
Abstract
Background:
Nurses engaging in research are held to research ethics standards.
Research aim:
Examine experiences, behaviors, and perceptions of nurses in Israel regarding research ethics and explore possible related factors.
Research design:
An original investigator-designed self-administered questionnaire measured five variables: (a) ethics in research, (b) encountered research misconduct during the course of one’s studies, (c) the inclination to fabricate data, (d) the inclination to select or omit data, and (e) knowledge of research misconduct in the workplace. Additionally, demographic data were collected.
Participants and research context:
The questionnaire was completed by 151 Israeli registered nurses. 10.2% hold a PhD, 34 % hold an MA, 42.2% hold a BA, and 13.6% with no academic degree.
Ethical considerations:
The study was approved by the University’s ethics committee; anonymity and consent of the respondents were respected.
Findings:
Registered nurses’ level of studies achieved was significantly associated with a lower inclination to fabricate data, with one exception—PhD nurses were more inclined to fabricate data than nurses with a Master’s degree. A trend was found in which a higher level of studies is associated with higher knowledge of research misconduct in the workplace.
Discussion:
Results indicate that nurses’ perceptions of research ethics change throughout their academic studies, indicating a positive influence of level of studies, research experience, and work experience on ethics perceptions. Nevertheless, PhD nurses showed a greater inclination to actually select, omit, or even fabricate data than MA nurses. This may be related to pressure to publish.
Conclusion:
PhD nursing programs should include ethics training. Academic faculty members should serve as role models regarding research integrity. Research ethics deserves further emphasis on all levels of nurse education in Israel, as well as in the nurses’ code of ethics and related documents. This may positively impact ethical research practices.
Keywords
Introduction
Integrity and compliance with ethical standards are crucial and essential for the purpose of advancing knowledge and conducting high-level scientific and academic research. Research misconduct may cause harm in various ways: from a scientific point of view, it reflects on the reliability of the results, the professionalism of the researchers, future research, and the public perception of academic work and academia; 1 –3 from a clinical point of view, it may result in physical and emotional harm to research participants and future patients.
As nurses have a significant role in biomedical research, this study focuses on factors that may influence nursing research ethics conduct.
The aim of this study is to examine behaviors, experiences, and perceptions of nurses in Israel regarding research ethics and to explore possible demographic factors that may be associated with them.
The study explores to what extent nurses encounter research misconduct during their studies; their knowledge of research misconduct in the workplace; what behaviors nurses deem improper in the various phases of research; and finally, the extent to which nurses are inclined to fabricate, select, or omit data in research.
Based on the results of a questionnaire designed by the authors for this study, we explore possible reasons for differences in research ethics approaches and behaviors between nurses who achieved different levels of academic studies and consider various suggestions to possibly improve nursing research ethics: developing nursing research ethics guidelines by the nurses’ association, integrating research ethics training to PhD nursing programs, and having academic staff serving as role models for upholding research ethics practices.
Background
Sar 4 views a research study as the fruit of a researcher’s creative thinking, the product of hard work, talent, personal investment, and the ability to articulate an idea. As such, it should enjoy the legal protection from being plagiarized; thus, the invention or falsification of passages from it or its replication without acknowledgement of the original is deemed dishonesty and academic fraud, and punishable by severe penalties.
Scholars trying to explain the reasons for research misconduct related to pressures to publish for the purpose of academic promotion; an unsupportive research environment; as well as other structural, sociological, and psychological factors; 2 personality traits; 5 encountering academic misconduct during one’s academic studies or in other settings; 6 and academic level. 6 –8 Moreover, Fanelli et al. 2 concluded that scientific misconduct is more likely to occur in countries that lack research integrity policies, countries where individual publication performance is rewarded with cash, cultures, and situations where mutual criticism is deficient, and in the initial phases of a researcher’s career.
Research in healthcare and nursing aims to construct new knowledge, advance clinical practice, and protect the reliability of the research process that may relate to life, health, and the well-being of individuals and society as a whole. Research integrity seems crucial as ethical conflicts involving issues such as resource allocation, funding, budgeting, and economic expansion may arise. Nurses’ skill set may be very useful assuming leadership roles in ethical conflicts and decision-making in research ethics–related matters they handle. 9
The role of ethical codes is debatable. Pattison 10 wondered whether nursing codes of practice are likely to foster and elicit ethical awareness and behavior, particularly if they utilize ambiguous or confusing terminology or lack ethical guidance. The same critical approach to nursing codes of ethics may be specifically applied to research ethics in these codes: global nurses’ codes of ethics and professional behavior refer to research to varying degrees. Research is described in these codes as one of the nursing domains and therefore, it should meet ethical standards. 11 –13
Some nurses’ associations have published specific research ethics guidelines in addition to the general code of ethics. 14,15 The American Nurses Association (ANA) Code of Ethics, along with its interpretive statements, relates to research both directly and indirectly. It defines “practice” as including research and it relates to the role of researcher as one of the nurses’ various roles; it mentions the possibility of nurses facing conflicting loyalties and conflicts of interest in the field of research; it relates to the interdependence of nurses on other professionals in research work, as well as to the accountability and responsibility of nurses for the quality of the research they are involved with; and, of course, it relates to the protection of participants in (clinical) research. Finally, it mentions additional ANA position statements that address research issues, although we found no specific ANA position statement focusing on this issue. 16
In comparison, the Israeli Nurses Association Code of Ethics relates to the nurse’s duty to maintain a high standard of professional conduct and states that “Research shall be conducted in accordance with customary ethical rules.” 17 This statement is subjected to different interpretations. Moreover, one may wonder what these customary ethical rules are, at which point they are presented to nurses conducting research, and to what extent, if at all, this ethical duty is emphasized as part of the nursing ethics education. While research ethics guidelines could be general and aimed at various professionals involved in research, it might be advisable that the nurses’ association develop specific nursing research ethics guidelines. This could emphasize the importance allocated to research integrity and the role of the nurses in maintaining it.
Ethics education may be manifested not only in the ethics curriculum but also in other practices of the academic institution, including how academic honesty is managed. The International Committee of Medical Journal Editors (ICMJE) states that an author will be deemed to be the person who conceived the topic of the research/paper, and/or analyzed the data, and/or wrote, or made substantial alterations to, the final report, and/or gave final approval for publication of the research/paper after having verified that it satisfied all accepted standards, and proofed and edited it.
18
In recent years, the number of students registered in academic nursing programs in Israel (as opposed to non-academic programs which were common in the past) has significantly increased. 19 Undergraduate academic training programs in nursing focus on basic level of research (courses on research methods and statistics), whereas programs for higher degrees contain a more advanced level of research training. Another factor that may indicate the emergence of a pro-research nursing approach is the establishment of the Israeli Society for Nursing Research in 2002. These developments in Israel call for a need to examine the amount of attention that research ethics currently receive among nurses.
Methods
Study procedure
An original investigator-designed questionnaire was compiled by the research team for this survey based on the literature. 4,6,20 –22
In this cross-sectional, descriptive, correlational study, a convenience sample of 151 Israeli registered nurses from a broad range of fields, including community nurses, intensive care unit (ICU) nurses, and nurse researchers responded to the questionnaire.
In the first phase, the questionnaire was distributed among nurses enrolled in academic and other training programs at the Tel Aviv University’s Nursing Department. At the beginning of a class, in the first semester of studies, nurses were addressed by one of the researchers and asked to participate in a study on ethics in scientific publications. The researcher explained the study’s aim is to learn about nurses’ positions on scientific publication ethics and the manner in which the information would be used. The researcher also explained that their participation in the study was entirely voluntary and that they could stop at any point. The nurses were guaranteed that non-participation would not cause them any harm and that all information would remain confidential. A total of 148 printed questionnaires were distributed among nurses starting a BA, MA, or PhD program in Tel Aviv university; of which, 119 responded. In order to reach more nurses with higher level of studies achieved, the second phase included posting an online link to the questionnaire in the closed Facebook group of the Israeli society for nursing research. In total, 32 users (18 of them holding an MA and 8 holding a PhD) entered the online questionnaire and fully responded to it. The overall compliance rate was 84%.
Ethical considerations
The study was approved by the Tel Aviv University ethics committee. To respect the privacy and anonymity of the participants, the demographic information only related to gender, age, country of birth, education, and professional role—in general. It did not relate to the specific field of nursing, specific name of the hospital/institute they work at, or to personal information such as name or ID. The filled in questionnaire are kept in a locked closet with access of the authors only. Participants approved that by filling in the questionnaire, they consent to participate in the study and that they may choose to not participate at any given moment. The submission of the filled questionnaires was done in a manner that preserves the anonymity of the participants and allows them to avoid submitting it altogether.
Tools
Questionnaire development
The instrument consisted of a cross-sectional, descriptive, correlational study questionnaire developed by the authors, two of whom are experts in medical ethics and two in nursing research. First, the authors discussed and agreed upon the sections/variables of the questionnaire, based on themes discussed in the literature. Then, each author composed suggested questionnaire items for each of the sections. Finally, all four had to be in full agreement for any item to be included in the questionnaire. A pilot study was conducted on 10 nurses to evaluate respondents’ understanding of the questionnaire, its wording, items, comprehensiveness, and structure.
Research tool description
The structured self-administered questionnaire measured five variables: (a) ethics in research, (b) encountered research misconduct during the course of one’s academic studies, (c) the inclination to fabricate data, (d) the inclination to select or omit data, and (e) knowledge of research misconduct in the workplace. In addition, respondents’ demographic data were also collected.
The variable of ethics in research was measured by a 25-item tool measuring the respondent’s agreement with various items related to ethics in research. The tool consisted of statements such as “It is acceptable for articles to contain excerpts from other works without citation,” “It is acceptable to report data in a way that fits the hypothesis of the researcher,” and “An article with inaccurately presented results is considered misconduct and fraud.” Respondents were asked to rank the extent of their agreement with the statements on a scale of 1 (completely disagree) to 5 (completely agree). Relevant items were reverse scored. In this study, Cronbach’s alpha of the questionnaire was 0.71.
The variable of encountered research misconduct during the course of one’s academic studies was measured by a 4-item tool measuring the experience of ethical misconduct during academic studies, a modified version of Nilstun et al., 23 which contained questions about dishonesty and other unethical behavior in connection with research and with academic studies. The tool consisted of statements such as “During your academic studies did you encounter…(a) data misrepresentation to improve an exam score, (b) changing academic research findings in order to improve outcomes, (c) a reporting of findings or results despite knowing that they are not true, (d) incidents of plagiarism.” Respondents were asked to rank the degree of their agreement with the statements on a scale of 1 (never) to 5 (many times). In this study, Cronbach’s alpha of the questionnaire was 0.78.
The variables of (1) inclination to fabricate data and (2) inclination to select or omit data were measured by a 4-item tool. Questions related to the respondents’ inclination to (1) speed up the publication of research results, (2) increase the chances of a trip abroad at the expense of the employer, (3) increase chances of being appointed to a senior position, and (4) increase the chances of receiving a scholarship. Respondents were asked to provide a yes/no response. If respondents gave at least one positive response to any of the questions, the answer was coded as “inclination of the respondent to fabricate data” or “inclination of the respondent to select or omit data,” respectively.
The variable of knowledge of research misconduct in the workplace was measured by a 2-item tool with four different scenarios (a total of 8 items) measuring the encounters of respondents with ethical misconduct in the workplace: 1. In your view, did the following occur in your workplace:…(a) adjusting research results, (b) adjusting research data, (c) unfair order of names in the list of authors, (d) publication of a study in several journals (double publishing). 2. In the last 12 months, did you encounter unethical professional pressure related to…(a) the order of the authors’ names in an article, (b) data collection, (c) research results, (d) adding to the list of authors the name of a person who had no actual part in the research.
Data analysis
Descriptive statistics were used to analyze the respondents’ sociodemographic data and to describe the research variables. To examine the differences between multiple groups, a one-way analysis of variance (ANOVA) for variables with normal distribution, or chi-square for dichotomous variables, was performed. T-tests for independent variables were conducted to examine the differences between independent groups. Data were analyzed using SPSS v21.0 (IBM, USA).
Demographic and clinical characteristics of participants
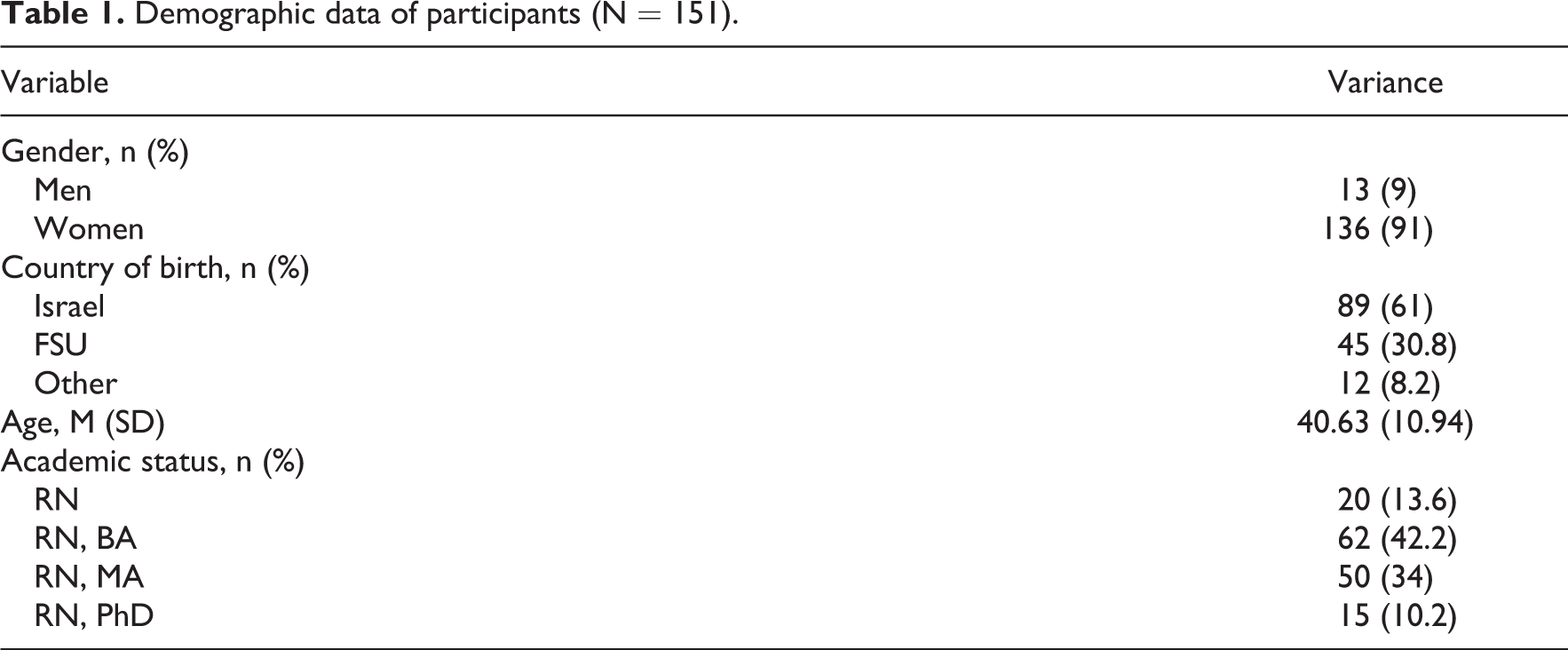
All 151 respondents were nurses, 23–70 years of age (mean = 40.73, standard deviation (SD) = 10.98), and the majority (91%) were women. Of which, 61% of the respondents were born in Israel and 30.8% were born in the former Soviet Union (FSU); 44% had a Master’s or PhD degree (see Table 1).
Demographic data of participants (N = 151).
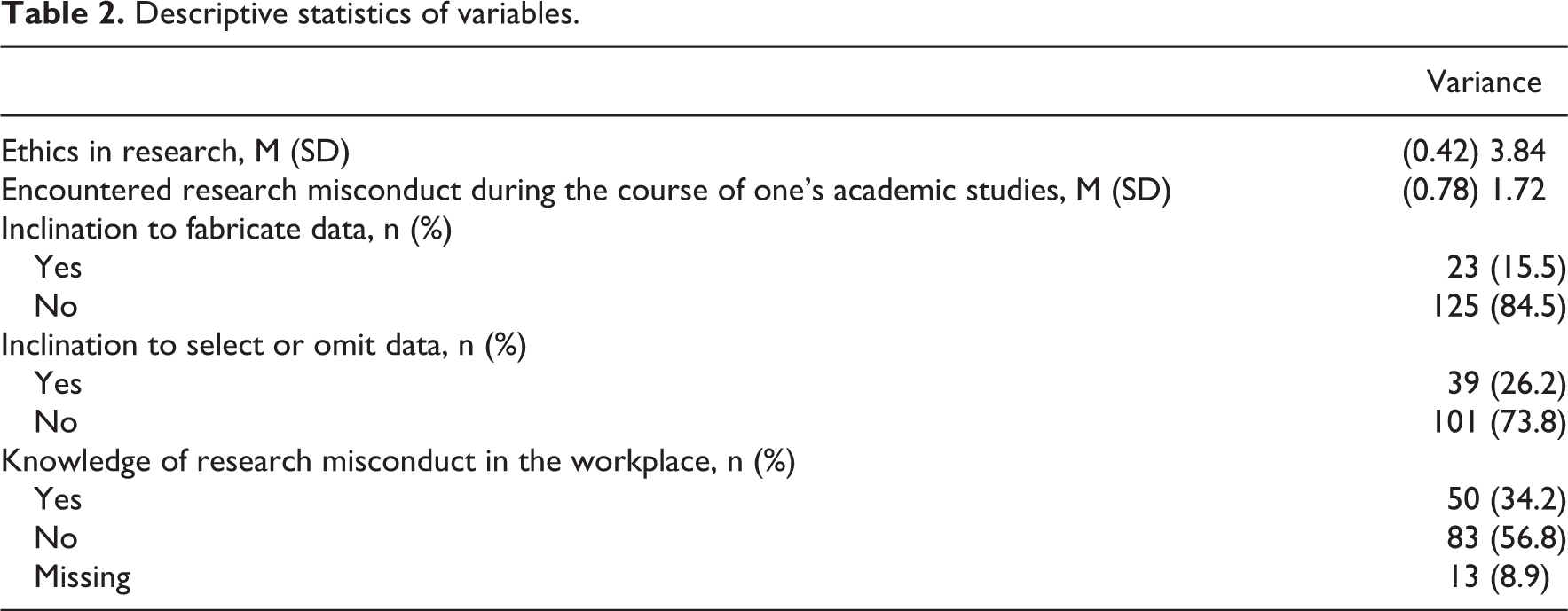
As presented in Table 2, 26.2% (39) of participants showed an “inclination to select or omit data.” Moreover, 15.5% (23) showed an “inclination to fabricate data.” One-third of the study sample (34.2% (50)) reported knowledge of research misconduct in the workplace.
Descriptive statistics of variables.
A one-way ANOVA was conducted to examine respondents’ attitudes toward ethics in research with different levels of studies achieved (four levels: RN, BA, MA, and PhD). A significant difference was found between different levels of studies achieved (F(3, 145) = 12.537, p < 0.01). The scores were as follows: “RN” (M = 3.61, SD = 0.33); “BA” (M = 3.70, SD = 0.38); “MA” (M = 3.94, SD = 0.40); and “PhD” (M = 4.27, SD = 0.25) (see Table 3).
One-way ANOVA for multiple group differences.
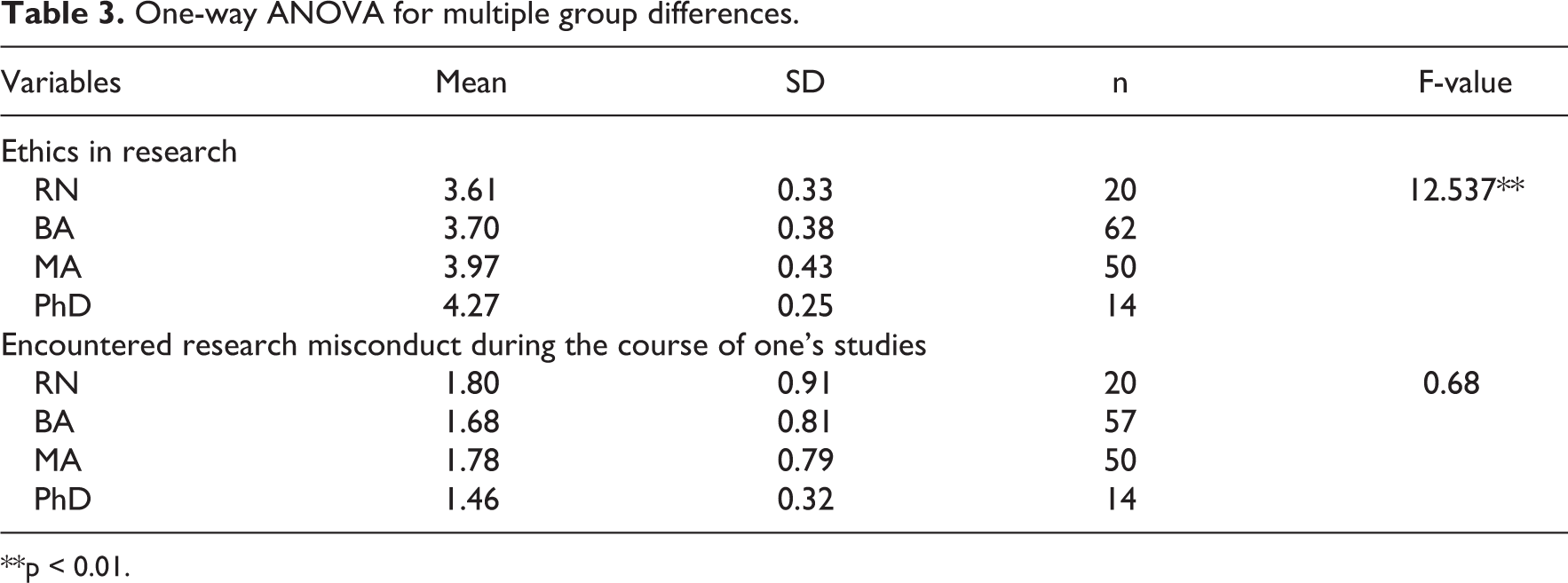
**p < 0.01.
A one-way ANOVA was conducted to examine the encountered research misconduct during the course of one’s academic studies (four levels: RN, BA, MA, and PhD). No significant differences were found (see Table 3).
Independent t-tests were conducted to examine the differences between nurses who reported an inclination to fabricate data, and nurses who did not, in their attitudes toward ethics in research and, separately, in their encountered research misconduct during the course of their academic studies. A significant difference was found between the two groups only in attitudes toward ethics in research (t(145) = 3.20, p < 0.01). Nurses who did not report being inclined to fabricate data achieved a higher score (M = 3.88, SD = 0.42) on ethics in research than nurses who reported such an inclination (M = 3.57, SD = 0.41) (see Table 4).
T-test for group differences regarding attitudes toward ethics in research and regarding encountered research misconduct during the course of one’s academic studies.
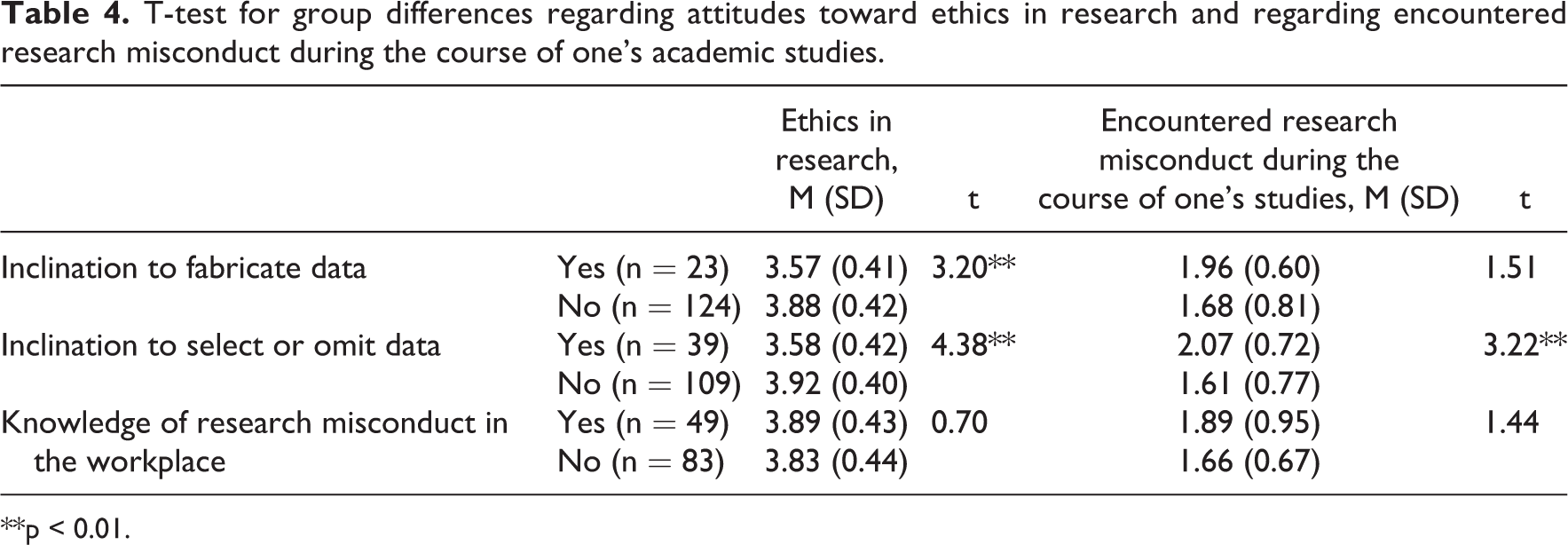
**p < 0.01.
Independent t-tests were conducted to examine the differences between nurses who reported an inclination to select or omit data and nurses who did not in their attitudes toward ethics in research, and separately in their encountered research misconduct during the course of their academic studies. A significant difference was found between the two groups in their attitudes toward ethics in research (t(146) = 4.38, p < 0.01) and in their encountered research misconduct during the course of their academic studies (t(146) = 3.22, p < 0.01). Nurses who did not report an inclination to select or omit data achieved a higher score (M = 3.92, SD = 0.40) on ethics in research than nurses who reported such an inclination (M = 3.58, SD = 0.42). In contrast, nurses who did not report an inclination to select or omit data had a lower score (M = 1.61, SD = 0.77) on encountered research misconduct during the course of their academic studies than nurses who reported such an inclination (M = 2.07, SD = 0.72) (see Table 4).
Independent t-tests were conducted to examine differences between nurses who reported knowledge of research misconduct in the workplace and nurses who did not, in their attitudes toward ethics in research and, separately in their encountered research misconduct during the course of their academic studies. No significant differences were found (see Table 4).
Chi-square tests were conducted to examine the associations between level of studies achieved (RN, BA, MA, and PhD) and “inclination to fabricate data,” and between “inclination to select or omit data” and “knowledge of research misconduct in the workplace,” respectively. Of all nurses who reported an “inclination to fabricate data,” 35% were RNs, 14.8% had a Bachelor’s degree, 6.1% had a Master’s degree, and 13.3% had a PhD. In contrast, of all nurses who did not report an “inclination to fabricate data,” 65% were RNs, 85.2% had a Bachelor’s degree, 93.9% had a Master’s degree, and 85.8% had a PhD. The correlation was significant (
Chi-square tests.
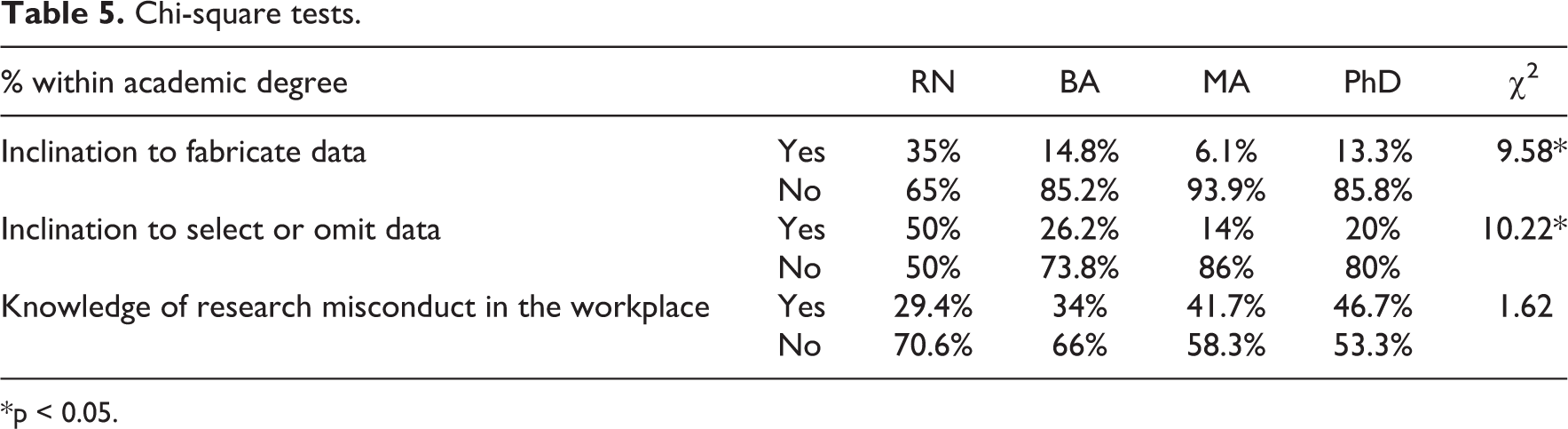
*p < 0.05.
Of all nurses who reported an inclination to select or omit data, 50% were RNs, 26.2% had a Bachelor’s degree, 14% had a Master’s degree, and 20% had a PhD. In contrast, of all nurses who did not report an “inclination to select or omit data,” 50% were RNs, 73.8% had a Bachelor’s degree, 86% had a Master’s degree, and 80% had a PhD. The correlation was significant (
As for nurses who reported knowledge of research misconduct in the workplace, the following 29.4% were RNs, 34% had a Bachelor’s degree, 41.7% had a Master’s degree, and 46.7% had a PhD. In contrast, of all nurses who did not report knowledge of research misconduct in the workplace, 70.6% were RNs, 66% had a Bachelor’s degree, 58.3% had a Master’s degree, and 53.3% had a PhD. The correlation did not reach statistical significance. Nevertheless, one can encounter a trend in which a more advanced academic degree is associated with higher knowledge of research misconduct in the workplace.
Discussion
Nursing research has become increasingly prevalent in Israel, as it has worldwide. This requires an emphasis on research ethics, integrity, and avoiding misconduct in research. This study examined nurses’ perceptions regarding research ethics, their encounters, and knowledge of research misconduct during their professional studies and at work, and their inclination to fabricate, select, or omit data in research. The results indicate that nurses’ perceptions of research ethics change throughout their academic studies. Nurses with a PhD have the highest ethics perceptions in comparison with nurses with lower academic degrees. PhD nurses scored higher than all the other groups of nurses for overall ethics perception. This may indicate the positive influence of academic studies, research experience, and work experience on ethics perception.
At the same time, PhD nurses showed a greater inclination to actually select, omit, or even fabricate data than MA nurses. This may be related to pressure to publish, which is more prevalent among PhD holders, as suggested by Fanelli et al. 2 In Israel, as worldwide, PhD students are expected to publish papers resulting from their dissertation. The growing risk of research misconduct as the PhD population increases was highlighted by Mitchell and Carroll, 8 who recommend setting guidelines for students and supervisors who conduct research under pressure and deadlines within a undefined or unclear ethical work environment.
Moreover, in our study, nurses who were inclined to fabricate, select, or omit data achieved a lower score on their perception of ethics in research. Interestingly, nurses who were inclined to select or omit data had significantly more encountered research misconduct during the course of their studies. At the same time, nurses who were inclined to fabricate data did not differ in their level of encountered research misconduct during the course of their studies. This finding supports the suggestion of Stone et al. 24 to differentiate between minor and serious academic integrity violations. Although in their paper they do not refer to data omission, we would suggest that selecting or omitting data should be perceived by researchers as minor in comparison with fabricating data. Thus, the first could be influenced by encountered research misconduct during the course of one’s studies while the second was probably not.
The association between encountered data misrepresentation during the course of studies and future inclination to engage in such activities should also focus on academic faculty members and their ethical behavior. Academic faculty members should understand that they serve as role models for their students, who learn from and are influenced by their teachers’ behavior, morals, and norms. According to Confucian philosophy, rulers should lead by example, and not rely on the rule of law alone. 25 Honesty seems to be an important academic virtue. Academics, who make sure they are not selecting data, omitting data, or fabricating it, should have a strong impact on their students, more than mere knowledge of the ethical guidelines (or “rules”) on the part of the students. This notion is also reflected by Kornfeld’s 26 argument that specialized ethical courses have not reduced the level of ethical misconduct, and who therefore suggests using a mentor system in which the mentors share responsibility for their trainees’ work. In addition to “leading by example,” it would seem advisable to actually teach the skills of original academic composition to students, as suggested by Pennington, 6 who also states that this cannot be other than a lengthy process and so must begin at an early stage.
Additionally, we found that higher level of studies achieved was significantly associated with a lower inclination to fabricate data, with one exception—PhD nurses were more inclined to fabricate data than nurses with a Master’s degree. Finally, higher level of studies achieved significantly associated with a lower inclination to select or omit data, with one exception—PhD nurses were more inclined to select or omit data than nurses with a Master’s degree.
Currently, PhD-level nursing programs in Israel do not contain an ethics course or training on ethics in research. Nevertheless, PhD students are expected to uphold ethical standards and norms regarding research and scientific publication. Clayton et al. 27 suggest using simulation techniques to enhance the ethical training of PhD students. They view simulations as a way of practicing and reinforcing the principles of responsible conduct of research in a safe and controlled environment. Djalalinia et al. 28 recommend using misconduct management programs in research education, particularly for health researchers, as ethical training improves research designing, conducting, and results publication.
Limitations
A possible limitation of the study relates to the subject matter, as it requires respondents to self-report on actual or possible wrongdoings on their part. As such, the results may be somewhat biased and the conclusions should be taken under careful consideration. Furthermore, the study was conducted in Israel and thus conclusions may not necessarily reflect on different nurses’ populations.
Future research could focus on a large international sample of nurses and widen the tools used for the collection of further data (i.e. using simulations and discussing disciplinary case reports) and may allow for comparing different nurses’ population perceptions regarding research ethics.
Conclusion
In light of our findings, we suggest constructing training programs in research ethics, as a part of the PhD-level nursing programs in Israel that will include both reference to research misconduct guidelines and simulations.
As nursing research becomes more prevalent in Israel, the issue of ethics in nursing research deserves more attention. Following our study, we conclude that deepening the ethics perception of nurses is warranted. We suggest constructing a specialized training program on ethics in research according to the level of the studies. This will impress upon faculty members and supervisors of students at all levels of research the importance of giving a personal example in research ethics. We also suggest that the Israeli Nurses Association Ethics Bureau consider adopting specific guidelines or annotations for research ethics in nursing that would be referred to in its ethics code, which currently only mentions “customary ethical rules.”
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.