
Abstract
Background
Patient dignity is sometimes neglected in intensive care unit (ICU) settings, which may potentially cause psychological harm to critically ill patients. However, no instrument has been specifically developed to evaluate the behaviors of dignified care among critical care nurses.
Aim
This study aimed to develop and evaluate ICU Dignified Care Questionnaire (IDCQ) for measurement of self-assessed dignity-conserving behaviors of critical care nurses during care.
Methods
The instrument was developed in 3 phases. Phase 1: item generation; phase 2: a two-round Delphi survey and a readability pilot study; phase 3: cross-sectional survey with model estimation. The questionnaire was evaluated by item analysis, exploratory and confirmatory factor analysis, assessment of internal consistency reliability, and test-retest reliability. The investigation was conducted using a convenience sample of 392 critical care nurses from 6 cities in Zhejiang Province, China, of which 30 participated in the test-retest reliability survey 2 weeks later.
Ethical considerations
The study was approved by ethics committee. All participants provided written informed consent before the survey. The questionnaire survey was anonymous.
Results
The results showed acceptable reliability and validity of the IDCQ. The 17-item final version questionnaire was divided into 2 dimensions: absolute dignity and relative dignity. These two factors accounted for 62.804% of the total variance, and model fitting results were acceptable. The Cronbach’s alpha coefficient of the questionnaire was 0.94, and the test-retest intraclass correlation coefficient (ICC) was 0.88 after 2 weeks.
Conclusions
This study developed a brief and reliable instrument (IDCQ) to assess dignified care in ICU nursing. It can help critical care nurses identify their behaviors in maintaining patient dignity and discover their deficiencies. It may also serve as a clinical nursing management tool to help reduce patient disrespect experience in ICU.
Introduction
Dignity is an abstract, complex, and meaningful concept which is of immense relevance to the human experience. According to the literature, the attributes of dignity include personhood (intrinsic value), sociability (situation-dependent), respect, and autonomy.1–5
Critically ill patients are immensely vulnerable and need a certain level of respect for their dignity. Studies6–8 have suggested that loss of dignity is a common phenomenon among intensive care unit (ICU) patients. In the ICU, patients with life-threatening illnesses are usually unable to speak, are physically restrained, passively accept various manipulations, are often stripped naked, accompanied by bedside alarms, and are separated from their families. 9 “Loss of dignity” in this situation is regarded as intrinsic emotional harm, which may lead to anxiety, depression, or post-traumatic stress disorder syndrome in ICU survivors; 10 in addition, dying ICU patients suffer severely beyond physical pain. 11
Nurses play an essential role in promoting the sense of dignity among patients. 12 As a humanistic discipline, the ethical nature of nursing is to provide care for human vulnerability and to preserve and promote patient dignity as much as possible. 13 According to Gazarian et al., 14 positive nurse-patient interactions based on care and compassion represent an excellent way to maintain patient dignity. In the ICU environment, maintaining patient dignity includes understanding and caring for the patient as a unique individual, making an effort to communicate with all patients, protecting their vulnerability and privacy, listening to them, speaking up for them, and empowering them with choices or control.9,15–17
However, the current status of critical care nurses in preserving patient dignity is not well characterized. There are only two instruments related to maintaining the dignity of ICU patients, that is, CORE-ICU 18 and DOC. 19 The CORE-ICU 18 is a tool for evaluating clinicians’ perspectives of respectful treatment in the ICU. The scale consists of 21 items encompassing 3 dimensions: overall respect, respectful behaviors, disrespectful behaviors. This scale was not designed for nurses specifically. Besides, in Asian culture, individuals are more likely to feel embarrassed and ashamed to report their behaviors that cause disrespect to others. Therefore, Asian clinicians may be more likely to hide their actual behaviors when asked about the dimension of disrespectful behaviors. As reported by the developers 18 of this scale, Asian respondents reported greater respect for patients than respondents of other races. Thus, this instrument may not be suitable for universal use. Carrese et al. 19 developed the DOC to assess the level of respect and dignity accorded to patients in the ICU and their families. The DOC is a direct observation checklist with 10 items, consisting of 2 subscales: clinician behavior and clinician demeanor. The DOC can avoid the influence of self-reported bias to some extent. However, the existence of an observer is liable to induce a conscious change in the behavior of the clinicians. 19 Moreover, DOC requires a skilled observer and the process is time-consuming. Thus, it is not suitable as a conventional screening scale. For these reasons, this study aimed to develop an instrument to provide a more concrete measure of how critical care nurses provide care with respect and dignity. This novel questionnaire is intended for use as a complementary tool along with the currently used instruments for assessing the behaviors of critical care nurses in dignified care.
Aim
The aim of this study was to develop the ICU Dignified Care Questionnaire (IDCQ) and to assess its reliability and validity in order to provide a basis for evaluating the behaviors of critical care nurses in preserving patient dignity.
Methods
Study design
The development of this questionnaire was divided into 3 phases (Figure 1). Phase 1: development of the preliminary version (item generation); Phase 2: development of the test version (two-round Delphi survey and a readability pilot study); Phase 3: development of the final version (a cross-sectional survey and model estimation). The process of instrument development.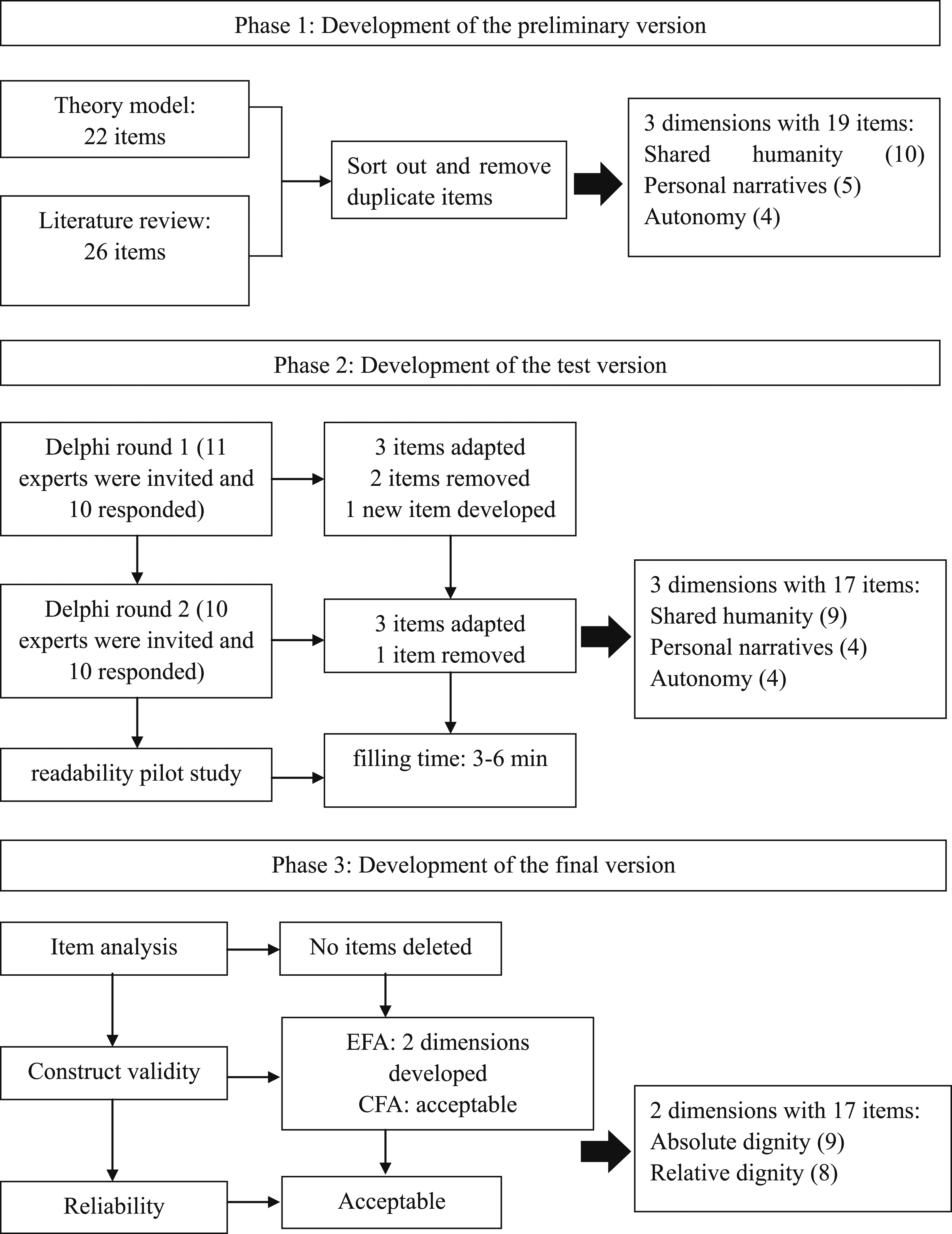
Phase 1: Development of the preliminary version
Items used in the initial version of the instrument were sourced from a conceptual model and a systematic review of relevant literature. The conceptual model, proposed by Dr Henry et al. 20 from Johns Hopkins University, is mainly suitable for adult patients in the ICU. According to the model, the dignity of ICU patients emanates from 3 aspects, that is, shared humanity, personal narrative, and autonomy. The concept of shared humanity indicates that every patient should be respected equally; personal narrative means that nurses should regard each patient as a unique individual; and autonomy emphasizes that nurses should safeguard the autonomy of patients and their decision-making agents during medical care. The above 3 sources of dignity are based on shared humanity and are sometimes interactive. Based on the model, we initially generated some items and structured the questionnaire into 3 dimensions: autonomy, personal narrative, and shared humanity.
To enrich the item pool, we searched the following databases for articles published as of July 2020 to identify more items about critical care nurses’ behaviors in preserving dignity: Cochrane Library, Joanna Briggs Institute EBP Database, PubMed, Embase, PsycINFO, CINAHL, Web of Science, China National Knowledge Infrastructure (CNKI), Wanfang Data Chinese database, Chinese Chongqing VIP Information, and China Biology Medicine disc (CBMdisc). The literature search was conducted using a combination of subject terms and keywords.
Phase 2: Development of the test version
Delphi expert panel consultation
In October 2020, 10 experts participated in this study to assess the questionnaire, which qualified the requirements for an expert panel (8–12 experts). 21 The field of expertise of these 10 experts were: nursing education (n = 1), critical care (n = 4), and nursing management and critical care (n = 5). Experts were asked to evaluate the correlation between the items and the corresponding dimensions using a 5-point Likert scale (l = very irrelevant; 2 = irrelevant; 3 = general; 4 = relatively relevant; 5 = very relevant). “Modification Suggestions” and “Supplement Items” columns were set up in the table to obtain the inputs of experts for refining the expression of items. After receiving feedback from each round of expert consultation, the research team calculated the item selection indices and modified the content. Then, the revised questionnaire was sent to the experts for the next round of inquiry until the opinions of the experts tended to be consistent.
The item selection indices were determined using the critical value method, 22 including 3 indicators: the coefficient of variation (CV), the mean, and the full score ratio. The above 3 indicators were calculated for each item based on the scores of the experts. The threshold value of CV was calculated as “mean + standard deviation.” If the CV value of a particular item was less than the corresponding threshold value, the item was considered acceptable. The mean and full score ratio threshold values were calculated by “mean − standard deviation.” Accordingly, for mean value and full score ratio value, if the value of a particular item was more than the corresponding threshold value, this item was considered acceptable. Items that did not fit 2 or more indicators simultaneously were deleted.
Readability pilot testing
After consulting with experts, we selected a purposive sample of 20 critical care nurses from a comprehensive hospital in Wenzhou, China, to evaluate the readability and semantic clarity of the items. The respondents were asked to provide suggestions for revising any ambiguous content. The feedback received was then incorporated to form the test version of 17-item questionnaire.
Phase 3: Development of the final version
Participants and setting
A cross-sectional design was used in this phase. A convenience sample of critical care nurses was recruited from 6 cities in Zhejiang Province, China, between November 2020 and January 2021. Inclusion criteria: (a) registered nurses; (b) experience of working in the ICU; (c) provision of written informed consent for participation in this study. Exclusion criteria: (a) Pediatric ICU nurses; (b) nurses who are not on duty because of further study, sick leave, personal leave, or other reasons. Two weeks later, 30 critical care nurses who had participated in the survey were randomly selected to fill in the instrument again to evaluate the test-retest reliability.
Sample size
Based on the recommendations for adequate sample size, exploratory factor analysis (EFA) could be conducted in more than 20 respondents per item, 23 while confirmatory factor analysis (CFA) required more than 300 respondents. 24 Besides, factoring a dropout rate of 20%, at least 408 participants (17*20*1.2) were required. Finally, 432 critical care nurses were invited to complete the questionnaire.
Data analysis
SPSS Version 25.0 (IBM Corp., Armonk, NY, USA) and Amos 23.0 programs (IBM Corp., Armonk, NY, USA) were used for data analysis. Item analysis was conducted first, and then reliability and validity of the IDCQ were tested. The validity of the IDCQ was evaluated with tests of content validity and structure validity. Content validity was assessed based on experts’ scoring in the second round of the expert consultation, using the following indicators: item-level content validity index (I-CVI) and the average scale-level content validity index (S-CVI/Ave). The I-CVI was calculated as the number of experts who awarded a rating of 4 or 5 for a particular item divided by the total number of experts. S-CVI/Ave was the average of all I-CVIs. Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were performed to assess the structural validity of the IDCQ. Before conducting EFA, the Kaiser–Meyer–Oklin (KMO) test and Bartlett test of sphericity were performed. Cronbach’s alpha coefficient was calculated to assess internal consistency reliability. The 2-week test-retest reliability was assessed using intraclass correlation coefficient (ICC).
Ethical consideration
This study was reviewed by the Ethics Committee (Issuing number: 2020–208) [details omitted for double-anonymized peer review]. Written informed consent was obtained from all participants prior to their enrolment. In addition, the questionnaire was anonymous.
Results
Phase 1: Development of the preliminary version
Based on the conceptual model and systematic literature review, we combined all the items and deleted the duplicates to create a 19-item questionnaire encompassing three dimensions: shared humanity (10 items), personal narrative (5 items), and autonomy (4 items).
Phase 2: Development of the test version
Delphi expert panel consultation
According to the experts’ first-round evaluation scores and revision suggestions, we calculated the item selection indices (CV < 0.24, mean > 4.30, full score ratio > 52.98%). Based on these indices, two items (Item 1 “I provide undifferentiated care to all patients regardless of age, ethnicity, illness, wealth, or social status” and Item 6 “I talk about patients or their families behind their backs”) were eliminated. One item (“I care for the patient’s surroundings, such as lighting and noise”) was added to the “shared humanity” dimension. In addition, the expressions of some items were modified based on expert suggestions. The revised questionnaire, including 3 dimensions and 18 items, was resent to experts for evaluation. After the second-round of expert consultation, the item selection indices were recalculated (CV < 0.20, mean > 4.40, full score ratio > 70.79%), and one item (Item 13 “I am bored with the request of patients or their families”) was deleted. As per the experts’ suggestions, we also modified the descriptions of some items in this round. After the completion of this round, the coefficient of variation for each item was small.
Readability pilot testing
All the 20 respondents affirmed that the content of the questionnaire was easy to understand. The time required for filling the questionnaire was 3–6 min. Thus, the test version of the questionnaire was formed with 3 dimensions: shared humanity (9 items), personal narrative (4 items), and autonomy (4 items).
Phase 3: Development of the final version
Eventually, of the 432 questionnaires, 392 were valid. The valid response rate of the questionnaire was 90.74%.
Item analysis
The results showed that the total correlation coefficients of all items were greater than the cutoff value of 0.4. 25 The critical ratio showed good discrimination ability of the questionnaire (p < .01). As for internal consistency, the overall Cronbach’s alpha coefficient of the questionnaire decreased after removal of each item individually. Based on these results, all items were retained.
Construct validity testing
Findings of exploratory factor analysis.
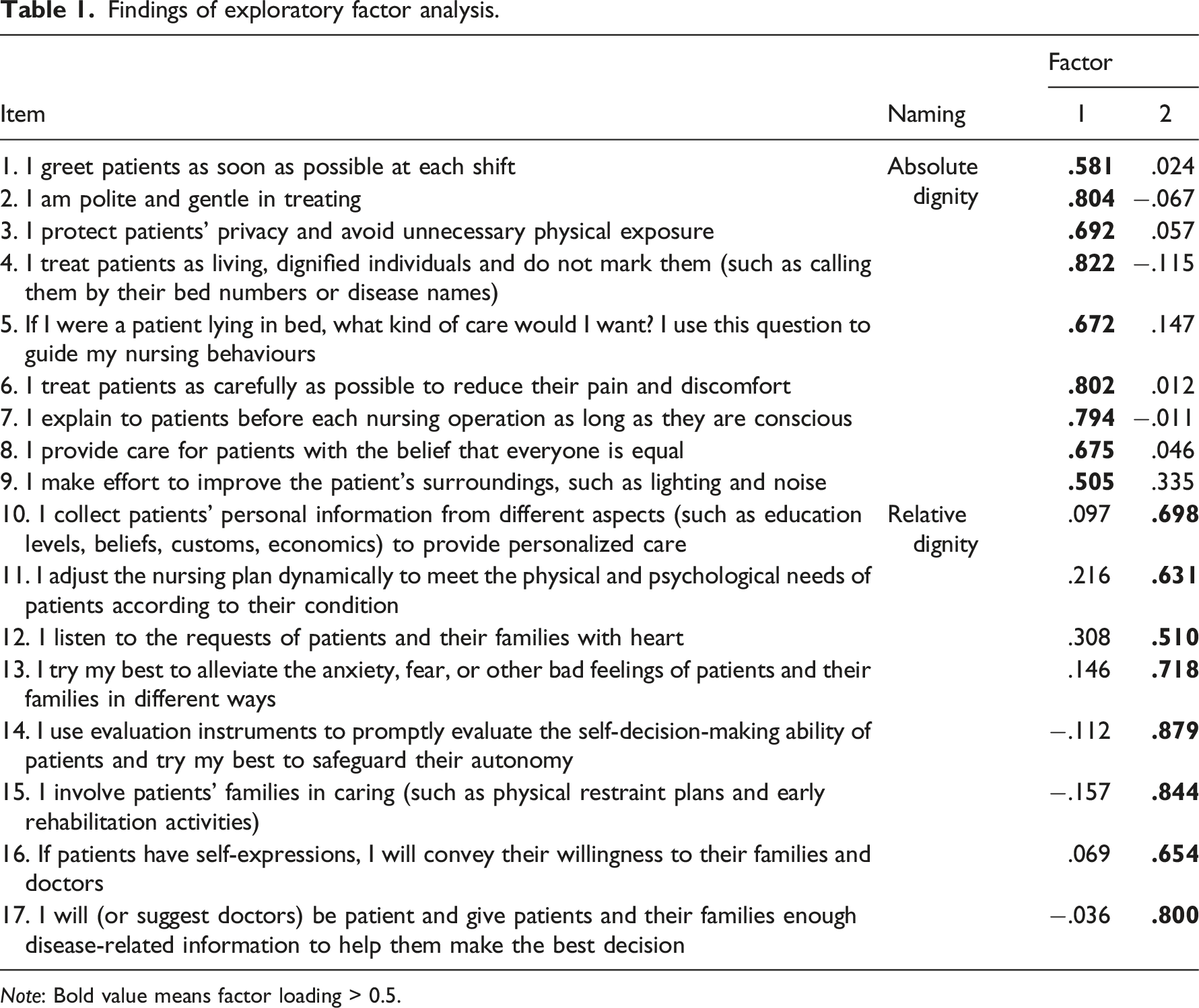
Note: Bold value means factor loading > 0.5.
To further validate the factor structure of the instrument, the bootstrap technique with maximum likelihood estimation was used to conduct CFA. The results obtained were as follows: χ
2
/df = 2.644, GFI = 0.912, NFI = 0.932, IFI = 0.956, CFI = 0.956, RMSEA = 0.065, SRMR = 0.0421 (Figure 2). The standardized factor load of each item ranged from 0.583 to 0.845. The average variance extracted for the “absolute dignity” and “relative dignity” dimensions were 0.543 and 0.581, respectively. The composite reliability of the above dimensions was 0.914 and 0.917, respectively. All the goodness-of-fit indices met the recommendations of the literature: χ
2
/df < 5, GFI > 0.9, NFI > 0.9, IFI > 0.9, CFI > 0.9, RMSEA < 0.08, SRMR < 0.08,31–33 indicating good model fitting. Finally, the final version of the questionnaire was developed with 2 dimensions: absolute dignity (9 items), relative dignity (8 items). Standardized path coefficient diagram of the questionnaire.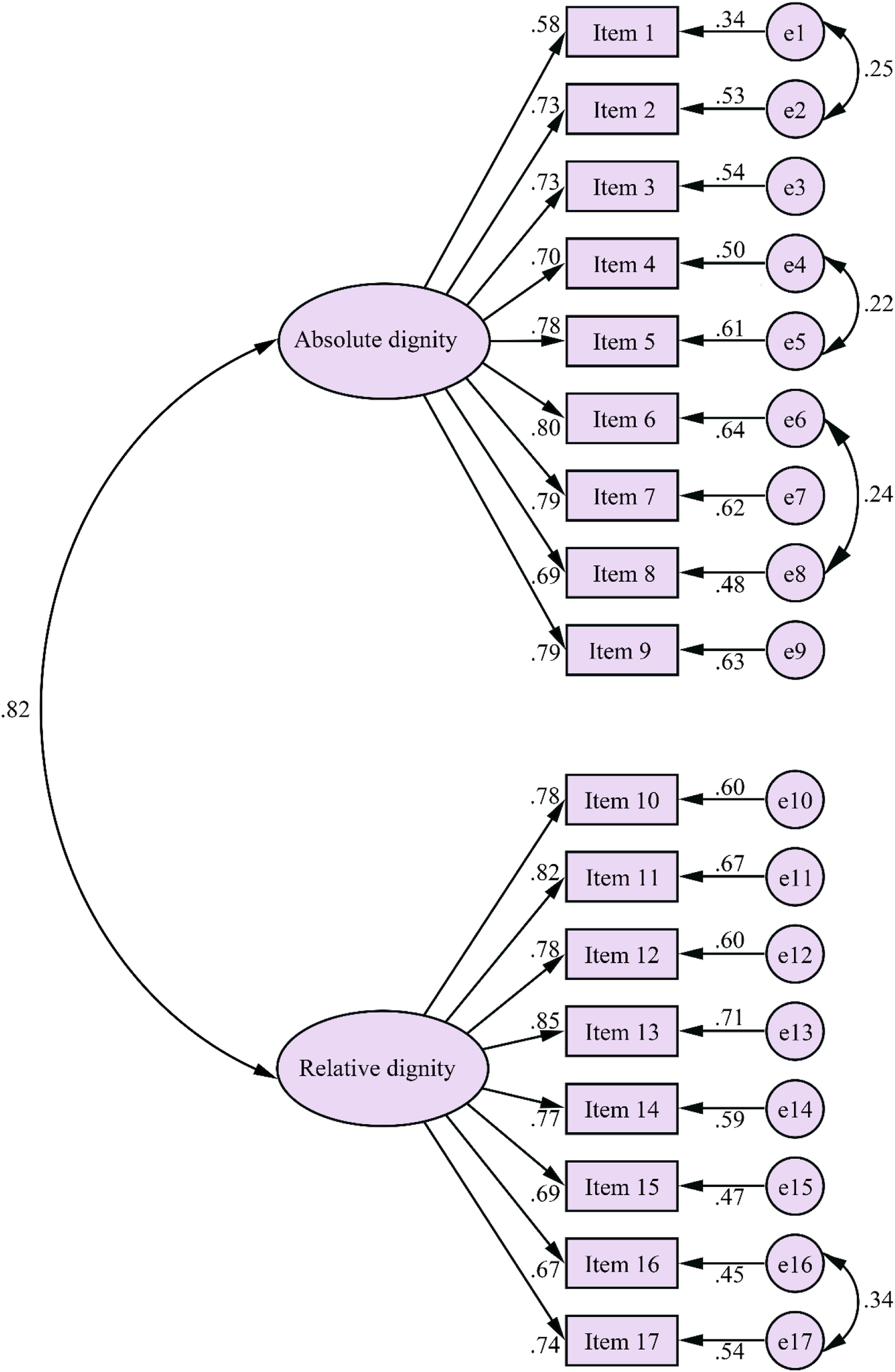
Content validity
The I-CVI of each questionnaire item ranged from 0.80 to 1.00, and the S-CVI/Ave of the questionnaire was 0.98, both exceeding the recommended value (I-CVI > 0.78, S-CVI/Ave ≥ 0.90). 34
Reliability testing
We calculated Cronbach’s alpha coefficient and ICC to measure internal consistency reliability and test-retest reliability, respectively. The Cronbach’s alpha coefficients of the questionnaire were 0.94 (overall), 0.91 (absolute dignity), and 0.92 (relative dignity), which were considered satisfactory. 35 The 2-week test-retest reliability index ICC of the total questionnaire was 0.88 (95% confidence interval was 0.75–0.94), surpassing the cut point of 0.7. 36
The final version of IDCQ
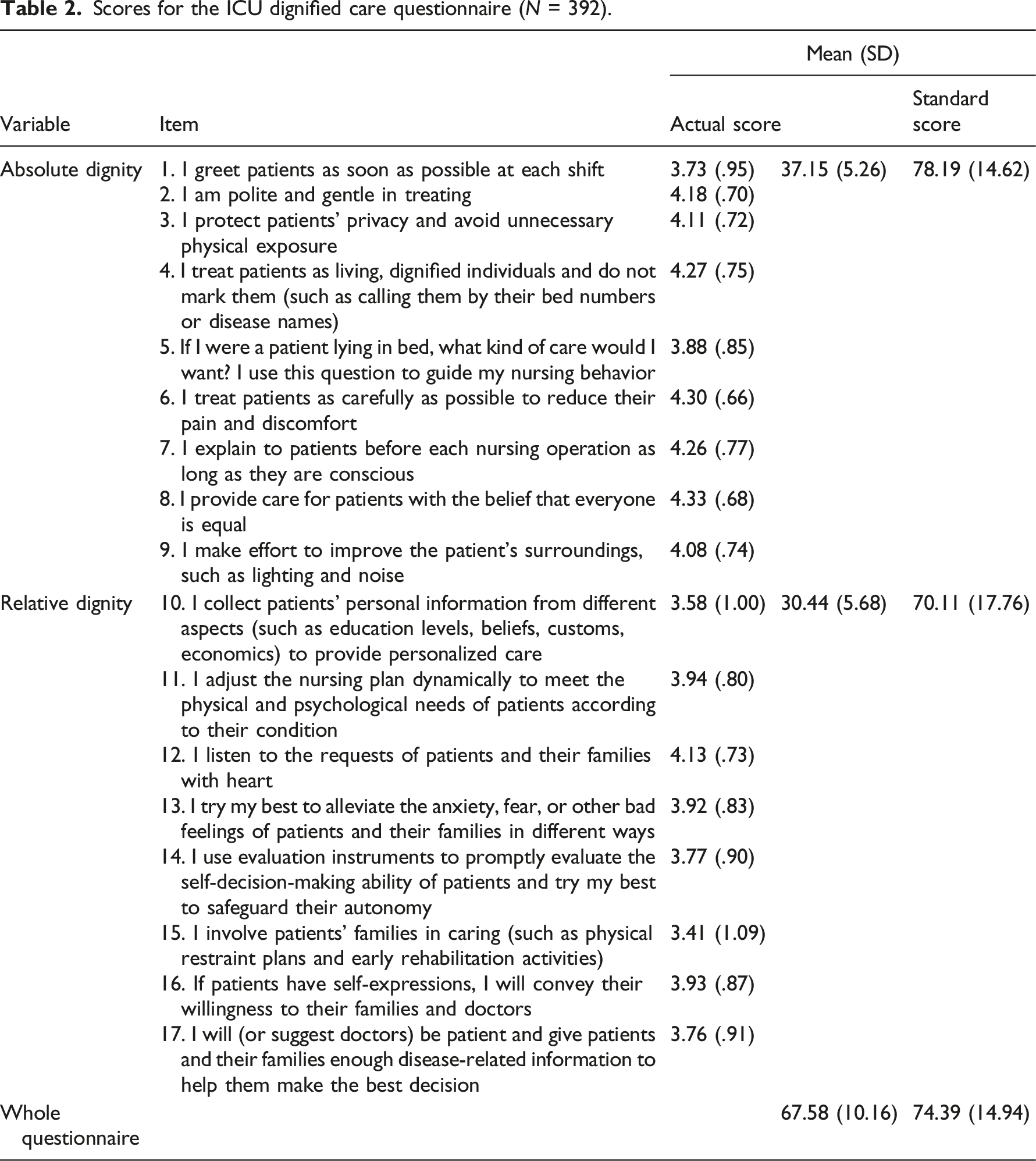
This study eventually developed the IDCQ with 17 items and 2 dimensions of “absolute dignity” and “relative dignity.” Each item was assessed using the 5-point Likert scale (1–5 stands for “never” to “always”) (Supplementary Table). The total score of the questionnaire ranges between 17 and 85 points. Critical care nurse’s behaviors of dignified care are assessed according to the standard score. Standard score = (actual score – theoretical minimum score)/(theoretical maximum score – theoretical minimum score) × 100, with a standard score of ≥80 indicating good behavior, 60–79 indicating intermediate, and <60 indicating poor behavior. 37 Higher scores on this questionnaire represent greater respect provided by the critical care nurses to patients.
Scores for the ICU dignified care questionnaire (N = 392).
Discussion
We strictly followed the protocol 38 to develop a novel instrument-IDCQ, which consisted of two dimensions, absolute dignity (9 items) and relative dignity (8 items). Our findings did not strictly follow the three theoretical dimensions of the original research hypothesis. However, there is no contradiction between the two.
Though the terms used in the literature,2,28,29,39–42 are not entirely consistent, dignity often can be divided into two sub-categories: absolute dignity and relative dignity. According to literature, everyone has absolute dignity simply because they are human. Absolute dignity, also called universal, human, basic, or intrinsic dignity, stresses the value and meaning of the existence of each person’s life. Maintaining absolute dignity requires that nurses treat each patient as a valuable being with basic respect rather than as an object of illness. Relative dignity, also called acquired, social, personal, or inflorescent dignity, varies from person to person. This implies that people from different sociocultural contexts may have different understanding of dignity. 42 Therefore, nurses should endeavor to provide personalized care in order to maintain the patient’s relative dignity. In this study, items 1–9 in the theoretical model dimension of “share humanity” address greetings, courtesy, privacy protection, and general care, reflecting respect for the value of life, which is consistent with the connotation of maintaining the patient’s absolute dignity. Similarly, “personal narrative” (Items 10–13) and “autonomy” (Items 14–17) in the initial theoretical dimensions focus on the patient uniqueness, aiming to provide individualized patient-centered dignified care, which is in line with the implication of preserving the patient’s relative dignity. Therefore, combining the results of EFA, we integrated the original dimensions of “personal narrative” and “autonomy” into “relative dignity.” Correspondingly, the dimension of “shared humanity” was renamed as “absolute dignity.”
We first examined the construct validity of the questionnaire by EFA. The results showed that two factors accounted for 62.804% of the total variance, which exceeded the acceptable value of 50%. 43 Each item had a high loading on the factor to which it attributed. To further demonstrate the construct validity of the questionnaire, CFA was used for analysis. The goodness-of-fit indices of the model were acceptable. The results of CFA showed that the standardized factor loading of each item was >0.5, the average variance extracted was >0.5, and the composite reliability was >0.8, which qualified the requirements. 44 These findings indicated acceptable convergent validity of the questionnaire.
Reliability refers to the consistency and stability of test results. Better reliability implies less chance of a random error in the measurement. In this study, the overall Cronbach’s alpha coefficients and that for each dimension were all >0.9, indicating that IDCQ has good internal consistency reliability. Furthermore, the ICC of the total questionnaire was 0.88 after 2 weeks, suggesting that the questionnaire had good reliability and stability across time.
In terms of the scores for the IDCQ, participants showed a medium level of provision of dignified care for patients. Besides, the respondents reported that they performed poorly in maintaining patients’ relative dignity compared to absolute dignity. Although the study used a convenience sampling method, the survey results reflected, to some extent, the need for improving the level of maintenance of patient dignity by critical care nurses, especially relative dignity. ICU patients have different care needs and may have greater expectations regarding respect for their relative dignity. Previous study 45 also found some gaps between the patients’ expectations of dignity and their satisfaction with dignified care. More research is needed to use the IDCQ to investigate the level of critical care nurses’ behaviors in dignity-conserving care. In addition, the relationship between patient satisfaction and the extent to which nurses maintain relative dignity needs to be explored.
Limitations
The final version of the IDCQ was found to be valid and reliable. However, some limitations of this study should be considered. Firstly, there was a paucity of literature on maintaining the dignity of ICU patients. This may have limited the generation of item pool in this study. Secondly, all critical care nurses who participated in this cross-sectional survey were from the same province in China. Thus, the results may be interpreted in a specific sociocultural context. The generalizability of the IDCQ needs to be further assessed in other regions and countries. Last but not least, the IDCQ is an instrument measuring behavior frequency of critical care nurses in dignified care. It may not always fully reflect the desirable situation of dignified care because frequent care is somewhat discrepant from the patients’ demands. Further research is needed to examine these gaps.
Conclusions
This study developed a reliable and valid instrument (IDCQ) with 17 items and 2 dimensions to assess the dignified care for critical care nurses. Dignity is an essential element in nursing care. Every patient deserves to be treated with respect, even in critical illness.
The IDCQ can help critical care nurses to conduct self-assessment of their behaviors in dignity maintenance. Improvements can be made in areas where they are deficient, thus enhancing dignified care. Nursing managers can use the IDCQ as a tool for evaluating the quality of humanistic care in the ICU. It can help nursing managers to develop interventions to promote dignified care at the organizational level.
Supplemental Material
Supplemental Material - Intensive care unit dignified care: Development and validation of a questionnaire
Supplemental Material for Intensive care unit dignified care: Development and validation of a questionnaire by Andong Liang, Wenxian Xu, Yucong Shen, Yeqin Yang, Qiongshuang Hu, Zhenzhen Xu, Peipei Pan and Zhongqiu Lu in Nursing Ethics.
Footnotes
Acknowledgements
We would like to extend our deep gratitude to all experts for their assistance and guidance during this instrument development process. We also thank all ICU nurses who participated in the reliability and validity verification of the instrument.
Author contributions
AL was the main designer and investigator, collected and analyzed data, and wrote the first draft. WX, YS, and PP participated in literature review and data collection. QH and ZX revised the manuscript critically for important intellectual content, and intensive reading of the revised manuscript. ZL supervised the study, managed and coordinated the implementation. YY also supervised the study, helped with the design and guided the writing and revision. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was reviewed by the Ethics Committee in Clinical Research of the First Affiliated Hospital of Wenzhou Medical University (Issuing number: 2020–208). Participants provided written informed consent before filling in, and the questionnaire was anonymous.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.