
Abstract
Background:
Maintaining patient dignity is an important aspect of nursing care. No instrument is currently available to measure nurses’ behaviours for maintaining patient dignity in clinical care.
Objectives:
To develop and test an instrument to measure activities nurses perform to maintain patient dignity in clinical care settings, guided by the literature and face-to-face interviews.
Research design:
A quantitative cross-sectional descriptive survey collected data from the developed scale, which was analysed by descriptive statistics and factor analysis.
Participants and research context:
Convenience samples of nurses participated in the interviews (n = 40) and examined face validity of the scale (n = 20). A purposive sample of 610 nurses was recruited from four regional hospitals in the northern, southern and eastern areas of Taiwan to test the developed scale.
Ethical considerations:
Research was approved by the Institutional Review Board of the study hospital. Information about the study was provided to nurses and those willing to participate provided written informed consent prior to data collection.
Findings:
The 36-item Dignity in Care Scale for Nurses had acceptable content and face validity. Factor analysis identified six factors necessary for maintaining dignity of patient care: communication skills, confidentiality of patient information, prompt response to patient needs, respect for patient’s autonomy, providing a safe environment and protecting the patient’s well-being. The reliability coefficient for the total scale was 0.93; alpha coefficients for the subscales ranged from 0.70 to 0.94.
Discussion:
The Dignity in Care Scale for Nurses was demonstrated to be a reliable and valid tool for assessing how nurses maintain dignity in care for patients in the clinical setting. The questionnaire can be used to provide feedback to nurses regarding patient dignity.
Conclusion:
Data gained from this instrument could be used to design nursing education programmes to help nurses enhance their abilities for maintaining patient dignity in clinical practice.
Introduction
Dignity was recognised as a human right by the World Health Organisation (WHO) in the Universal Declaration of Human Rights in 1948. 1 The term dignity is a multidimensional construct associated with a person’s worth and includes concepts such as respect, value and recognition. 1 Patient dignity is an important issue in healthcare systems 2,3 and a core value in nursing care. Healthcare in the absence of providing dignity can adversely influence patients’ recovery. 4 –7
Good nursing care is considered dignity-enhancing care; maintaining dignity of care promotes emotional comfort, which enhances recovery. 7 –9 Respect for basic human rights and maintenance of patient dignity has been promoted by nursing organisations in Western countries 10 –12 and in Taiwan. 13 Maintaining patient dignity includes honouring a patient’s individuality, allowing them to maintain autonomy in making medical decisions, acknowledging religious and cultural values, treating patients equally regardless of economic status and respecting the patient’s lifestyle, 10 –13 which is fostered by the healthcare team and nurse–patient interactions. 14,15 Respect for dignity is central to the International Council of Nursing Code, which states, ‘Inherent in nursing is respect for human rights, including cultural rights, the right to life and choice, to dignity and to be treated with respect’. 16 Respect incorporated religious and cultural beliefs, and informed consent. 17
The healthcare literature on dignity has addressed the meaning and implications of dignity in multidisciplinary healthcare fields for nurse and patient populations, 18 –21 which is primarily descriptive and focuses on the experiences between healthcare providers and patients. 22 Several qualitative studies have shown that maintaining patient dignity requires protecting patient privacy, respecting the patient and providing patient autonomy; this has been demonstrated in Western countries including the United States, 23,24 the United Kingdom, 25 –28 Canada, 29 Finland 20,30 and other European countries 31 –34 as well as Asian countries. 14,17,35,36 Dignified care for patients also includes emotional support, truthfulness, 6,28,37,38 communication, avoidance of unnecessary body exposure and maintaining patient privacy. Privacy involved dignity of care, and privacy of the body and personal space 39 –41 A qualitative study of patients’ perspectives in Taiwan identified six characteristics that maintained dignity of care for hospitalised patients: a sense of control and autonomy, being respected as a person, avoidance of body exposure, feeling cared for by the nursing staff, confidentiality of disease information and a prompt response to their needs. 35
Purpose of the study
Patient dignity is maintained by the nursing care provided. Therefore, how nurses provide care can influence a patient’s perception of receiving dignified care. Previous studies in Western and Asian countries focused on qualitative interview data to determine how nurses maintain patient dignity. No studies have quantitatively assessed the activities nurses perform to maintain patient dignity in clinical care settings. Therefore, the purpose of this study was to construct and test an evidence-based survey instrument of nursing behaviours associated with maintaining patient dignity.
Research methods
Study design
Instrument development with testing and a cross-sectional descriptive quantitative survey was conducted.
Instrument development
We developed a Dignity in Care Scale for Nurses (DISCN) to measure how nurses maintain patient dignity in clinical care settings. Development of the DISCN was conducted in three phases: (1) item generation and scale development, (2) assessment of content and face validity and (3) validity and reliability of the instrument.
Participants and setting
A convenience sample of 40 nurses from medical and surgical wards was recruited to participate in face-to-face interviews for item generation of the scale. A second convenience sample of 20 clinical nurses was recruited for examining the face validity of the scale. The final version of DISCN was tested with nurses recruited by purposive sampling from four regional hospitals in the northern, southern and eastern areas of Taiwan. Inclusion criteria for this group of nurses were: (1) working for at least 3 months after internship in internal medicine, surgery, an emergency room or an intensive care unit, (2) at least 20 years of age, (3) able to complete the self-administered questionnaires in Chinese or Taiwanese and (4) willing to sign an informed consent prior to participation. The minimum sample size for factor analysis should be at least 5–10 times the number of items of the scale or greater. 42 Our initial scale had 43 items; therefore, the minimum sample size was determined to be between 215 and 430.
Item generation and scale development
Item generation of the dignity in care construct was based on previous qualitative research findings, 17,35 related references 6,25,39 and individual face-to-face interviews with 40 clinical nurses regarding their views of how nurses provide dignity of care to patients in clinical practice. Audiotaped interviews were conducted as described previously. 17 Briefly, nurses were asked two questions: (1) How do you provide dignified care in clinical practice? and (2) What is your view of dignified care? Interview data were transcribed verbatim and analysed by content analysis. The interview data showed nurses considered dignity of care required respecting the patient, protecting patient information, providing emotional support and preventing exposure of the patient’s body. After reviewing the literature and analysis of the interview data, we created 43 items, which were statements regarding how dignity of patient care is maintained in a clinical setting. The items of the DISCN were scored on a 5-point Likert-type scale (1 = never, 2 = rarely, 3 = sometimes, 4 = usually, 5 = always). Higher scores indicate a higher frequency of providing dignity care
Content and face validity
The preliminary 43-item DISCN was examined for content validity by a panel of five experts: three clinical nurses with extensive experience in the field of ethics and nursing education, and two experienced clinical nurses. The experts were asked to rate each item of the DICSN on a 4-point Likert-type scale on the basis of relevance to providing dignity in care to the associated category: 1 = not relevant, 2 = somewhat relevant, 3 = relevant, but needs minor changes and 4 = very relevant. The content validity index for the items of the scale (I-CVI) was computed by determining the proportion of items rated 3 or 4 by all the experts. 42 Items were selected if the average score was 3 points higher. Items rated 3 were revised based on comments or suggestions from the experts. The readability of the 43 items of the preliminary DISCN was examined with face validity. The convenience sample of 20 clinical nurses completed the 43-item DISCN and evaluated the items for clarity.
Validity and reliability of the instrument
Construct validity of the 43 items was determined with exploratory factor analysis (EFA). The reliability of the DICSN was estimated by the internal consistency of each subscale, which was measured with Cronbach’s alpha coefficient. Test–retest reliability was evaluated with 60 randomly selected participants who were asked to answer the survey a second time, 4 weeks later.
Data collection
Data for the DISCN were collected between April and December 2013. A packet containing a cover letter restating the purpose of the study, the DISCN, and a demographic data questionnaire, anonymised with a coded number, was distributed by mail to 642 participants. Participants were instructed to return the completed packet by mail in the stamped envelope provided.
Data analysis
Data were analysed with SPSS 18.0 software (SPSS, Inc., Chicago, IL). Participant characteristics were analysed with descriptive statistics. The DICSN was evaluated with tests of reliability and validity. Statistical methods included frequency, mean and standard deviation (SD). Construct validity was assessed via EFA. Principal component factor analysis was performed using varimax rotation with Kaiser normalisation of the scale. Factors were selected based on eigenvalues > 1 and not <5% variance accounted for by each factor. 43,44 Internal consistency reliability was assessed by Cronbach’s α coefficient. The 4-week test–retest reliability was assessed by calculating the intraclass correlation coefficient (ICC); p values < 0.05 were considered significant.
Research ethics
Before data collection, the study was approved by the hospital’s Institutional Review Board (IRB; No-11-07-013). The first author explained the purpose and significance of the study to all nurses, as well as their right to withdraw at any time and for any reason, without any impact on their job and that the data would be treated confidentially. Nurses who agreed to participate joined the study after signing informed consent.
Results
Participant characteristics
A total of 610 clinical nurses returned completed data packets for a response rate of 95%. The demographic characteristics of the participants are shown in Table 1. The mean age was 29.8 years (SD = 6.53, range = 20–56) and most were female (n = 608, 99.7%), not married (n = 395, 64.8%), had at least a college degree (n = 304, 50.0%) and had achieved a level on the nursing ladder of N2 (certified nursing leader) or higher (n = 387, 87.2%). The mean length of nursing experience was 6.86 years of work (SD = 6.04, range = 0.4–34). None of the participants had taken a course on dignity in care in the clinical setting.
Demographic characteristics of nurse participants (N = 610).
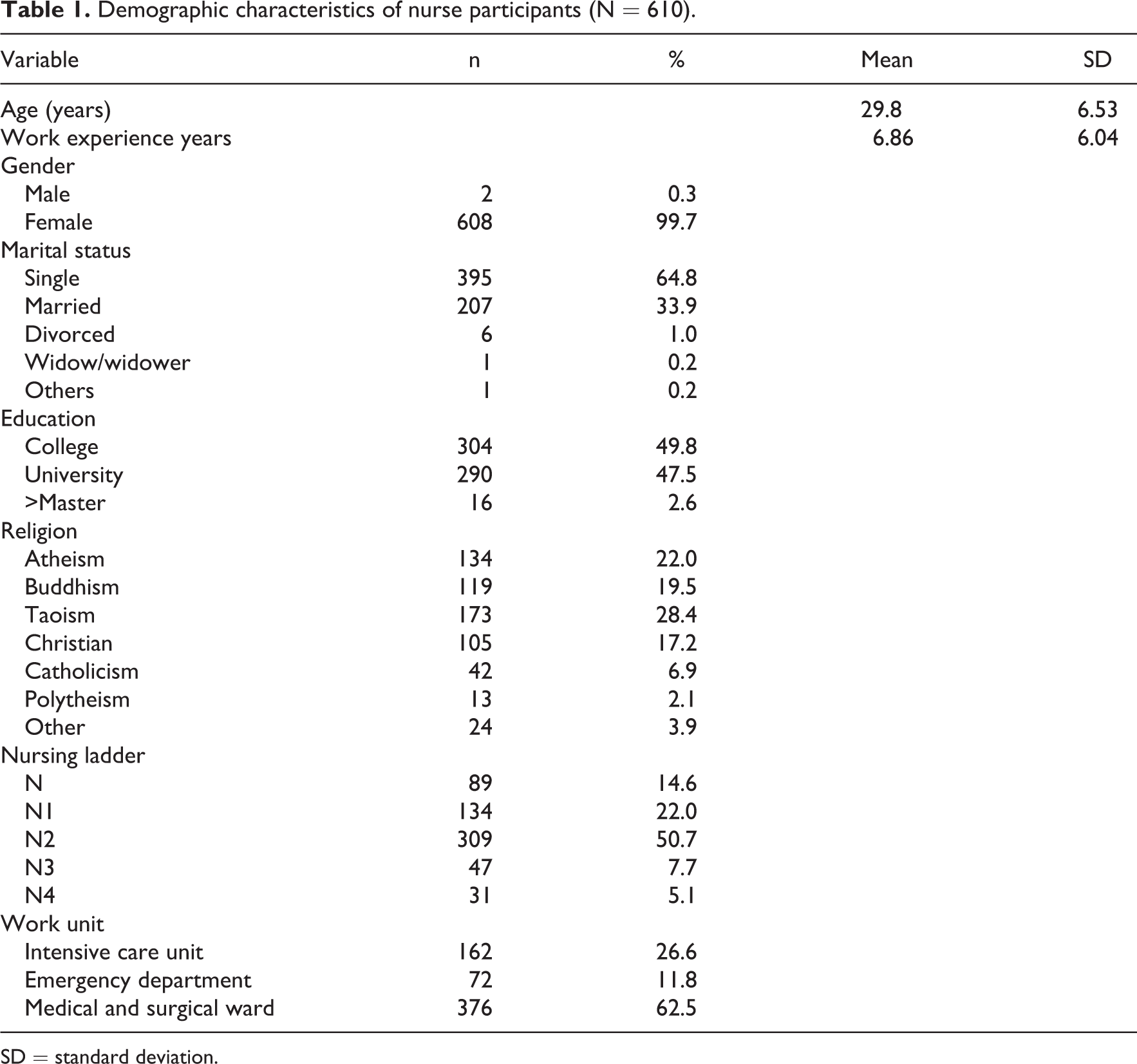
SD = standard deviation.
Validity
Content validity and face validity
Analysis of the 43 items of the initial DISCN evaluated by the panel of five experts resulted in an I-CVI of 0.97, which is above the recommended CVI (0.80) for a new instrument. 43 On the basis of feedback from the panel, some editorial changes were made regarding content. Face validity of the 43-item DISCN, was determined to be acceptable based on the ability of the 20 clinical nurses to read and understand all 43 items, and agreement with the statements regarding how nurses maintain patient dignity in clinical practice; therefore, all 43 items were retained. Participants completed the questionnaire in 10–15 min, and no difficulties were reported.
Construct validity
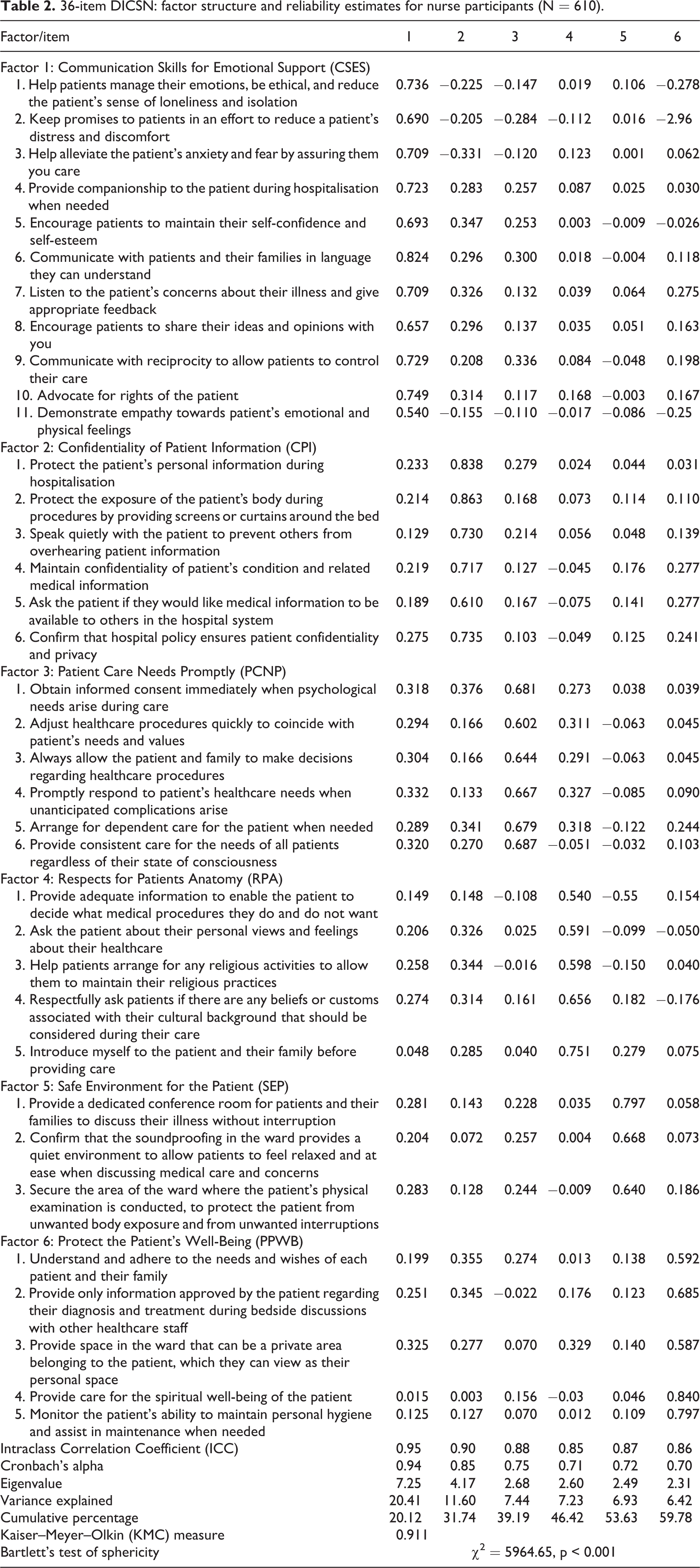
Prior to conducting EFA, Kaiser–Meyer–Olkin (KMO) and Bartlett’s test of sphericity was used to measure the sampling adequacy and variance, respectively. The KMO value of the initial DISCN was 0.945, and Bartlett’s sphericity was <0.001 (χ2 = 14225.386, p < 0.001), indicating factor analysis was appropriate. 43 Factors were selected based on an eigenvalue > 1. EFA yielded a nine-factor solution, which explained 63.23% of the total variance. To define the composition of the nine factors more efficiently, items that did not load strongly or cleanly on a single factor were eliminated. According to the scree plot, the slope of the curve became emergent at the sixth point, and factors 7–9 only contributed 9.2% of the accumulated variance. Items were kept if they loaded on a single factor >0.50; seven items were deleted because they did not load strongly. 44 Deletion of the 7 items resulted in 36 items. The construct validity of this 36-item scale (see Appendix 1) was tested by principal axis factor analysis with varimax rotation; the final six-factor solution accounted for 59.78% of the variance. We labelled the six factors as follows: Factor 1: offer communication skills for emotional support (CSES, 11 items); Factor 2: ensure confidentiality of patient information (CPI, 6 items); Factor 3: provide patient care needs promptly (PCNP, 6 items); Factor 4: respect patient’s autonomy (RPA, 5 items); Factor 5: provide a safe environment for the patient (SEP, 3 items) and Factor 6: protect patient privacy and well-being (PPWB, 5 items). Table 2 shows the factor structure of the DICSN, while Table 3 shows the scores of the subscales of the DICSN.
36-item DICSN: factor structure and reliability estimates for nurse participants (N = 610).
Scores for the subscales of the Dignity in Care Scale for Nurses (DICSN): range = 1–5.
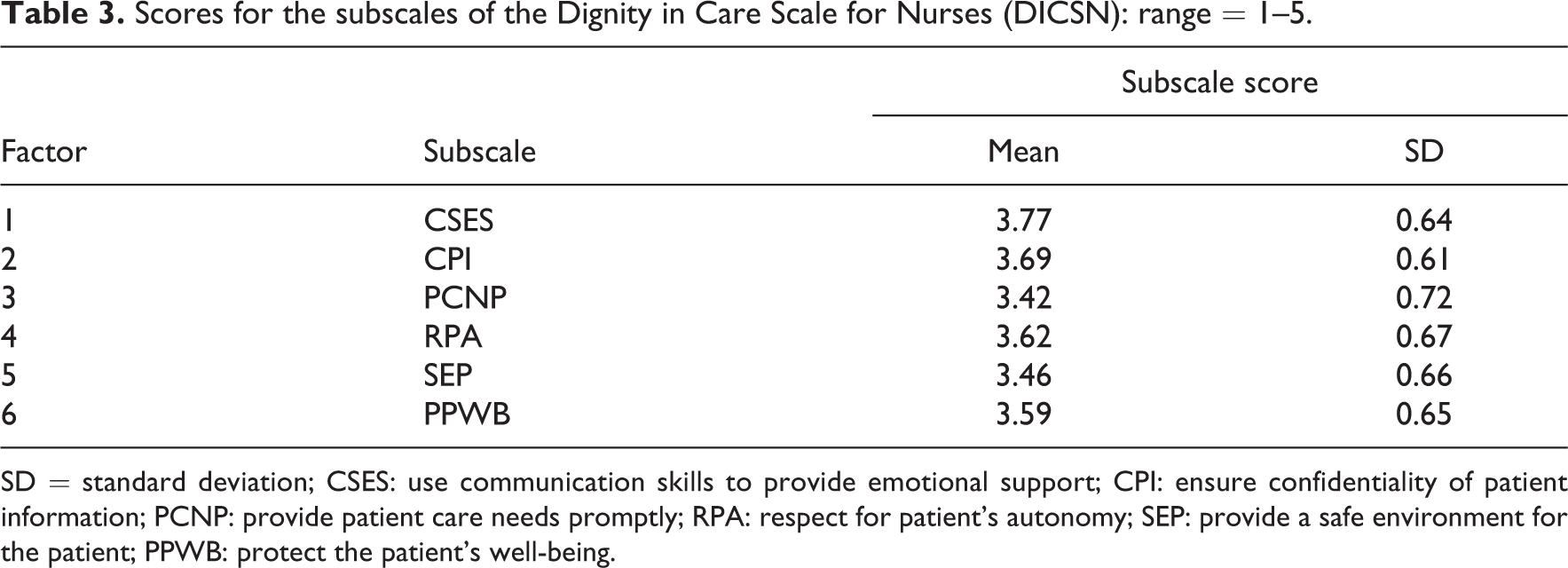
SD = standard deviation; CSES: use communication skills to provide emotional support; CPI: ensure confidentiality of patient information; PCNP: provide patient care needs promptly; RPA: respect for patient’s autonomy; SEP: provide a safe environment for the patient; PPWB: protect the patient’s well-being.
Reliability
Internal consistency reliability
Cronbach’s alpha for the final 36-item instrument was found to have high internal consistency, with an alpha coefficient of 0.94 for the total questionnaire. Alpha coefficients for the six factors ranged from 0.70 to 0.94 (Table 2). All alpha coefficients for the DICSN subscales and the total scale were >0.7, indicating adequate internal consistency of the total scale to measure the construct of interest. 45 In items of variance explained by the subscales, emotional support explained the greatest amount (20.14%) and SEP explained the least (6.42%).
Test–retest reliability
The 4-week test–retest reliability was assessed by calculating the ICC. Of the 610 participants, 60 were randomly selected and asked to answer the survey a second time, 4 weeks later. The ICC of the global DICSN was 0.95; the ICC for each subscale ranged from 0.85 to 0.95 (Table 2).
Scoring
The 36 items of the final DISCN were scored with a 5-point Likert-type scale ranging from 1 to 5: 1 = never, 2 = occasionally, 3 = often, 4 = most of the time, 5 = always. The score for the instrument ranged from 36 to 175. The subscales scores were determined by dividing the total item scores for the subscale by the number of items; therefore, all subscale scores ranged from 1 to 5. Higher scores indicated a higher frequency of performing tasks to maintain patient dignity in a clinical setting. The mean total score for the 610 participants responding to the six-factor DICSN was 126.9 (SD = 18.5), indicating that frequency of performing tasks associated with maintaining dignity of care was moderate. The highest mean subscale score of the six subscales was CSES (3.77; SD = 0.64), indicating communicating with patients in ways that offered emotional support was the most frequent method of maintaining dignity in patient care. The lowest mean subscale score was promptness of care (PCPN, 3.42; SD = 0.67).
Discussion
This study developed and validated a new instrument, the DICSN for nurses to measure behaviours clinical nurses employ to maintain patient dignity. The DICSN had acceptable reliability and validity, and required only 10–15 min to complete. The final six-factor solution accounted for 59.78% of the variance. The six subscales describe aspects of nurse–patient interactions that maintain patient dignity: CSES, CPI, PCPN, RPA, SEP and PPWB. These findings are similar to qualitative studies of how nurses preserve dignity in care. 27,37,39
The mean subscale score for CSES was the highest of the six subscales of the DISCN for the participants in our study. Offering emotional support as a means of providing dignity in care is supported by interview data from Lin and Tsai, 17 who found nurses considered emotional care important for maintaining patient dignity. Patients have reported psychological support and comfort from nurses is perceived as a behaviour that maintains patient dignity; supportive communication allows patients to feel comfortable and express their emotions. 32,35,41 The finding that CSES was the highest subscale score might suggest the clinical nurses in our study considered encouraging and allowing patients to express their emotional and physical concerns an important aspect of maintaining dignity of care.
Ensuring CPI was the second highest mean score for the participants on the DISCN. Qualitative studies have also reported protecting the patients’ personal and medical information and unwanted body exposure is important for maintaining dignity in care. 27,35,39,40,46 However, these forms of confidentiality are more challenging in hospital environments in which patients are cared for in a multi-patient ward facility. 27 The nurses’ mean score for CPI indicated most participants made an effort to discuss medical information out of hearing of other patients or visitors, protected the patient from body exposure and confirmed the hospital policy regarding patient confidentiality. Spatial privacy problems are encountered in many hospital rooms in Taiwan. Under Taiwan’s National Health Insurance, three- to five-person hospital rooms are free of charge; because of economic constraints, most patients select these no-pay beds. Hence, hospital rooms should be designed in a manner that confidentiality of patient information can easily be maintained during nursing interventions. This can be accomplished by using a low voice to prevent others from overhearing conversations, as well as providing spatial privacy. 6
The mean scores for maintaining dignity in care by RPA and PPWB were similar. When a hospitalised patient feels in control of their care and can make decisions for themselves, they are more likely to have a sense of well-being and less likely to feel a loss of dignity. 27 Respecting patients’ individual needs included understanding and accommodating not only medical instructions, but also the patient’s beliefs and culture. Respecting a patient’s autonomy not only has the advantage of providing patients with dignity, but also allowing patients to feel more comfortable about giving informed consent. 8,17,34
The mean subscale scores for providing an SEP and PCNP were also similar. A safe environment ensures the hospital setting provides comfort. Previous studies have demonstrated the importance of helping patients feel relaxed, valued and safe, which requires providing patients with personal space, protection from unwanted body exposure, and control over who has access to their medical information and information regarding illness. 6,47 Protecting the patient from unwanted exposure of the body is particularly difficult in Taiwan, where nurses are under constant pressure to mix genders in wards due to bed shortages, resulting in patients experiencing a loss of dignity. Providing patient care promptly is important when patients are critically ill and rely on nurses to meet their care. There is a strong relationship between prompt nursing care and a patient’s experience of dignity during hospitalisation. 35,36 Therefore, this finding may indicate that nurses need to be made aware that PCPN also has an impact on maintaining dignity of care.
Limitations
This study had some limitations. First, testing of the DISCN was conducted with participants selected by purposive sampling and most were from medical, surgical and critical care units. This might limit the generalisability of the findings to other clinical settings. Second, although the item generation included data from qualitative studies conducted in both Western and Asian countries, items were also the result of the interview data collected from nurses in Taiwan. Therefore, validation of the scale with clinical nurses in other countries will be required to determine cross-cultural generalisability of the DISCN.
Conclusion
The newly developed DICSN is a comprehensive measurement tool for how nurses maintain dignity in care for hospitalised patients. The scale provides a quantitative assessment of six elements: communication skills, confidentiality of patient information, prompt response to patient needs, and respect for patient’s autonomy, providing a safe environment and protecting privacy of care. The instrument has acceptable internal consistency, reliability, and good content and construct validity (Figure 1). Application of the DICSN instrument could expand our understanding of how nursing staff maintain patient dignity. Our findings contribute to the literature regarding dignity in care, which could improve clinical care for patients by providing feedback to nurses and hospital administrators. Nursing programmes could use the DICSN for in-service nursing programmes to enhance the ability of nurses to provide patients with dignity in care. The strength of this study is its focus on positive elements that can be implemented by nurses to maintain patient dignity.
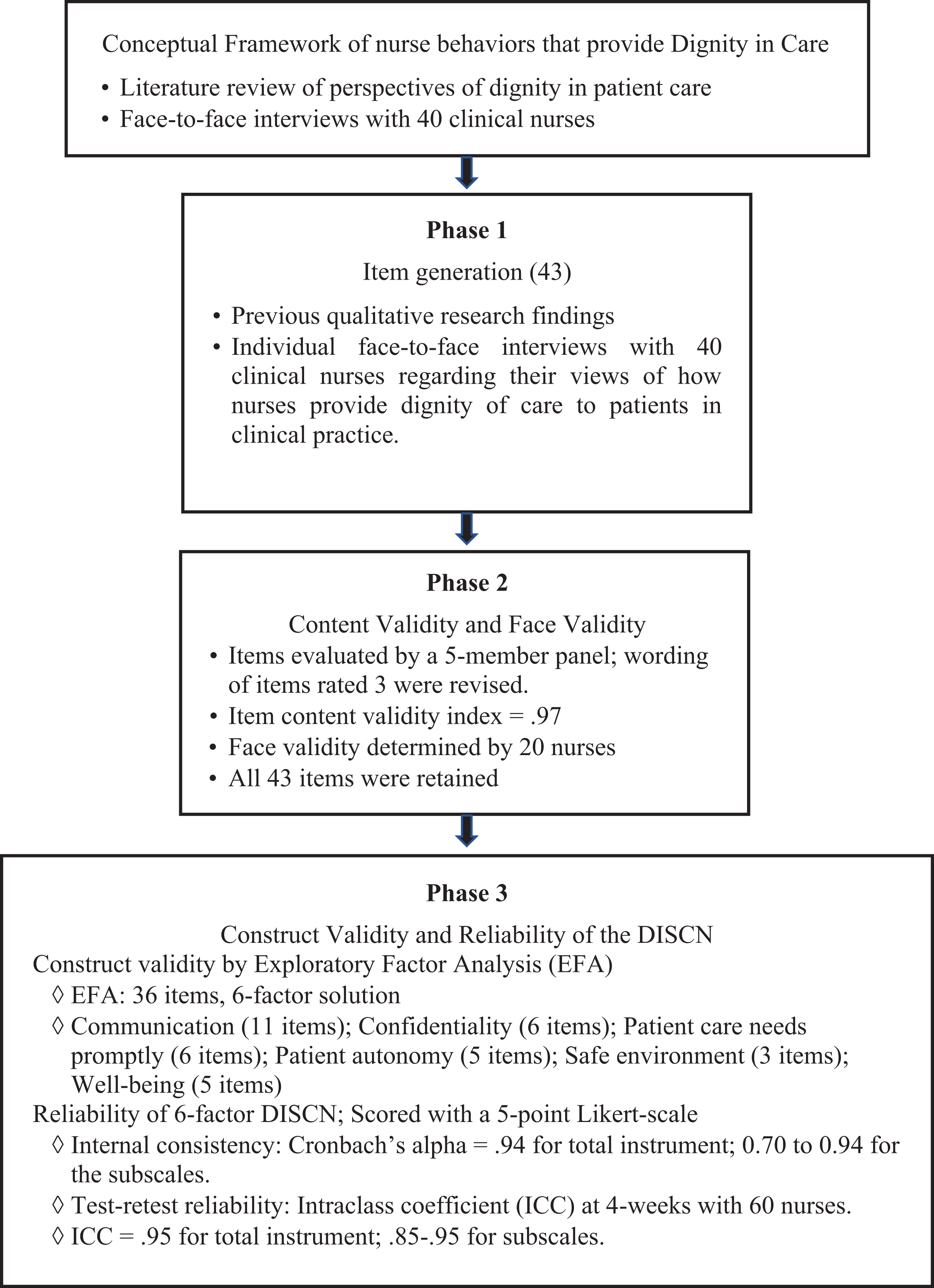
Development of the Dignity in Care Scale for Nurses (DISCN).
Footnotes
Acknowledgements
We would like to thank all the participants who gave their time to this study.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by the Mennonite Christian Hospital, Taiwan.
Ethical approval
This study was approved by the institutional review board of the ethical committee of Mennonite Christian Hospital (IRB 98-1452B).