
Abstract
Background:
In recent years, the interest in ethical climate has increased in the literature. However, there is limited understanding of the phenomenon within the cancer care context as well as between countries.
Aim:
To evaluate cancer nurses’ perceptions of hospital ethical climate in Greece and Cyprus.
Research design:
This was a quantitative descriptive–correlational comparative study with cancer nurses. Data were collected with the Greek version of the Hospital Ethical Climate Survey questionnaire in addition to demographic data.
Participants and research context:
In total, n = 235 cancer nurses working in cancer care settings in Greece and Cyprus were recruited at two national oncology nursing conferences.
Ethical considerations:
The study conforms to the principles of the World Medical Association Declaration of Helsinki and the relevant ethical approvals were obtained according to national law.
Results:
The results showed that in terms of the “Managers” dimension, participants working in Greek hospitals (4.30 ± 0.73) had a higher score compared to the Cyprus participants (3.66 ± 0.93) (t = −5.777, p ≤ 0.001). The perceptions of nurses working in oncology units in Greece regarding the ethical climate were more positive compared to Cyprus (M = 3.67 for Greece and M = 3.53 for Cyprus, p ≤ 0.001). Nurses with a higher level of education had a lower average ethical climate score across all dimensions. All dimensions exhibit positive and moderate to high correlations between them (r = 0.414–0.728, p < 0.01).
Conclusion:
It is imperative to evaluate and improve the hospital ethical climate that prevails in each cancer care department. This highlights the fact that nurses working in seemingly similar cultural and organizational contexts might still have different perceptions of the ethical climate. Despite these differences, it is necessary to create the right conditions to address ethical issues. A positive ethical climate requires good relationships between healthcare professionals and the presence of good teamwork in order to ensure better healthcare provision.
Introduction
Nursing has grown extensively in recent years. Today’s nurses have the knowledge, academic background, as well as the responsibility to make decisions or facilitate the patient’s decision-making process on complex issues related to care within a multidisciplinary context. In each of these cases, the goal is to ensure the best possible outcomes when it comes to the patients’ health by providing the highest quality of care that meets the patient needs and preferences. In this context, nurses face various moral dilemmas when there are two or more conflicting views. 1
According to the American Nurses Association, 2 a healthy working environment is one that is safe, empowering, and satisfying. The World Health Organization reports that the working environment is a place of “physical, mental and social well-being,” where all healthcare professionals aim at both the health and safety of their patients and colleagues. Within this context, it is important for the environment to cultivate a sense of security, respect, and empowerment for all members of the multidisciplinary team. These are basic principles that constitute the ethical climate which is part of the working environment. The prevailing climate in any workplace can negatively or positively affect the work of the healthcare professionals. Therefore, it is important to understand healthcare professionals’ perceptions on their workplace’s ethical climate for achieving and maintaining the quality of the care provided and for promoting their well-being. Within this workplace context, nurses are routinely challenged to reconcile the dichotomy between professional ethical practice set forth by the International Council of Nurses (2012) and organizational constraints which often hinder the nurses’ ability to address the myriad of challenging dilemmas in the workplace. 3 Preceding studies have demonstrated that nurses’ work environment is associated with the provision of individualized and quality care, missed nursing care, and lower mortality rates.
Nurses working in hospital wards are routinely called upon to cope with various stressors. In an already stressful environment, nurses are also confronted with various ethical issues related to patient care. These issues become more complex and difficult when nurses take care of patients affected by cancer. In this context, nursing professionals face situations of pain, finitude, and death; physical and emotional side effects such as hopelessness, fear, and loneliness; intense and denouncing feelings of human fragility, at the same time that an expectation of curing the disease may be present. 4,5 Further ethical challenges can be derived from situations such as the decision to interrupt treatment, the extension of life without concern for its quality, or caring for young people with a poor prognosis. 6,7
These difficult situations, related to the care provided by healthcare professionals in cancer care departments, call for a thorough study of ethical climate. Caring for people affected by cancer is a complex and demanding task that can have a burdensome strain on healthcare professionals. The manifestation of a positive ethical climate in the organization is considered as a pivotal, since it has been associated with the nurses’ job satisfaction in their workplace, 8,9 moral distress, 10 –13 well-being in general, 11 and quality of care provision. 14
There are many terms used to describe the ethical climate, such as the “ethical dimension,” “moral climate,” “ethical culture,” and “ethical environment.” 15 The interest in the ethical climate has risen in the literature in recent years, and thus interest in it has soared. A few studies have explored the hospital ethical climate in relation to nurses for the older people, general nurses, and psychiatric nurses but very few are available in relation to cancer care nurses. For example, a study in Sweden investigated to what extent nurses who care for children with cancer managed to deal with difficult decisions related to death, life, and pain depending on the ethical climate that prevailed in their workplace. Vryonides et al. 16 conducted a study on the associations between the ethical climate and missed nursing care in cancer care units. Overall, the topic of the ethical climate has not been extensively studied within the cancer care context and explicitly in relation to the evaluation of perceptions of oncology nurses regarding the ethical climate. There appears to be a gap in the literature in relation to cross-country comparisons of nurses’ perceptions on the ethical climate. 16
Ethical climate
The concept of ethical climate was first introduced by Victor and Cullen and entails the common perceptions of what is morally correct and how ethical issues are resolved in an organization. 17 Olson 15 defined ethical climate as “the individual perceptions of the organization that influence attitudes and behavior and serves as a reference for employee behavior.” It is “the one in which organizational practices and conditions promote discussion and resolution of decisions with ethical content.” Others defined the ethical climate as the normal behavior and action of workers within the workplace, as well as the support offered to them by their organization. 18 The ethical climate of an organization is not a constant variable but a changeable one, especially in a hospital setting. The climate can vary between groups of nurses, in different environments, and in different working conditions. 17
Several factors have been found to be associated with the ethical climate including self-interest, company profit, efficiency, friendship, team interest, social responsibility, personal morality, rules, company procedures, laws, and professional codes. 17,19
In the nursing literature, the value and importance of creating a positive ethical climate in the hospital has been systematically emphasized. A positive ethical climate can be related to an organization fostering caring and well-being of others, promoting supportive hospital management, fostering shared responsibility and teamwork with commitment to ethical behavior through inter-professional cooperation and adequate communication. Preceding studies showed that the positive ethical climate facilitated the ability of the healthcare professionals to meet the needs of patients and relatives. 1 Furthermore, a positive ethical climate promoted the exchange of information between healthcare professionals and the existence of an ethical code of conduct in the workplace. 6
A less positive ethical climate among healthcare professionals in the cancer care setting can be the result of frustration feelings that prevail among nurses, job dissatisfaction, poor business relations, and disputes that may arise during working hours. Studies showed that the ethical climate affects not only the ambitions but also the behavior of workers. The consequences of a less positive ethical climate can include nurses’ burnout, a lack of interest in the job, and a reduction in the quality of care provided. 10,12 The prevailing climate in any cancer care setting between staff mirrors the quality of care received by patients. Since the ethical climate can affect nurses adversely, there is need to create a climate in which they can feel secure and can effectively resolve ethical challenges.
Literature
In a study by Siebens et al. 20 using the BELIMAGE assessment tool, researchers rated the “way the nurses perceive themselves within their working environment.” This study concluded that the feeling of dissatisfaction and burnout reported by nurses was related to the environment in which they worked rather than the clinical practice as such. In another study by Abou Hashish, 21 whose purpose was to determine the relationship between the ethical climate in the workplace and the organizational support and satisfaction of nurses within their work environment, five measuring tools were used (an ethical climate questionnaire, a survey of perceived organizational support, an organizational commitment questionnaire, an index of job satisfaction, and a turnover intention scale). This study showed that there is a correlation between organizational support and the job satisfaction of nurses and therefore their perceptions about the ethical climate in their workplace.
In contrast, a study with 235 general nurses working in four public hospitals and three private ones in Iran explored nurses’ perception on the ethical climate through the use of the Hospital Ethical Climate Survey (HECS) questionnaire. The results showed a high score on the “Physicians” dimension in nurses. Furthermore, the results showed no statistically significant difference between the perceptions of nurses regarding the ethical climate depending on where they worked, either in the private or the public hospitals.
A study by Bartholdson and Lutzen 6 studied the experiences of nurses caring for children with cancer and the way these experiences related to ethical issues. The study showed that healthcare professionals appraised the contribution of teamwork when dealing with ethical issues in this context. Therefore, the case of relationships between the healthcare professionals becomes important when retrieving their perceptions on ethical climate.
Goldman and Tabak, 9 who studied the perceptions of nurses on ethical climate and any associations to demographic data, showed that gender, job tenure, and the level of education level can affect the nurses’ perceptions of the ethical climate. Relationships between members of a group seem to be a prerequisite so that all members are satisfied with their work. The teamwork and cohesion of a group can be categorized as a predictor of whether members are satisfied. Goldman and Tabak 9 also pointed out that the managers are the ones who should set an example and be emulated by the team members in order to promote a positive ethical climate among members.
Hwang and Park 22 studied the perceptions of 1826 nurses in public hospitals in Korea with the HECS questionnaire. Their study indicated a low score in the dimension “Physicians.” Nurses who exhibited a more positive climate in the dimension “Patients” tended to make fewer medical errors, while nurses who exhibited a positive ethical climate in the dimensions “Manager,” “Hospital,” and “Physicians” seemed to be less willing to leave their jobs. In terms of the demographic data, the results showed that the working experience was positively associated with the perceptions that nurses have of the ethical climate in their workplace.
Importance
The study of the hospital ethical climate and its relationship with demographic data are extremely significant for the organization and clinical practice. It is important to know whether the ethical climate that prevails among health professionals is positive or less positive. A less positive or a negative ethical climate can have an impact on healthcare professionals themselves (moral distress, burnout) or on the quality of the care provided. Within the framework of globalization (as this can relate to job retention and financial migration), healthcare reform (National and European), staff mobility within the European Union (EU) borders and the current fiscal climate, it is considered important to determine the perceptions of nurses in regard to the ethical climate in various healthcare settings. Mapping the ethical climate situation in any country allows for corrective measures to be assumed once a problem is appropriately diagnosed with valid, reliable, and sensitive instruments. The comparison between Greece and Cyprus as the first cross-country study comparing ethical climate aims to provide the evidence on whether nurses in different countries, with similar cultural and organizational contexts, may differ on the way they perceive the ethical climate in cancer care settings. Culture can affect health provision on many levels, such as on the level of individual beliefs held by healthcare professionals, or on the level of organizational patterns, practices, and group norms, which in turn might have an impact on the provision of personalized care. 23
The National Health Care System in Greece was founded in 1983. Basic goals of this healthcare system were equal provision and financing health services with complete cover of population and improvement of the health services’ organization. The Greek Health Care System can be characterized as a mixed system. It is financed by general taxes, social contributions, and state budget through compulsory social insurance. 24 The Cyprus Health Care System is also based on a mixed system and similar to the one implemented in Greece. There are public and private delivery systems. The public system is financed by Government and controlled by the Ministry of Health, whereas the private delivery system is financed by private healthcare insurance or by cash payments. 25
Aim of the study
The aim of the study was to evaluate the perceptions of nurses working in cancer care units in Greece and Cyprus on the hospital ethical climate.
The following objectives were set by the study: To identify any differences between Cyprus and Greece regarding the perceptions of cancer nurses on hospital ethical climate. To explore whether there is an association between the ethical climate and demographic data of cancer nurses.
Methods
Design
This was a quantitative descriptive–correlational comparative study in Cyprus and Greece.
Sample—selection criteria
The participants of the study were registered nurses who worked in hospitals in cancer care settings. The selection criteria were purposively left general as a means to include as many nurses as possible in the sample. Therefore, in principle, all registered nurses working in cancer care settings for over 6 months were eligible to take part in the study.
The minimum required sample size was calculated by power analysis (nQuery with statistical significance level of 5% and statistical power of 80%). In total, 81 nurses were recruited in Greece (response rate 55%) and 154 nurses in Cyprus (response rate 64%). A total of 235 nurses participated in the study.
Data collection procedure
The study followed a cross-national comparative design. The questionnaire employed was the Greek version of the HECS questionnaire. 25 The questionnaire was given to the participants attending two National conferences: the Pancyprian Nursing Oncology Congress (Cyprus) and Panhellenic Nursing Oncology Conference (Greece). These two conferences were purposively selected as each year they attract sufficient numbers of cancer nurses from across both countries.
Questionnaire
Several questionnaires have been developed to measure the ethical climate such as the HECS. The HECS was selected because it is short, easy to answer, created by nurses, and reflects the aim of the study. The questionnaire focuses on relationships between healthcare professionals. The HECS questionnaire was created by Linda Olson 15 in order to assess how nurses perceive the ethical climate in the area where they work. This questionnaire consists of 26 questions divided over five dimensions with which the nurse relates to. The five dimensions are Managers (includes six questions), Physicians (includes six questions), Peers (includes six questions), Hospital (includes six questions), and the Patients (includes four questions). The 26 questions can be answered with a 5-point Likert-type scale from 1 to 5 (1 = almost never to 5 = almost always) with higher values indicating a more positive ethical climate. The “Managers” dimension covers aspects in relation to respect, confidence, and support in the nurse–manager relation. The relation with “Physicians” mainly encompasses respect for and confidence in the physician and the involvement in treatment-related decisions. The “Peers” dimension reflects on issues concerning the support and the likelihood to depend on your colleagues in challenging situations. The “Hospital” dimension relates to the support provided to the nurse through the hospital’s mission as well as the available protocols and guidelines. Finally, the “Patients” dimension reflects the provision of information to the patient and having respect for the patient’s wishes.
The questionnaire includes demographic information such as gender, years of work experience, educational level, place of employment, and employment conditions. The HECS questionnaire was translated and evaluated in Greek for psychometric properties in cancer care settings by Charalambous et al. 25 and has a proven validity and reliability in Greek.
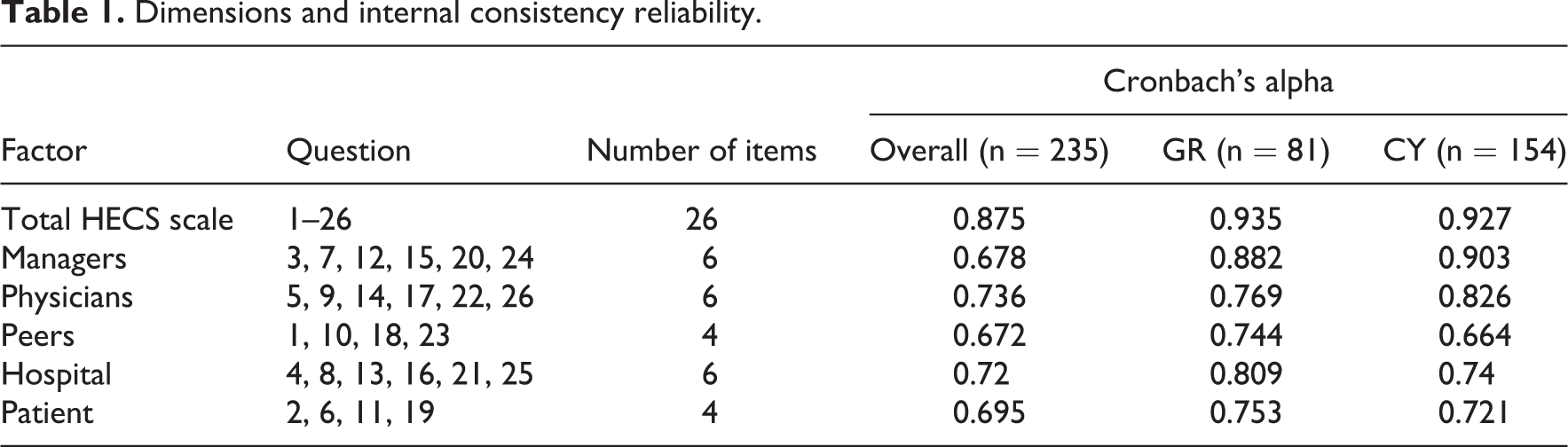
The five ethical climate dimensions are presented along with their constituent statements and Cronbach’s alpha internal consistency index. All dimensions presented adequate reliability coefficients ranging from 0.695 to 0.875 for the overall sample that is comparable to those reported in the validation study (Table 1).
Dimensions and internal consistency reliability.
Statistical analysis
Demographic characteristics are described as frequencies (N) and percentages (%). Also, descriptive statistics for the five resulting dimensions are presented with mean, standard deviation, and standard error. Independent samples t test was performed to investigate the differences for the subpopulations (Greece and Cyprus) for all five dimensions. The size of the differences in the level of the ethical climate between Greece and Cyprus was investigated using the effect size estimate of Cohen’s d. The linear associations between the dimensions of the instrument were explored using Pearson’s correlation coefficient. The association of the demographic characteristics with the level of the ethical climate was explored using a linear regression model. A regression model was deployed for each of the dimensions. Statistical significance was set to 0.05 and all analyses were conducted using SPSS v.21.
Ethical considerations
The study conforms to the principles of the World Medical Association Declaration of Helsinki and the relevant ethical approvals were obtained according to national law. Participants were informed about the purpose of the study, and the methodology and written consents were obtained. Anonymity was maintained throughout the entire procedure, and respondents’ participation was voluntary.
Results
Demographics
The sample of the survey consists of 235 nurses working in various cancer care settings. The participants are divided in two groups: 81 (34.5%) are working in hospitals in Greece and 154 (65.5%) in Cypriot hospitals (Table 2).
Demographic characteristics of the participants (N = 235).
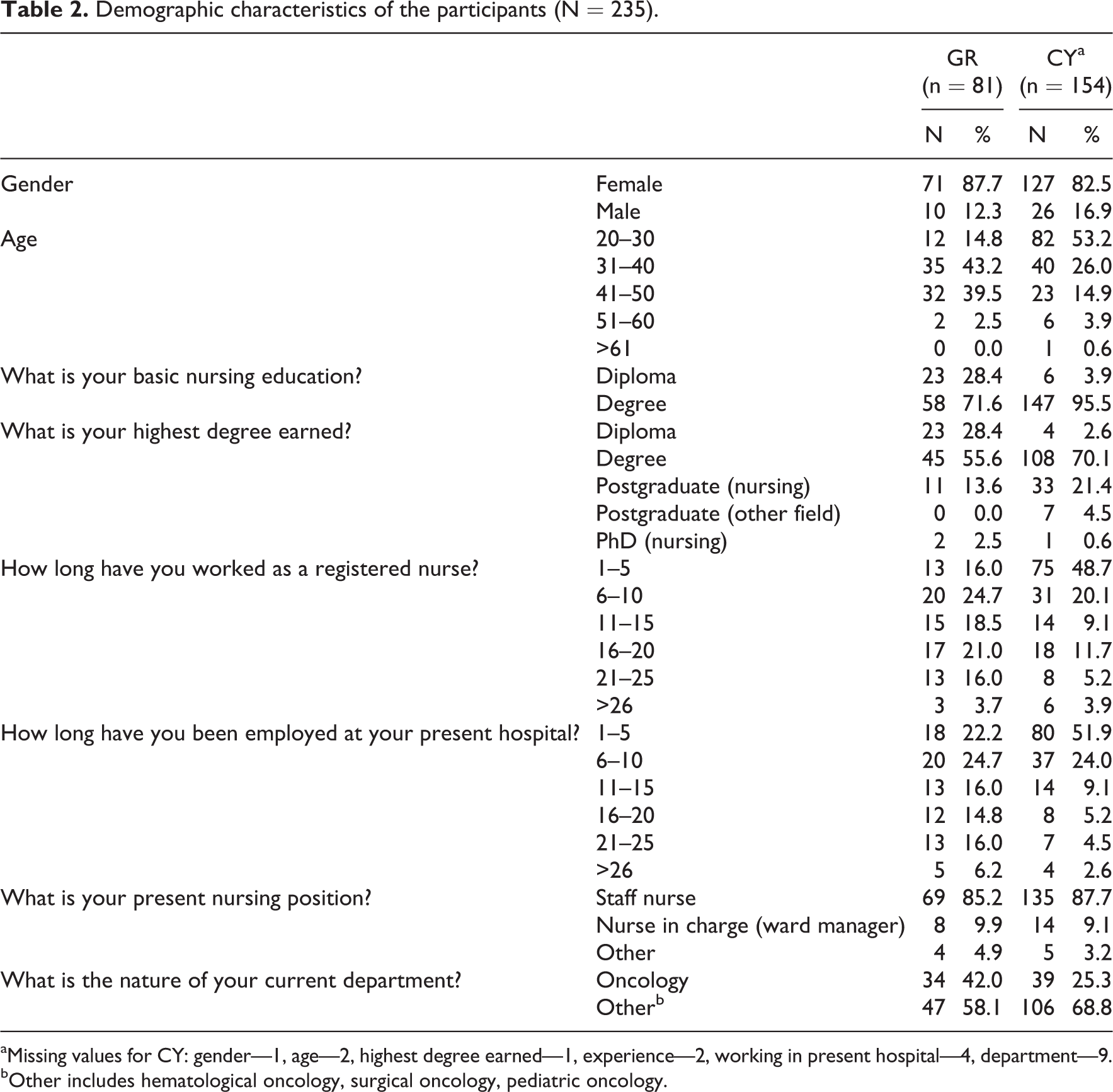
aMissing values for CY: gender—1, age—2, highest degree earned—1, experience—2, working in present hospital—4, department—9.
bOther includes hematological oncology, surgical oncology, pediatric oncology.
Greece (N = 81, 34.5%)
From the 81 participants working in Greek hospitals, 71 (87.7%) were female. Most of the participants (n = 35) were in the age group of 31–40 years (43.2%), followed by those in the age group of 41–50 years (n = 32) (39.5%). As far as their basic education, 23 (28.4%) held college diploma and 58 (71.6%) held a university degree. Most participants held a degree for 45 (55.6%) participants and the least (n = 2, 2.5%) held a PhD (nursing). Most participants had been working as a registered nurses for 6–10 years (n = 20, 24.7%) followed by those working 16–20 years (17, 21%). Most of the participants held a staff nurse’s position (n = 69, 85.2%).
Cyprus (N = 154, 65.5%)
A total of 154 (35.5%) nurses working in hospitals in Cyprus participated in this study, of whom 127 (82.5%) were female and most were in the age group of 20–30 years (n = 82, 53.2%). With regard to their basic education and their highest degree earned throughout the professional career, most participants had a university degree (n = 147, 95.5%) and most had earned a degree 108 (70.1%), respectively.
Most participants (n = 75, 48.7%) have been working as a registered nurses from 1 to 5 years, and 80 (51.9%) participants have been working from 1 to 5 years in their present hospital. As far as their position, 135 (87.7%) are staff nurses, 14 (9.1%) are ward managers (nurse in charge), and 5 (3.2%) have other positions.
Hospital ethical climate dimensions
Dimension scores calculation was done using the mean response of the items (Table 3). The results showed that in terms of the “Managers” dimension, participants working in Greek hospitals (4.30 ± 0.73) had a higher score compared to the Cyprus participants (3.66 ± 0.93) (t = −5.777, p ≤ 0.001). The size of the difference between Cyprus and Greece is large (Cohen’s d = 0.79). With respect to the other ethical climate dimensions, no statistically significant differences were observed between Cyprus and Greece. A low score in the dimension “Physicians” was observed in both countries. In the other three dimensions, the differences were not found to be large or statistically significant. However, the results show that the “Peers” dimension in Greece (M = 4.08) is quite high (Figure 1).
Descriptive statistics and comparisons of the five dimensions across Greece and Cyprus.
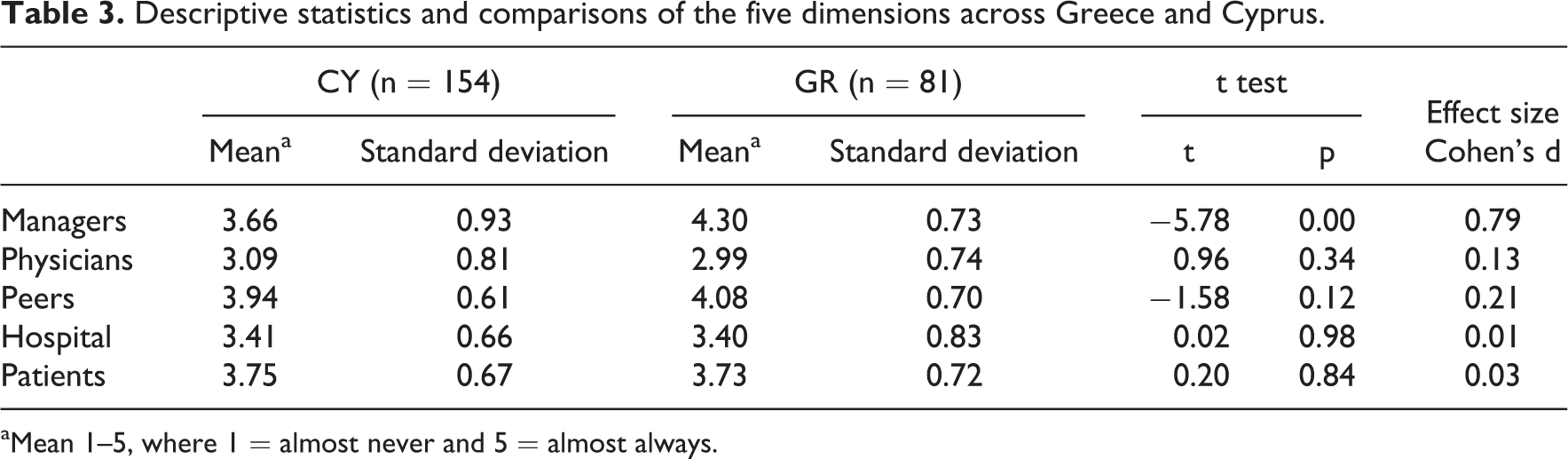
aMean 1–5, where 1 = almost never and 5 = almost always.

Mean level of the variables under study (with 95% confidence intervals).
Table 4 shows the total hospital ethical climate for both countries combined (3.58) and separately for each country in all dimensions. The total ethical climate for Greece was 3.67, whereas for Cyprus it was 3.53. Highest scores were identified in the Peers dimension (3.99), followed by the Managers dimension (3.88), the Patients dimension (3.74), and Hospital dimension (3.4). The lowest score was recorded in the Physicians dimension (3.06).
Descriptive statistics of the survey on ethical climate.
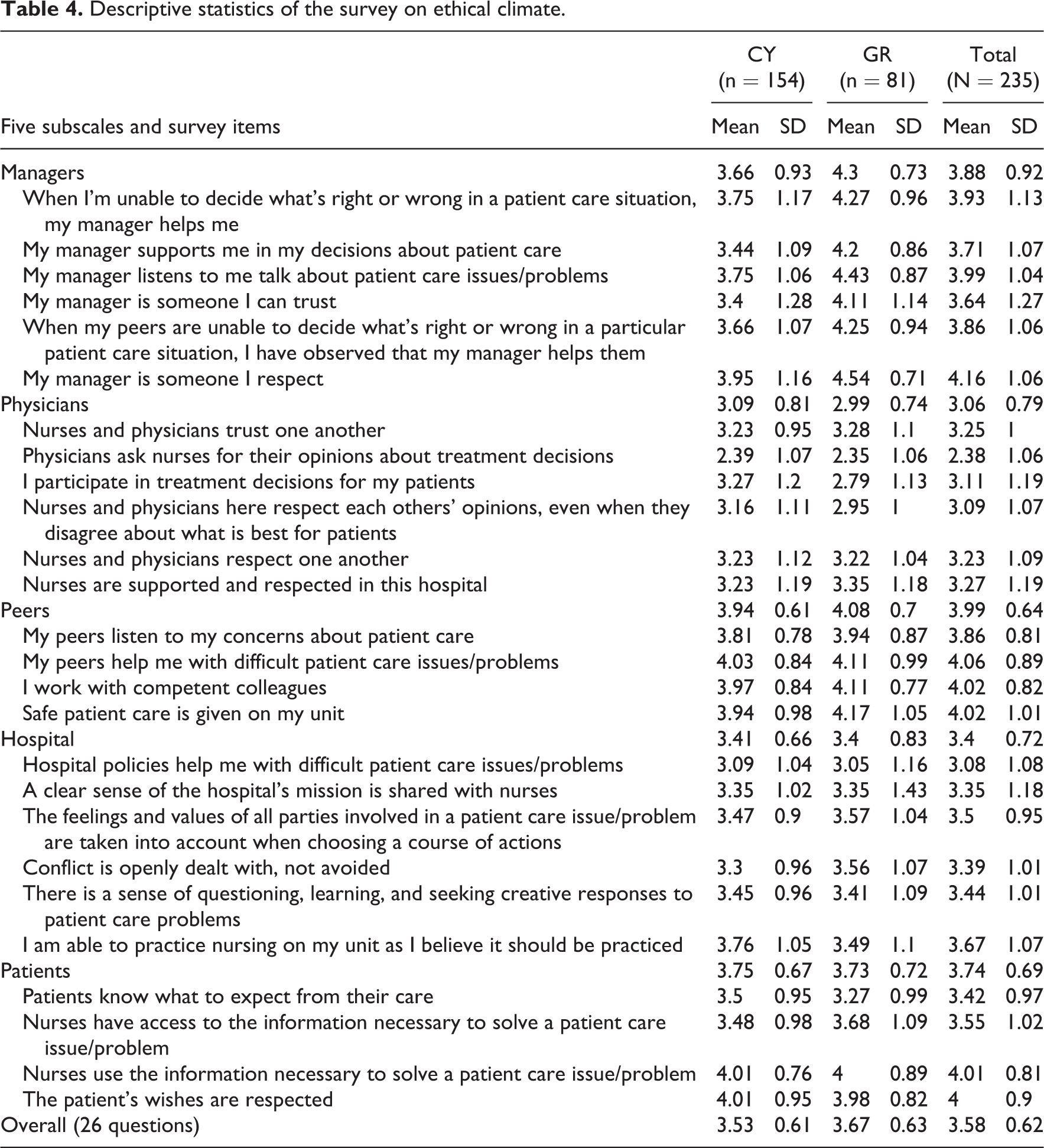
With respect to single item questions, the answer with the highest score was “My manager is someone I respect” (4.16), whereas the lowest score was for the answer “I participate in treatment decisions for my patients” (2.38). Low scores were also seen for the following items: “Hospital policies help me with difficult patient care issues/problems” (3.08) and “Nurses and physicians here respect each other’s opinions, even when they disagree about what is best for patients” (3.09).
Correlations
The linear associations between all dimensions were explored using Pearson’s correlation coefficient (Figure 2 and Table 5).
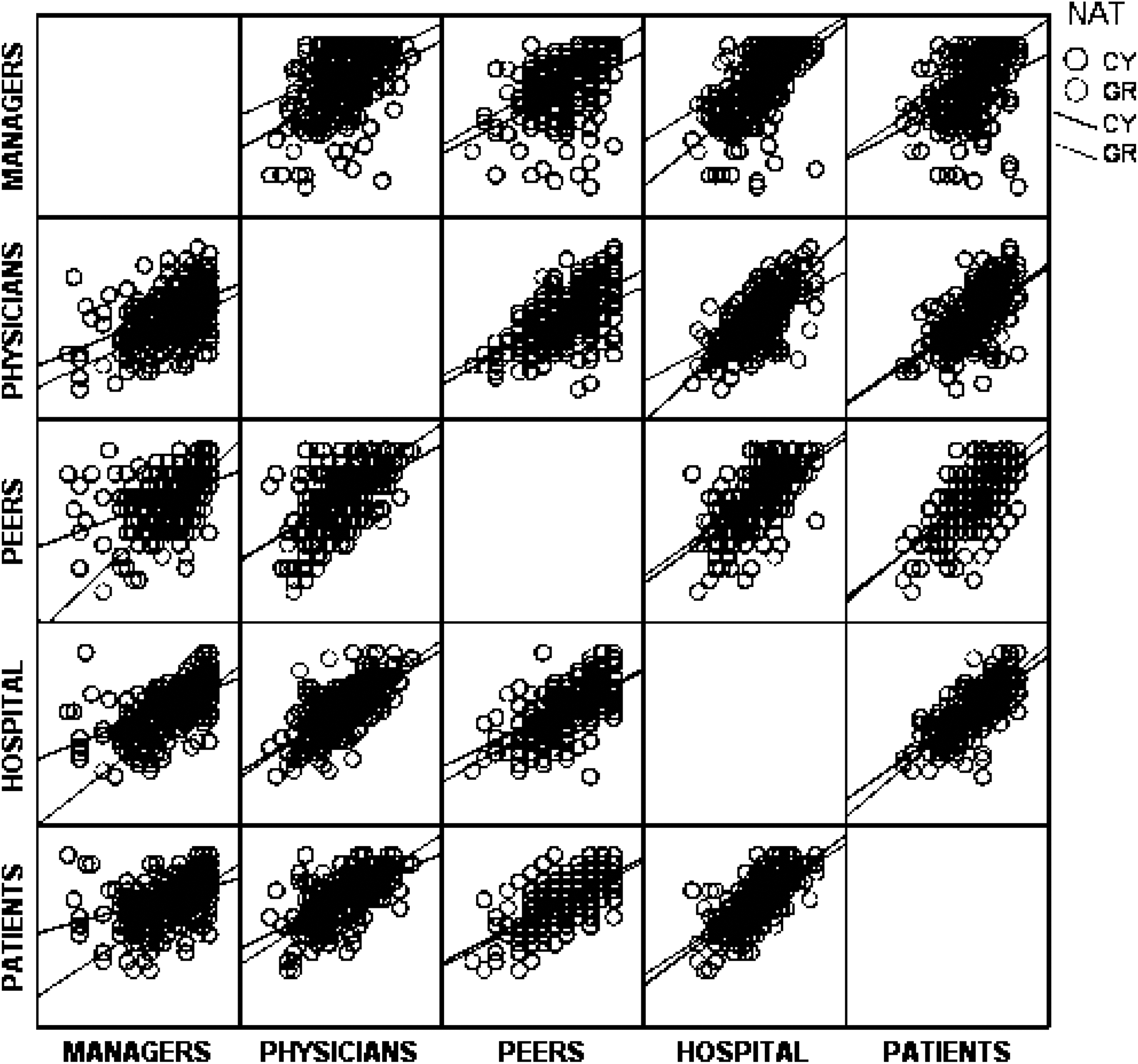
Scatterplot for exploring the linear association between the ethical climate dimensions.
Pearson’s correlation between ethical climate dimensions.
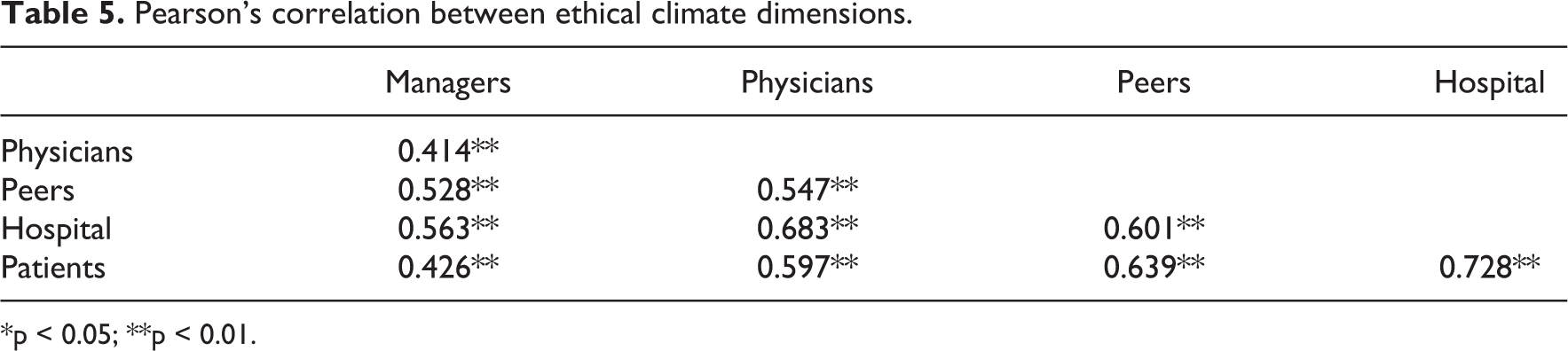
*p < 0.05; **p < 0.01.
All dimensions exhibit positive and moderate to high correlations between them (r = 0.414–0.728, p < 0.01). The highest correlation is observed between Hospital and Patients dimensions (r = 0.728, p < 0.01).
Regression analysis
All demographic variables were incorporated into a linear regression model for exploring the possible associations with the dimensions of the ethical climate. A separate regression model was deployed for each of the dimensions (Table 6).
Linear regression associating the demographic variables with the ethical climate dimensions.
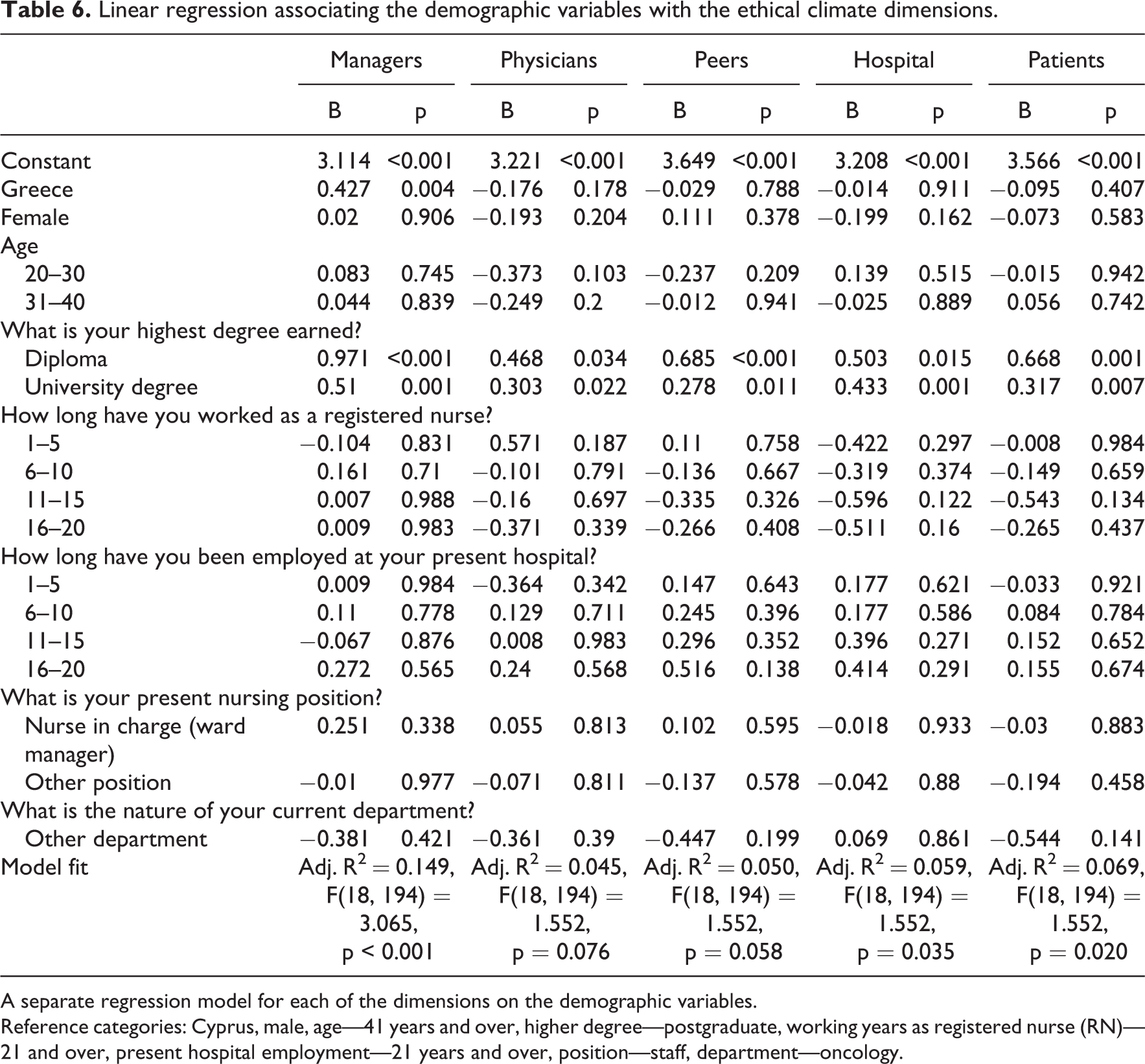
A separate regression model for each of the dimensions on the demographic variables.
Reference categories: Cyprus, male, age—41 years and over, higher degree—postgraduate, working years as registered nurse (RN)—21 and over, present hospital employment—21 years and over, position—staff, department—oncology.
Managers
The linear regression model explains 14.9% of the variation of the “Managers” dimension of the ethical climate (adj. R2 = 0.149, F(18, 194) = 3.065, p < 0.001)
Nurses in Greece have scored higher on the “Managers” ethical climate dimension compared to nurses in Cyprus by 0.43 points (in a scale of 1–5) on average (b = 0.43, p = 0.004).
The highest degree earned is associated with the level of “Managers” ethical climate. Specifically, nurses with diploma or University degree have on average 0.971 (p < 0.001) or 0.51 (p = 0.001) points, respectively, higher ethical climate than nurses with a postgraduate degree (MSc or PhD).
No other demographic factors were found statistically significantly associated with the level of Managers’ ethical climate.
Physicians
The linear regression model explains 4.5% of the variation of the Physicians’ dimension of the ethical climate which is not statistically significant (adj. R2 = 0.045, F(18, 194) = 1.552, p = 0.076).
However, the results showed that the highest degree the nurses earned is associated with the level of physician’s ethical climate. Specifically, nurses with diploma or university degree have on average 0.468 (p = 0.034) or 0.303 (p = 0.022) points, respectively, higher ethical climate than nurses with a postgraduate degree (MSc or PhD).
Peers
The linear regression model explains 5.0% of the variation of the Peers dimension of the ethical climate which is not statistically significant (adj. R2 = 0.050, F(18, 194) = 1.552, p = 0.058). Still, the highest degree earned is associated with the level of Peers’ ethical climate. Specifically, nurses with diploma or university degree have on average 0.685 (p < 0.001) or 0.278 (p = 0.001) points, respectively, higher ethical climate than nurses with a postgraduate degree (MSc or PhD).
Hospital
The linear regression model explains 6.0% of the variation of the Hospital dimension of the ethical climate (adj. R2 = 0.059, F(18, 194) = 1.552, p = 0.035).
Only the highest degree earned was found to be associated with the level Hospital’s ethical climate. Nurses with diploma or university degree have on average 0.503 (p = 0.015) or 0.433 (p = 0.001) points, respectively, higher ethical climate than nurses with a postgraduate degree (MSc or PhD).
Patients
The linear regression model explains 7.0% of the variation of the Patients dimension of the ethical climate (adj. R2 = 0.069, F(18, 194) = 1.552, p = 0.020).
The highest degree earned was found to be associated with the level Hospital’s ethical climate. Nurses with diploma or university degree have on average 0.668 (p = 0.001) or 0.317 (p = 0.007) points, respectively, higher ethical climate than nurses with a postgraduate degree (MSc or PhD).
Discussion
This study explored the hospital ethical climates in Cyprus and Greece, their differences, and its’ associations to the participants’ demographical data. The HECS questionnaire, with its five dimensions, helped to formulate and examine the level of the ethical hospital climate in both countries and to compare both levels, respectively. Finally, it allowed the researchers to speculate about the possible reasons that determine the moral climate for cancer nurses in both countries.
The total reliability of the HECS was found a = 0.86 and for the five subscales ranged from 0.71 to 0.85. The validity and reliability of the HECS is comparable to those found in the original study by Olson, where the total reliability was found a = 0.91 and ranged from 0.68 to 0.92 for the subscales.
The difference between Cyprus (M = 3.53) and Greece (M = 3.67) was statistically significant (p < 0.001), with more positive hospital ethical climate being reported by nurses in Greece. The Peers dimension (3.99) represented the highest score, as it seems that relationships between nurses are quite good, and points toward the presence of a spirit of cooperation and support. A high score was also found in the Managers dimension (a total of 3.88), where Greece had a mean score of 4.30 and Cyprus 3.66. A possible explanation can be that nurses involved in caring for people with cancer in Greece have better relationships with their supervisors than nurses working in similar departments in Cyprus. In relation to Cyprus, it is likely that they received greater support from their supervisors when it came to decision-making and patient care.
The responses of nurses working in Greece indicate that they have somewhat more trust in their supervisors and greater respect for them. In a preceding study, 21 the results showed that the moral climate of nurses was directly related to job satisfaction and perceived organizational support. 21 The importance of manager’s support on the ethical climate has also been stressed in a qualitative study with registered nurses in New Zealand. 26
A high score on the “Managers” dimension has been also observed in other studies in the international literature. 27 –29 A study conducted by Suhonen et al. 8 in Finland observed a high score in the Peers dimension (4.29) and a low score in the Physicians dimension (3.58). It appears that the relationships between nurses were better than those of other healthcare professionals. The high score in the Peers dimension may be due to the fact that the authors studied nurses working in acute care settings and nursing provided at home. This can be partially explained by the more independent roles that nurses assume in the home setting compared to those in the acute care setting, whereas decision-making in relation to ethical issues within the hospital setting lays in most cases with the medical professionals.
In this study, a less positive hospital ethical climate score was observed in the Physicians dimension in Greece and Cyprus. This seems to suggest that nurses believe that physicians do not take nurses’ opinions into consideration when treating patients. It is likely that there is poor or no mutual respect and trust between them. The same results were consistently observed in similar studies studying the ethical climate in various clinical contexts. For example, less positive ethical climate with regard to Physicians dimension was found in nurses working in public hospitals in Iran, cancer nurses in Israel, nursing staff in public nursing homes in Korea, registered nurses in Canada, and nurses involved in acute care. 11,22,29
The low score in the Physicians dimension might also indicate that there is a lack of support and cooperation between doctors and nurses regarding patient care and one that threatens nurses’ autonomy. 30 In a study of 463 registered nurses, Hart 31 reported the ethical climate in acute care hospitals to be the most important variable predicting turnover intention, staffing, workload, and feelings of autonomy. The lack of trust, respect, and support creates a negative climate in the care sector and is a source of stress and dissatisfaction among nurses. 32,33 Consequently, this has an impact on patients, patient care, in general, and the ethical climate of the healthcare institution itself. In a study of 10,000 nurses, only 58.7% of them said that they could provide the care they would like to patients in the prevailing climate. 20
The relationship between nurses and physicians is related to the fact that maybe they perceive the ideal working environment differently. The collaboration of healthcare professionals and the existence of a well-structured team are indisputably necessary in the health sector, since in a study carried out on a large sample of general nurses, the nurses stated that the ideal team should provide its members with the feeling that they belong (96.1%), that there is someone who can guide them and support them (89.3%), and that in difficult situations they can trust and rely on their colleagues (88.4%). A good relationship between nurses and supervisors could also help improve relationships between nurses and physicians if the latter develop strategies as departmental leaders. 34 At the same time, it is worth noting that good relationships between healthcare professionals, and the presence of a group to which they can be relegated and from which they can draw support, are essential, since these affect stress levels and the quality of healthcare provision. 33
An analysis of the participants’ demographic data showed that the only characteristic that could have influenced the ethical climate of the cancer nurses was the variable referring to their level of education. Specifically, the results indicated that nurses who had a higher education (MSc or PhD) had approximately one unit less in relation to their ethical climate score (i.e. it was less positive) than other nurses who held a diploma or degree. A study in Finland involving nursing care for the older people, as well as a study by Lilia et al., 35 revealed similar results. However, a study by Numminen et al. 36 that examined newly graduated nurses’ perception of the ethical climate in their workplace environment and its association with their self-assessed professional competence found their overall perception of the ethical climate as positive.
The findings can be attributed to several factors. This may be due to the fact that their education may have led them to have higher demands and expectations than other healthcare professionals within the organization they worked in. One would expect nurses with a higher level of education to have better relationships with other healthcare professionals, as they have more knowledge advanced communication skills and are more prone to work in multidisciplinary teams. However, Lilia et al.’s 36 study showed that nurses with less knowledge feel less competent when it comes to providing adequate care due to a lack of knowledge of other treatment methods, thus resulting in lower ethical climate scores.
On the one hand, and based on this study, one might consider that since the results showed low scores for nurses with higher education, the opposite may as well be the case. It may be the case that due to their knowledge, they might have expressed views on patient care more frequently than doctors cared to acknowledge—as demonstrated by the low score on the Physicians dimension—and their resulting sense of resentment is evident. On the other hand, one would expect that the nurses with greater work experience in the field of healthcare receive greater respect and are more likely to maintain cooperative ties with physicians. However, there has not been any statistically significant difference between the participants in relation to their years of work. It seems that the length of employment does not affect the physicians’ attitudes toward nurses when it comes to decision-making and patient care.
However, similar studies have observed different findings. For example, in the studies by Mobasher et al. 32 and Borhani et al., 37 no statistically significant relationship between the demographic data and the ethical climate of the participants was observed. In contrast, Bahcenik and Oztürk 27 and Goldman and Tabak 9 found a relationship between the demographic data and the ethical climate, particularly in relation to age and the years of work experience.
According to the results of this study, if nurses’ educational level is known, then it is possible to assume, at least to some extent, the ethical climate of nurses working in similar work contexts. Nothing can be said in absolutist terms as this concerns different people with different individual traits and expectations.
Preceding studies in other nurse specialist groups found that nurses caring for people at home (HECS total score 3.89) had higher scores on the ethical climate scale total score compared to those nurses working in acute care (HECS total score 3.79). Furthermore, higher scores were observed for nurses working in private nursing homes (HECS total score 3.82) compared to those working in public nursing homes (HECS total score 3.76).
The difference between the total scores was not statistically significant but still worthy of mention. A more positive ethical climate was discerned in private nursing homes, since as reported by the participants in Ghorbani et al.’s 34 study, private nursing homes undertake studies on quality control standards and quality of care. It appeared that the nurses working in the cancer departments had a lower HECS total score (3.58) compared to nurses working in other clinical settings. The highest ethical climate score was observed in nurses working in the community service and those working in the private sector, which might ultimately indicate that nurses’ work environment plays a part in how they perceive the ethical climate of the organization within which they work.
Limitations
The study is not without limitations. A significant limitation is the convenience sample that was retrieved during two national conferences. Although a good representation of nurses working in the various cancer care settings is generally present in these conferences, the findings should be generalized with caution. Finally, the results may not be fully comparable with studies where the participants come from a different cultural background. In addition, this study focuses purposively on the relationships between healthcare professionals; therefore, other aspects of the ethical climate were not explored.
Conclusion
The ethical climate in cancer care settings can be different between countries with seemingly similar cultural contexts and healthcare systems. However, several similarities were also observed in specific dimensions of the ethical climate.
Ethical climate is a complex concept and the consisting dimensions interlink with each other. This means that any attempt to improve the ethical climate in the cancer care context should be directed toward all the constituent elements of ethical climate. However, based on the results, there is need to address these interventions primarily at improving collaboration and relationships with physicians and promoting organizational support.