those obstacles during the Workshop, and their post-Workshop responses often revealed why they did not encounter them or why those obstacles proved to be minor and manageable. That information was useful subsequent to this study, enabling the authors to improve the training of a new cohort of nursing students, preparing them to assist homeless persons at another AD Workshop.
First, participants’ responses shed light on the value of some aspects of the training they received—value that the authors did not always anticipate. For example, as discussed earlier, many participants noted that their orientation to the service agency prior to the AD Workshop reduced their fear of behaving in ways that homeless persons might regard as inappropriate. As a result, when the authors planned the training for a new cohort of nursing students, that orientation was retained as an essential step in the students’ preparation for the Workshop.
Similarly, it appears that participants’ opportunity to practice helping one another complete ADs during the training session eased their apprehensions about both behaving inappropriately and discussing a homeless person’s dying and death with him or her. Consequently, training for the new cohort of nursing students allotted much more time for the students to practice completing ADs. This was accomplished without lengthening their training session. The authors leveraged university resources to produce a quality training video. In the video, the two ethicists presented their PowerPoint and performed a role-playing interview. Nursing students in the new cohort received a digital copy of this video, enabling each of them to view the presentation and listen to the accompanying explanation at their leisure before attending the training session as a group. The video was also helpful in that students could use it to refresh their learning, reviewing portions of the presentation or the role-playing interview at any time prior to the AD Workshop.
The creation of another digital file helped members of the new cohort address the greatest challenge that the study’s participants encountered—the challenge of explaining the AD’s content and answering questions related to it. To address this challenge, the researchers proposed a recorded interview with an advanced practice nurse specializing in EOL care. One of the authors (the medical center ethicist) approached a colleague, a palliative care nurse, about being interviewed, and the nurse agreed. During the interview conducted by some of the honors students from the inaugural AD Workshop, the nurse discussed examples of EOL interventions (e.g. ventilator, feeding tube, hospice care, pain medications) and their potential side effects and other possible consequences (e.g. sores, infections, reduced mobility, limited communication). Students in the new cohort listened to the recorded interview prior to the next Workshop. Furthermore, notes from that interview were compiled and hard copies distributed to the students, which they kept accessible during the AD Workshop. All of these steps were designed to teach students more about EOL interventions and to inform and facilitate their discussions of the AD’s content with homeless persons. In the authors’ debriefing session with members of the new cohort, the students reported that these additional aspects of their training had been very helpful. In all of these ways, training for the project was improved to address the fears and challenge that the study participants encountered.
Conclusion
Given our study’s small sample size, its results cannot be generalized; however, portions of our approach might be transferable to similar settings or social contexts. For example, it seems likely that the fears and challenge that our study identified could be found among baccalaureate nursing students in any US state, for, in general, homeless persons are misunderstood and marginalized throughout the nation. Therefore, if nursing students are to be prepared adequately to provide this service, our training design, too, is likely to be useful across the United States.
Beyond these conjectures, additional research is needed at the intersection of nursing, moral courage, and ADs. Are our findings unique to US nursing students who seek to assist homeless persons, or might nursing students in other countries experience similar obstacles with respect to homeless persons or other marginalized groups in their nations (e.g. new immigrants and refugees, disabled persons, prisoners)? Furthermore, is it only nursing students who require moral courage, or do other caregivers—such as nurses, social workers, chaplains, or physicians with years of professional experience—also need moral courage to provide this service? Our study has sought to break new ground in this area of research, but much remains to be explored in the United States and internationally.
Lindh et al. 9 highlight the importance of developing pedagogical approaches that will cultivate courage—moral and otherwise—in nursing students “so that graduates will enter the profession with courage.” Because moral courage is necessary in nursing practice, 15 –17 our study provides valuable insight as to what the professional preparation of nursing students can include. Unfortunately, in nursing curricula, opportunities designed specifically for students to develop and practice moral courage appear to be rare. 18,19 Our study is an example of how moral courage might be cultivated in nursing students as part of a project through which they learn other important lessons. However, as our discussion makes clear, we would not advocate attempts to instill moral courage that expose students to avoidable fears or challenges (e.g. a fear of disrepute, the challenge of inadequate knowledge). Pedagogically, such an approach would be irresponsible. Instead, students should be prepared thoroughly and realistically to provide care, and the fears and challenges that could accompany their caregiving should be reduced as much as possible. For example, we minimized the students’ fear of disrepute by having them conduct the Workshop as a group (i.e. with a sense of mutual support)—avoiding the intimidation of meeting one-on-one with homeless persons at separate times—and by praising them for providing this service. So, after minimizing foreseeable fears and challenges in such ways, numerous opportunities for students to exercise moral courage could be offered in a course or curriculum, for some aspects of ordinary nursing practice—the complexity of caring for someone who is vastly different from oneself, for example—seem intractable and daunting enough.
Footnotes
Acknowledgements
The authors gratefully acknowledge the persons experiencing homelessness who allowed our nursing students to participate in their meaningful decision-making. The authors also express their appreciation to the staff members of the Volunteer Ministry Center for their hospitality and assistance. Finally, the authors wish to thank Vicki Cannington, APN, of University Palliative Care at the University of Tennessee Medical Center for generously lending her expertise to this project.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.