
Abstract
Background:
Moral distress is considered to be the negative feelings that arise when one knows the morally correct response to a situation but cannot act because of institutional or hierarchal constraints.
Objectives:
To analyze moral distress and its relation with sociodemographic and academic variables in undergraduate students from different universities in Brazil.
Method:
Quantitative study with a cross-sectional design. Data were collected through the Moral Distress Scale for Nursing Students, with 499 nursing students from three universities in the extreme south of Brazil answering the scale. The data were analyzed in the statistical software SPSS version 22.0, through descriptive statistical analysis, association tests (t-test and analysis of variance), and linear regression models.
Ethical considerations:
Approval for the study was obtained from the Research Ethics Committee at Universidade Federal do Rio Grande.
Findings:
The mean intensity of moral distress in the constructs ranged from 1.60 to 2.55. As to the occurrence of situations leading to moral distress in the constructs, the frequencies ranged from 1.21 to 2.43. The intensity level of moral distress showed higher averages in the more advanced grades of the undergraduate nursing course, when compared to the early grades of this course (between 5 and 10 grade, average = 2.60–3.14, p = 0.000).
Conclusion:
The demographic and academic characteristics of the undergraduate nursing students who referred higher levels of moral distress were being enrolled in the final course semesters, were at a federal university, and had no prior degree as an auxiliary nurse/nursing technician.
Introduction
Nursing undergraduate students experience moral distress (MD) in situations of conflict or dilemma involving ethical-moral values and the impossibility of acting during academic training. 1 Students have a profound sense of responsibility toward their patients, and this is confronted in cases of morally inadequate situations in which they may feel unable to act because of hierarchical issues and preoccupation with the evaluation of teachers. This may generate moral distress in them. 2
Interest in this subject nowadays has broadened this field of research, moving from the first investigations focused on health professionals to students in the health area. Specifically, moral distress was investigated in nursing students in Brazil1, 3 –5 and internationally. 6 –13
Thus, it is relevant to explain that students face their own moral problems 14 in the training environment they are inserted in, which may reveal the confrontation with dubious circumstances related to the exercise of autonomy, ethics, and morality. In this perspective, elucidating the situations that cause moral distress in undergraduate nursing students, in the training environments, can provide a description of the university weaknesses 5 and directly influence the defense and valuation of the students themselves, as well as the qualification of their education.
The theme moral distress has its origin in the problematization of the daily routine of nursing professionals. In this sense, little investigation has been done on moral distress in nursing students, 3,11,13 although their exposure to morally distressing situations is admittedly broad, especially due to the compliance with educational experiences in the clinical environment. Thus, when witnessing unhealthy behavioral circumstances and behaviors, incompatible with their values, principles, and standards learned in their academic education, the students, in the same way as professional nurses, perceive moral distress, 13 validating and justifying the need to investigate its occurrence in other settings, such as the academy. 1,3,4,15
Therefore, looking at the training environment of undergraduate nursing students may reveal that many moral confrontations associated with moral distress in students relate to the conditions of the university context. Thus, the presence of moral distress in nursing students indicates the need to develop coping and intervention strategies to be taught in the academic environment, by all nursing schools, in order to maintain the students’ well-being and to ensure high-quality academic training, 10 factors that demonstrate the relevance of expanding the knowledge about this subject in nursing students.
Conceptual and theoretical framework
Jameton 16 devised the concept of moral distress in the literature in the 1980s from situations experienced by nursing professionals in the hospital work environment, presenting his concept as the negative feelings that arise when one knows the morally correct response to a situation but cannot act because of institutional or hierarchal constraints.
Therefore, moral distress is a broad concept that discusses a range of experiences of morally constrained individuals and can be understood as a response to individual, institutional, or social constraints. To date, individuals may be restrained by personal causes, such as fear or unwillingness, or situational constraints, such as hierarchical decision-making or lack of resources. 17,18
In this sense, ethical problems were classified into three categories: moral uncertainty, when a problem is recognized as a morally inappropriate or incorrect situation; moral dilemma, when based on a moral problem, two or more ethically justifiable actions can be taken and, often, there are significant disadvantages to each potential solution; and moral distress, when the ethically appropriate action to solve a moral problem has probably been identified, but there are countless barriers for its implementation. 16
In the context of quantitative research on moral distress, Ramos et al. 19 developed a Brazilian instrument to measure the intensity and frequency of moral distress in nurses aiming to broaden the understanding of the theme from moral, political, and social aspects in the Brazilian context. The instrument presents questions about prolongation of life, therapeutic futility, professional incompetence, omission toward patients, and among others.
Nursing students also experience moral distress when they witness situations that are morally inadequate, particularly circumstances of care and behavior that are morally inadequate in the academic environment, situations of disrespect toward patients and their rights. 5,10 In this context, the students opts for silence to preserve the field of practical activity and the opportunities for learning. 4,5 These situations are incompatible with their values, principles, and personal standards learned during academic training and possibly cause them to experience moral distress.
Aim of the study
To analyze moral distress and its relation with sociodemographic and academic variables in undergraduate nursing students from different universities in Brazil.
Method
Study design
This is a quantitative study with a cross-sectional design. 20 It was carried out using the Moral Distress Scale for Nursing Students (ESMEE a ), previously validated, involving nursing students from three universities in Brazil.
Participants and place of study
The study was conducted at three universities located in two municipalities in the extreme south in Brazil—two courses belong to public universities and one to a private university. The study participants were undergraduate nursing students from three Brazilian universities, enrolled from the first to the final semester.
The criteria for the participants’ inclusion were restricted to being a student in the undergraduate nursing course at the selected universities and being available and interested in answering the instrument. The exclusion criteria were limited to the student’ absence from the place and at the time of data collection (due to academic mobility, outpatient regimen, and cancelation) and lack of availability or interest in participating in the research.
To select the participants, the non-probabilistic convenience sampling method was used, so that the informants were selected according to their presence and availability in the place and at the time the data collection process was implemented.
Also, previously knowing the total population, composed of 802 nursing students, divided into 411 in U1, 223 in U2, and 168 in U3, the application of the formula to these data resulted in the minimum sample of 263 informants. The final sample consisted of 499 students, and the losses corresponded to 303 because 280 students were not in the classroom during the data collection, 15 refused to participate, and 8 data collection instruments were returned blank.
Data collection
The data collection was carried out from 01 November to 20 December, 2015, through visits to the different classes of the undergraduate nursing courses at the three selected universities, previously scheduled with the professors of the subjects taught. All the classes of the institutions studied were visited, totaling 26 classes between the 1st and 10th semesters at the three universities, with 10 classes in U1, 9 classes in U2, because there was no class in the 10th semester, and 7 classes in U3, as there were no classes in the first, third, and fifth semester.
The previously trained collectors were presented and the students were invited to participate in the study; soon after the delivery of the instruments, the research objectives and the adopted method were described, reading the first sheet of the instrument and explaining its completion form. Students in the 9th and 10th semesters were contacted through classroom meetings or in the training area.
Instrument
The ESMEE was developed to be applied in quantitative studies. A guide with eight steps 21 was used to develop a scale intended to measure moral distress among undergraduate nursing students, to measure the frequency and intensity of moral distress experienced by nursing students.
The ESMEE was previously validated with a sample of 499 nursing students. The instrument contains 41 items on situations that can generate moral distress in nursing students related to dimensions of the academic environment, attitude of teachers, institutional/organizational environment, and practical/clinical environment.
The measurement of the frequency and intensity of moral distress reported by the students was performed using two seven-point Likert-type scales, one measuring the intensity of moral distress in a range from 0 (none) to 6 (very intense distress), and the other measuring the frequency of situations that generate moral distress occur in the range from 0 (never) to 6 (frequently).
The six constructs obtained correspond to different situations the nursing student can experience in the academic training environment and which can generate moral distress. In this sense, the construct C1: Commitment of the ethical dimension of user care is defined by aspects related to the users’ rights to privacy, security, and proper care. 2,9,10,13 Construct C2: Improper institutional conditions to teach user care in the institutional and organizational care system, is related to problems of professional incompetence, access to appropriate care, lack of continuity of care, and resource allocation. 10,13 With regard to C3: Authoritarian teaching practices, aspects of interpersonal relationships between student and teacher are mentioned, in which the nursing teachers demonstrate lack of support and excessively critical behavior, contributing to an uncomfortable learning environment. 9,13
Furthermore, construct C4: Lack of competence of the teacher includes factors related to the commitment of teacher qualification, in the use of appropriate methods, as well as in the distribution of the curricular contents, the consistency of the disciplines offered and the similarity between the contents taught and the practical reality. 11 Construct C5: Disrespect for the ethical dimension of vocational training encompasses situations of plagiarism, change of grades, and inappropriate behavior. 15 And construct C6: Professional choice includes the choice of the undergraduate course, continuation in the course and feelings of professional devaluation. 3
The six dimensions of the instrument explain 65.8% of the variation in the items. The instrument and dimensions presented satisfactory internal consistency, with Cronbach’s alpha equal to 0.970 and between 0.60 and 0.97, respectively. This analysis enabled verifying that the items of each construct analyzed together converged to a single factor, suggesting they are all one-dimensional. Hence, the Kaiser–Meyer–Olkin test of sampling adequacy (KMO = 0.967) and Bartlett’s test for sphericity are (chi-square = 14681.429).
In relation to the sample characteristics, on the initial page of the instrument, items were included for the student to complete, related to the university; current semester/grade; sex; age; number of times he was not approved in courses along the semesters; year of entry into the course; prior degree; and paid activity. On the initial page, the instrument also displayed an introductory text where the definition of moral distress and the form of completion were explained.
Data analysis
Data were analyzed using the statistical software SPSS (Statistical Package for Social Sciences), version 22.0. The following analyses were carried out: (1) descriptive statistics, through means and frequency distribution to identify the intensity and frequency with which the students experience moral distress; (2) analyses of variance among groups of respondents, according to characteristics of the sample to verify possible significant differences between groups of respondents; and (3) regression analysis to evaluate which constructs had the greatest effect on the nursing perceptions of students about the experience of moral distress.
Ethical aspects
The ethical aspects were respected in accordance with the recommendations of National Health Council Resolution 466/12. 22 Approval for the study was obtained from the Research Ethics Committee of the Federal University of Rio Grande (Opinion 097/2013).
Access to the scenario was obtained through a document sent to the Head Office of the three Universities, requesting the permission for the execution of the project, specifying the objectives of the study and the possible risks and benefits involved. All participants received information about the purpose of the study before responding to the scale, as well as information that their participation was voluntary, they could withdraw from the study as they wanted, questionnaires were anonymous, and data management would be confidential. Each participant returned an informed consent form. The universities studied were identified using the letter U followed by a sequential number (U1, U2, and U3).
Results
The sample consisted of 499 nursing students: 384 from public universities and 115 from private universities; 232 students were enrolled between the 6th and 10th semester, 56.3% never failed any subject and 57.7% started the course in the past 3 years. Among the students, 440 (88.2%) were female. With respect to age, the average was 24.8 years, ranging from 17 to 60 years, and the mode was age 22. The majority of the students also affirmed that they did not work, 389 (78%) and, of the remainder, (13.4%) reported working in the health area. In addition, 110 students (22%) reported having prior training, and 99 (19.8%) of them as nursing technicians/auxiliary nurses.
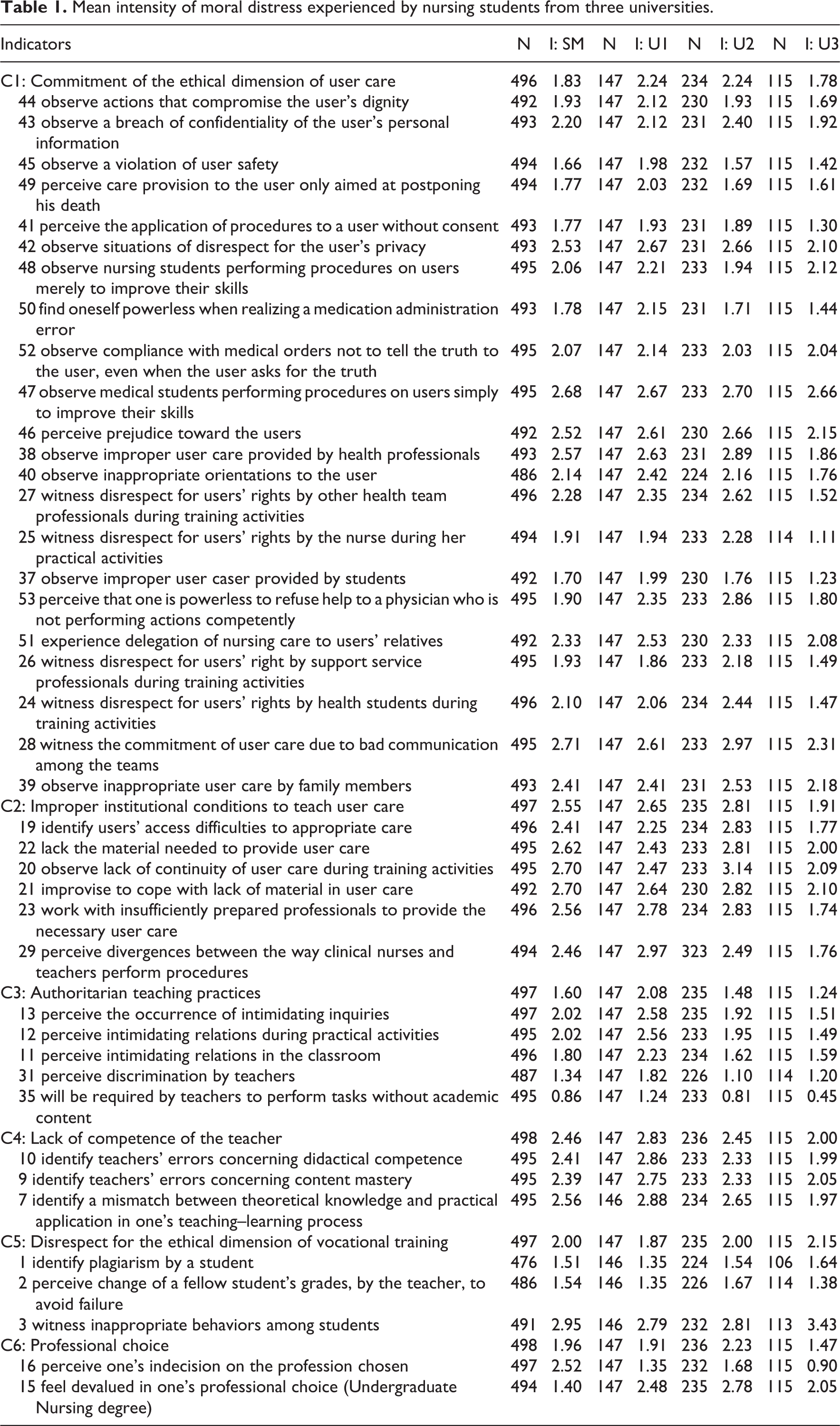
The mean intensity of moral distress in the constructs ranged from 1.60 to 2.55 (Table 1). As to the occurrence of situations leading to moral distress in the constructs, the frequencies ranged from 1.21 to 2.43. Thus, the mean frequency for U1 is as follows: C1 (1.84), C2 (2.65), C3 (1.70), C4 (2.53), C5 (1.80), and C6 (1.71). For U2, averages were as follows: for C1 (1.71), C2 (2.60), C3 (1.02), C4 (2.09), C5 (2.21), and C6 (1.78). For U3, averages were as follows: for C1 (1.52), C2 (1.80), C3 (0.97), C4 (1.65), C5 (2.00), and C6 (1.43).
Mean intensity of moral distress experienced by nursing students from three universities.
Based on the variance analyses performed, some important correlations were identified with 5% significance (Table 2). First, through the t-test, looking for significant differences among the data groups, it was verified that students under 25 years present significant correlations between moral distress and construct C6: Professional choice. Meanwhile, students in the final grades identified a higher average moral distress in general and in five constructs, except construct C6.
Comparison of moral distress intensity according to demographic and academic variables.

* Significance at 5%.
In relation to the prior training, students who were nursing technicians presented lower levels of general moral distress and in the following two constructs: C1: Commitment of the ethical dimension of user care and C3: Authoritarian teaching practices, in relation to students who had prior training in other areas. In addition, students who failed, one or more times, presented higher intensity levels of moral distress in the following two constructs: C3: Authoritarian teaching practices and C6: Professional choice, compared to students who had never failed.
Through analysis of variance (ANOVA; Duncan test), it can be inferred that the level of moral distress is more significant in the more advanced series (between 5th and 10th) of the undergraduate nursing degree, compared to the initial course grades. In relation to the constructs and the grades in general, construct C1: Commitment of the ethical dimension of user care has evidenced influence on the students from 5th to 10th grade. On the other hand, construct C2: Improper institutional conditions to teach user care showed higher means to generate moral distress in students between the 7th and 10th semester (Table 3).
Comparison of moral distress intensity by grades.

* Significance at 5%.
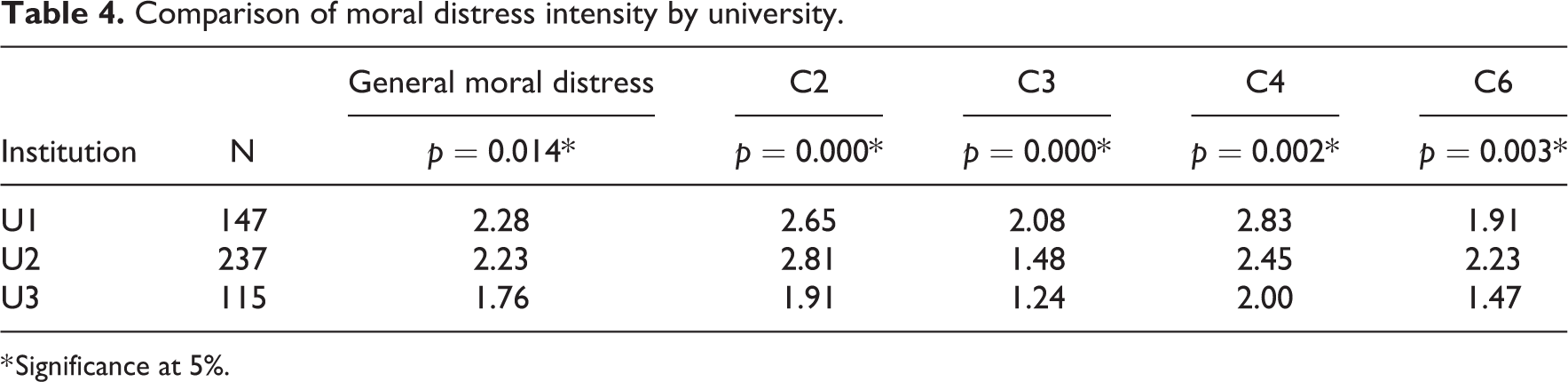
Correlations were obtained at the level of 5% with post hoc analyses in the Duncan test (Table 4), so that homogeneous groups could be identified in each of the variables. The results of the federal universities showed significant correlations in general moral distress and in four constructs: C2: Improper institutional conditions to teach user care, C4: Lack of competence of the teacher, C3: Authoritarian teaching practices, and C6: Professional choice, compared to the private university. On the other hand, construct C3 presented the highest isolated average in U1.
Comparison of moral distress intensity by university.
* Significance at 5%.
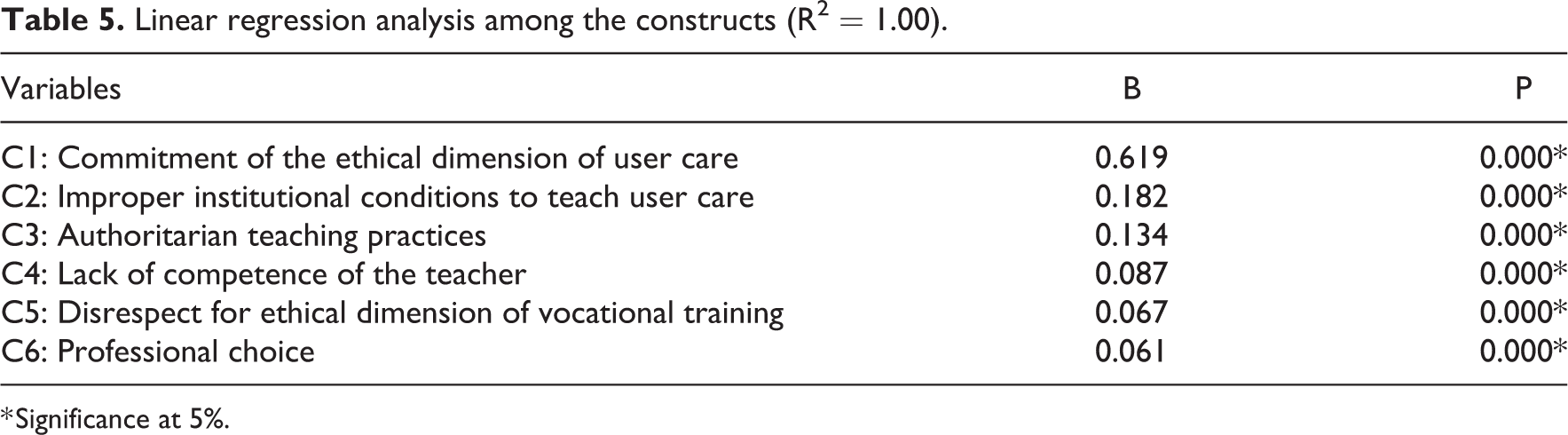
In the evaluation of the effects of the six constructs in relation to moral distress in nursing students, using the linear regression model, the mean of the six constructs was calculated; thus, the mean value was used as the dependent variable. The results identified a significance relation at 5% in all constructs. The construct with the strongest effect on moral distress in nursing students was C1: Commitment to the ethical dimension of user care (Table 5). The test obtained 1.00 as an adjusted determination coefficient (R2), representing 100% of explanation of moral distress in nursing students based on the validated questionnaire.
Linear regression analysis among the constructs (R2 = 1.00).
* Significance at 5%.
Discussion
Relationship between the dimensions and moral distress
The research of moral distress in undergraduate nursing students from three Brazilian universities through the ESMEE, with six constructs to present situations that can generate moral distress in the academic environment, showed lower means of intensity and frequency than other international study with nursing students. 9 In this sense, it is relevant to consider the high levels of moral distress identified among Brazilian nursing professionals, 23 –25 who, according to the literature, 13 share their experiences and frustrations with nursing students during practical teaching activities.
In this sense, this result may be related to the fact that the concept of moral distress is still little debated in the Brazilian academic environment. This raises more difficulties for the students to recognize certain situations as moral problems, identifying them as something common, recurrent in their work routine, or even more, as something peculiar to the practice of their profession, thus demonstrating a certain degree of conformity and passivity with these experiences. 1,4,13
In this context, moral and ethical training should take place horizontally, throughout the professional training process, through the constant problematization of the academic and health environment, with a view to developing the students’ ability to evaluate and judge certain situations and, consequently, their decision-making to solve them. Thus, the possibility of students facing moral problems is reduced, due to few opportunities to discuss moral and ethical issues, their hierarchical position and the permanent concern with teacher evaluations, 2,11,13 and factors that substantially generate moral distress.
In the analysis of the moral distress levels per university surveyed, and of each university in relation to the six constructs, it was observed that the federal universities (U1 and U2) presented higher mean moral distress levels than the private university (U3). Likewise, higher means were identified in constructs C2: Improper institutional conditions to teach user care, C3: Authoritarian teaching practices, C4: Lack of competence of the teacher, and C6: Professional choice.
In this sense, in relation to the construct C2: Improper institutional conditions to teach user care, the nursing students seem to demonstrate their dissatisfaction with the fragility of the public health environment and its organization. In Brazil, there have been recurrent reports of weaknesses in the health system, especially in public hospitals, where overcrowding and insufficient material and human resources commonly create difficulties in the provision of health services, factors that often generate moral distress in nursing professionals. 26
Similarly, nursing students, because they share this context with health professionals, may experience moral distress; therefore, educational institutions and teachers need to realize the importance of providing a favorable academic education environment, especially when precarious institutional conditions, which can cause moral distress, are identified.
The constructs, C3: Authoritarian teaching practices and C4: Lack of competence of the teacher, characterized in this study by events of intimidating relationships and inquiries; errors related to didactic competence, content mastery, and mismatch between theory and practice, may be associated, at federal universities, with the teachers’ employment relationship as tenured public servants. This institutional affiliation modality can contribute to a naturalization and consequent institutional acceptance of certain authoritarian and incompetent practices. 27 Therefore, it is important to emphasize that students from public and private educational institutions pay for the education received, either indirectly through taxes or directly by paying tuition.
Thus, when the students’ possible claims related to authoritarianism and lack of competence of the teacher are not met, they may choose to leave the course and even the university. When the institution is private, on the other hand, student drop-out immediately influences its financial organization, possibly impacting on the teachers. Hence, the findings of lower intensity and frequency of moral distress in nursing students at the private university may be related to their work organization, similar to that of other private companies, where institutional profit becomes the driver of actions. 28
In this sense, teachers in the private universities, without tenure, are mostly hired on an hourly basis (hours/class) or with limited contracts, which turns them into temporary service providers, who are permanently exposed and more vulnerable employment instability. Furthermore, teachers and their employment are vulnerable to students’ complaints, as education is understood as a good the client/student buys and the teacher/worker needs to build on client satisfaction. 28
Regardless of whether the teaching organization is public or private, the university environment strives for active subjects who participate in their own training process, and, therefore, their demands need to be heard and discussed. Thus, students will be able to intervene in their reality, in an inclusive and democratic way, exercising mutual respect and dialog, so that there is no room for impositions or limitations in their constitution as autonomous, ethical professionals who are capable of transforming the educational and health context, 27 directly leading to possible postures of coping, also with moral distress.
In addition, the construct C6: Professional choice, constituted by indecision about the chosen profession and feeling of professional devaluation, presented more significant means moral distress levels at federal universities. These data may be related to the free vacancies in higher education, unlike the private university, which financially charges the students and usually their families, contributing to the professional choice being made with greater knowledge about the selected course, possibly less impulsively, but more mature and shared.
In this context, an investigation involving nursing students at two, public and private, educational institutions, compared the socioeconomic profile and the factors that interfere in the professional option, noting that the expanding nursing work market and the opportunity for a better remuneration attract the students of the private institution. On the other hand, the students at public institutions showed a lack of knowledge on the profession and the field of action of the nurse, associating the image of the professional with the person who helps the neighbor. 29
Concerning the construct with the highest average in the study as a determinant of moral distress among undergraduate nursing students, C1: Commitment of the ethical dimension of user care was identified, which demonstrates the students’ concern with questions regarding ethical and moral care. These data legitimize and strengthen the need to guide students about patient advocacy, in order to contribute to raise their awareness and participation in coping with situations that can generate moral distress, thus arousing active attitudes of patient advocacy, who will come to take care of themselves, their fellow students, and the profession chosen. 8,30
Relationship between sociodemographic characteristics and moral distress
The analysis of moral distress and its relationship with sociodemographic and academic variables in undergraduate nursing students from different universities in Brazil showed significant correlations of moral distress in the construct C6: Professional choice, in students under 25 years of age, and in students who failed one or more times. These data may be associated to a professional choice that is still fragile, a fact that motivates further questions and insecurities about the course chosen, and even on their continuation.
Similar to the findings of this study, it has already been verified that different factors can influence the professional choice process, some of them related to immaturity, the belief that health courses are similar, and the option for less popular undergraduate courses in the same area. These factors are common in nursing and may give rise to false expectations regarding the undergraduate course chosen; thus, by not being reached, they contribute to the appearance of feelings of disappointment, discouragement, loss of enthusiasm and frustration, and imbricated in feelings of non-valuation of the profession, which constitute moral distress.
In view of this context, the students can move away from the classroom, present teacher/peer interaction difficulties and, consequently, compromise their academic performance. Accordingly, the students who failed one or more times in this study had higher levels of moral distress, also associated with the construct C3: Authoritarian teaching practices, supporting the premise that failure may be associated with the perception of an authoritarian teaching posture. This fact emphasizes the teacher’s exercise of power in the student’s training process, which may facilitate, favor, or even hinder and interfere with learning by reducing students’ interest in the pedagogical process. 27
Thus, it is necessary not only that nursing students have contact, from the initial grades, with the reality of nurses’ work but also that society, in a broader way, is better informed in order to know well and recognize the potentials and possibilities of nursing practice, in its most diverse working scenarios. 31 Teachers also need to perform professional behaviors in keeping with morality and ethics13 because through good example and support, nursing students can successfully build their professional future. 32
Nursing students enrolled in the final series identified significant moral distress in general, in two statistical tests, the t-test for independent samples and ANOVA (Duncan test). Regarding the constructs that generated the highest moral distress rates, among the students in the final semesters, in the ANOVA (Duncan test), we identified C1: Commitment of the ethical dimension of user care and C2: Improper institutional conditions to teach user care. Similarly, the t-test for independent samples also showed significant levels of moral distress in three other constructs: C3: Authoritarian teaching practices; C4: Lack of competence of the teacher; and C5: Disrespect for the ethical dimension of vocational training.
According to the literature, there is a direct correlation between the student’s semester and moral distress levels. In a study of 160 nursing students, only 29% of second-year students scored higher than zero, while 95% of the students in more advanced grades scored higher than zero for moral distress levels. Likewise, 10 students, who were heading toward the end of the course, more often reported moral problems, unlike those in the early stages. 8
As from the fifth semester, students are more experienced in the set of theoretical and practical academic activities, which gives them a better view of the educational and health context, allowing them to identify a greater number of ethical and morally conflicting situations in the different academic scenarios. Also, in this study, the results show that, as from the seventh semester, the students began to raise further questions on the practices of the nursing team they interact with, the lack of material resources and the right of the patient to high-quality healthcare.
In this context, academic education plays a fundamental role in addressing issues related to moral distress. To this end, various strategies have been highlighted, such as individual and group dialog and reflective writing on moral and ethical issues. Despite acknowledging that some situations generating moral distress may not be easily solved, the positive impact of a discussion forum is proven, especially by recognizing students’ concerns as valid.8
What the variable prior training is concerned, students who were auxiliary nurses/technicians presented lower levels of general moral distress and in two constructs, C1: Commitment to the ethical dimension of user care and C3: Authoritarian teaching practices, compared to students with other educational backgrounds. In this sense, several factors may be associated with the decreased perception of moral distress, among which one can cite self-defense and compliance with what was established due to prior professional experience, factors that may constitute a seeming trivialization of ethical and moral problems.
According to studies, 23 –26 these factors seem to confirm a certain professional acculturation when, after repeated exposures to negative examples, related to institutional health problems and their hierarchical relationships, they start to directly influence individuals and their moral sensitivity, to the extent of seeing them as an incorrigible part of the health and education system, or not even acknowledging them as moral problems. Therefore, it is important to note that the absence of moral distress does not necessarily indicate that ethical problems do not exist in a specific environment, but rather that their impact on individuals may be reduced due to their level of moral sensitivity.
Thus, due to the complexity of the global health environment, moral and ethical challenges will remain intrinsic to the academic training environment in nursing. Emphasis is placed on the need for nursing students to be properly prepared to confront moral distress, as opposed to educational demands that pressure them too much, preventing them from learning how to constructively manage their decisions in view of situations that can somehow generate moral distress. Thus, teaching students effective attitudes to respond to distressing situations and processing their concerns is the responsibility of university institutions and teachers. 13
Limitations
As a limitation of this study, it is relevant to highlight that ESMEE was prepared and applied for the first time in the surveyed sample; accordingly, there were no previous data from this scale for comparison.
The use of convenience sampling may be considered a limitation of this study 20 in view of the possibility of a low response rate. However, this choice was justified by the fact that it provided a representative sample of nursing students from the three universities surveyed. This study was carried out in the sociocultural context of the extreme south of Brazil, and therefore, caution is needed for the generalization of the findings to nursing students in other sociocultural contexts.
Conclusion
Correlations, although considered hardly significant, could be verified between moral distress and the profile of undergraduate nursing students. In this sense, undergraduate nursing students from three Brazilian universities reported a higher mean moral distress in the construct C2: Improper institutional conditions to teach user care. Also, students who reported higher levels of moral distress had the following demographic and academic characteristics: being enrolled in the final course terms, no background as an auxiliary nurse/nursing technician, and being enrolled in a federal university.
Regarding the constructs that can generate moral distress in the academic environment, the commitment of the ethical dimension of user care stood out among students in the final terms of the undergraduate nursing program without a degree as an auxiliary nurse/nursing technician.
A significant relation was also found between the construct of authoritarian teaching practices and students who failed one or more times. A stronger correlation was found among students in the final semesters and from federal universities for improper institutional conditions to teach user care and lack of competence of the teacher. In the construct C5: Disrespect for the ethical dimension of vocational training, the students in the final terms of the undergraduate nursing program evidenced higher mean moral distress; as well as in the construct C6: Professional choice for students under 25 who failed one or more times and were enrolled in federal universities.
Implications and further research
In this context, it can be concluded that, when problematizing situations that generate moral distress in the academic context, there is concern with the future of the nursing profession, as nursing students represent this future. Thus, attention, valuation, and discussion of ethical and moral problems and conflicts, perceived during the undergraduate academic period, offer an opportunity to create alternatives for necessary changes, such as coping with moral distress, consistent with a critical and active role for the nursing profession, committed to an educational and health reality guided by respect for the lives of users, students, and professionals.
Footnotes
Acknowledgements
The authors sincerely thank the directors and coordinators of the undergraduate nursing courses and all nursing students who participated in this study, whose contribution and interest made the realization of this study possible.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted under the research project “Patient advocacy and coping in nursing: possibilities of exercising power through experiences of moral distress,” financed by Universal Call 14/2012 (case 474761/2012-6). This research was also supported by a PhD grant awarded by the Foundation for Research Support of the State of Rio Grande do Sul (Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul—FAPERGS), from 2013 to 2016.