
Abstract
Background:
Determination of the factors affecting missed nursing care and the impact of ethical leadership is important in improving the quality of care.
Aim:
This study aims to determine the missed nursing care and its relationship with perceived ethical leadership.
Research design:
A cross-sectional study.
Participants and research context:
The sample consisted of 233 nurses, of whom 92.7% were staff nurses and 7.3% were charge nurses, who work in three different hospitals in Turkey. The study data were collected using a personal and professional characteristics data form, the Missed Nursing Care Survey, and the Ethical Leadership Scale.
Ethical considerations:
The study was approved by the non-interventional ethics committee of Dokuz Eylül University Ethics Committee for Noninvasive Clinical Studies. All participants’ written and verbal consents were obtained.
Findings:
The most missed nursing care practices were ambulation, attending interdisciplinary care conferences, and discharge planning. According to the logistic regression analysis, sex, the number of patients that the nurse is in charge of giving care, the number of patients discharged in the last shift, and satisfaction with the team were determined as factors affecting missed care. No significant relationship was found between ethical leadership and missed nursing care (p > 0.05), and a weak but significant relationship was found between the clarification of duties/roles subscale and missed nursing care (r = −0.136, p < 0.05).
Discussion:
Ethical leaders should collaborate with policy-makers at an institutional level to particularly achieve teamwork that is effective in the provision of care, to control missed basic nursing care, and to organize working hours and at the country level to determine roles and to increase the workforce.
Conclusion:
The results of this study contribute to the international literature on the most common type of missed nursing care, its reasons, and the relationship between the missed care and ethical leadership in a different cultural context.
Introduction
The International Council of Nurses (ICN) calls nurses on carrying out safe, individualized, and holistic nursing care in every condition. 1 However, today, nurses face many challenges, such as the ever-changing practices and policies in healthcare settings, increase in the number of patients, shortage of nurses, working hours, and uncertain roles.2–4 These challenges directly affect job satisfaction, moral distress, and patient care.5,6 These conditions lead to difficulties and also prioritization of nurses’ care activities. 7
Missed nursing care is an important indicator in determining the quality of nursing care and ensuring patient safety. 8 The concept of missed nursing care, which was first coined by Kalisch 9 was defined as partial or total neglect or delay of the necessary patient care. In the study, in addition to defining regularly repetitive missed nursing care, cases that caused missed nursing care were also explained. The missed nursing care practices in the literature10–13 were observed to be similar to practices described by Kalisch. 9 Saqer and AbuAlRub 10 and Bragadóttir et al. 8 reported that missed care usually stemmed from labor-related reasons. Verrall et al. 14 identified three themes for missed care in a qualitative study. These themes were increasing demands that cause reduced patient care time, ineffective methods in determining the number of staff, and an inadequate number of workers. In a study conducted in Sweden, 75% of the nurses reported that they had not been able to give at least one care in their last shift due to the lack of time. While nurses working day shifts report more missed care than those working night shifts, the decrease in the number of nurses has been found to cause more missed care. 12 Bragadóttir et al. 8 stated that nurses who worked in intensive care units, who were young, and who worked in places where there was good teamwork reported less missed care. Similar to the studies in the literature, a systematic review including 18 studies reported that the most missed part of care included patient ambulation, assessment of newly admitted patients, preparation of care plans, oral care, attending interdisciplinary care conferences, and documentation of nursing care. In the study, 75% of the nurses reported missed care, and missed care was found to increase when the number of nurses was low. 15 In a study involving 160,930 patients with heart failure in 419 acute care hospitals in the United States, more missed care and more readmissions were found in hospitals with poor working conditions. 16 According to studies in the literature, missed nursing care also negatively affects patient satisfaction. 13
Patient care is influenced not only by the individual decisions of nurses but also by features such as institutional support, management characteristics, and cultural variables.17,18 Therefore, it is necessary to investigate factors associated with missed nursing care in different cultures. The complex structure of the health sector, rapid developments in information technologies, and the pressure on employees for the increase in productivity increase the need for a managerial approach in the realization of ethical practices.19,20 Today, making ethical decisions that promote the safety and well-being of patients in these healthcare settings is more challenging than ever. 21 Institutions need dynamic nurse leaders to improve ethical decisions and patient outcomes. 4 While there are studies showing missed nursing care in the literature, there are very few studies examining the effect of leader characteristics on it. 4,22–24 Therefore, it is necessary to investigate factors associated with missed nursing care in different cultures.
Theorical framework
In our country, which has switched to performance-based healthcare services, the increase in the number of patients, the pace of hospitalization and discharge, the worsening working conditions, and the decline in public health services significantly affect the right of patients to receive quality healthcare.25,26 This health reform has led to increased workload, reduced patient time, and decreased quality of healthcare services. 25 These difficulties encountered by Turkish nurses in practice make it difficult for them to adhere to ethical principles in care.18,26 In addition, the low number of nurses, low job satisfaction, inadequate social rights, lack of voice, and uncertainty in role and job definition cause burnout and reduced job satisfaction.5,6 Under these conditions, institutions’ need for ethical leaders who, with a systemic perspective, show respect for patients and employees, value them, and are role models in line with human-oriented goals rather than pursuing financial and task-oriented goals has grown even more.24,27 In our country, Özden et al. 6 found that as nurses’ perceptions of ethical leadership increased, their ethical climate and job satisfaction also increased. Ethical leaders can have effective power in providing an environment where ethical decisions are made in care, nurses are empowered, and quality patient care is provided by creating a care-oriented ethical climate.18,28 On the contrary, ethical leadership has also been associated with ethical value systems that affect nurses’ patient care by contributing to job satisfaction. 29
Ethical leadership is the demonstration of normatively appropriate behaviors in one’s practices and relationships with other people and encouragement of other individuals through communication. 30 Ethical leadership also includes a commitment to ethical principles, and fairness and empathy in behaviors. 31 Brown and Treviño 32 stated that social learning theory provided a theoretical background to examine the relationships between ethical leadership and employee behavior. According to this theory, managers who exhibit ethical behaviors are role models for their employees. Ethical behaviors of managers also affect the behaviors of employees in this regard. 33 It is possible that appropriate behaviors of ethical leaders as role models in institutional terms can develop the self-belief of individuals in their skills and self-motivation of employees. Accordingly, if the ethical leader supports and encourages people who practice ethical care, observers will be more likely to adopt that behavior. 33 De Hoogh and Den Hartog 34 carried out a study parallel to Brown and Trevino’s definition of ethical leadership. Accordingly, ethical leaders encourage and reward ethical behaviors, and clarify responsibilities. In addition, Resick et al., 35 in their comprehensive study, defined the six basic characteristics of ethical leadership as “character and honesty, ethical awareness, community/individual-oriented, motivation, empowerment, and ethical responsibility management.” Accordingly, ethical leaders set ethical standards and determine ethical behavior expectations by considering the collective interests of the group. In this regard, ethical leaders, who should make sure that appropriate nursing care is offered in their clinics, can take the first step to ensure the “first, do no harm to patients” principle by creating a working environment where missed nursing care is discussed in a transparent manner. On the contrary, ethical leaders can prioritize not only medical care (patient assessment, glucose monitoring, and intake/output monitoring) but also basic nursing care such as ambulation and patient education, by setting goals in line with ethical professional principles and values in providing care. 4 In other words, ethical leaders teach their employees how to think strategically because they ask “what is the most appropriate thing to do” when making decisions. 36
In the 21st century, with care services becoming more team-oriented and integrated, the responsibility of ethical leaders for organizing the healthcare team has increased, too. 3 Unfair leadership behaviors can lead nurses to refuse their care duties. 4 Parallel to this, individuals who are treated fairly and well by their leaders respond with greater effort in their jobs. 30 In this respect, ethical leaders can strengthen teamwork using their interpersonal relationships and eventually reduce missed care rates. 18
While incomplete care is an ethical issue in itself, its effects create many ethical dilemmas. Missed nursing care contributes to negative patient outcomes, moral problems, and burnout.
7
Investigating the problem of missed care and the factors contributing to it is important for both nurses and nurse managers to design and implement strategies to help eliminate and reduce the causes of “missed nursing care.” Therefore, we need to understand the ethical leadership characteristics and organizational structure that lead to meeting care needs.7,37 With this respect, we have not found any studies in the literature investigating the relationship between missed nursing care and ethical leadership. Aim: This study aimed to determine the relationship between missed nursing care and perceived ethical leadership.
Methods
Study setting and participants
The study used a descriptive and cross-sectional design. The population of the study consisted of 744 nurses working in the Surgical, Internal Medicine, and Intensive Care units of a university hospital (315), an education and research hospital (269), and a state hospital (160) between 1 April and 31 December 2019 in Turkey. These units, which did not include the outpatient clinic and remote treatment centers of the two hospitals, were chosen because patients receive long-term care. In the study, no sampling procedure was employed; instead, 233 nurses who agreed to participate in the study and who met the sample selection criteria were included in the sample of the study. According to the post hoc power analysis done with the G-Power application, the sample was found to have a 0.81 power and adequate size.
Instruments
Data were collected using three different forms: a Personal and Professional Characteristics Data Form, the Missed Nursing Care Survey, and the Ethical Leadership Scale.
The Personal and Professional Characteristics Data Form
This form was designed by the researchers in light of the literature. It consists of 22 questions about the socio-demographic and professional characteristics of nurses. The questions in the form assess demographic and working characteristics.
The Missed Nursing Care Survey
This scale was developed by Kalisch and Williams. 38 The Turkish validity and reliability study of the scale was carried out by Kalisch et al. 39 The scale consists of two parts. The first part determines missed nursing care needs, and the second part identifies the reasons for missed nursing care. Only the first part was used in this study. The first section consists of 24 items and has a 5-point Likert-type scoring system (always missed, frequently, occasionally, rarely, and never missed). Cronbach’s alpha value of the first part was found to be 0.936, and the overall test–retest coefficient was 0.95. Each item in Kalisch et al.’s 39 version is scored between 1 = rarely missed and 4 = always missed. The “never missed” option is not included in the scoring. The total score that can be obtained from the scale ranges between 24 and 96. High scores from the scale show increased missed nursing care. In our study, Cronbach’s alpha value of the scale was found to be 0.819.
The Ethical Leadership Scale
The Ethical Leadership Scale was developed by De Hoogh and Den Hartog. 34 Turkish validity and reliability study of the scale was conducted by Alkan, 19 and Cronbach’s alpha coefficient was reported as 0.965 (ethics and fairness = 0.961 (six questions), clarification of duties/roles = 0.945 (five questions), and power-sharing = 0.928 (six questions)). The scale consists of 17 questions and three subscales: ethics and fairness (6 questions), clarification of duties/roles (5 questions), and power-sharing (6 questions). In the scale, the options for each item are “1 = strongly disagree,” “2 = disagree,” “3 = undecided,” “4 = agree,” and “5 = strongly agree.” The lowest and highest total scores that can be obtained from the scale are 17 and 85, respectively. High total scores obtained from the scale indicate a positive increase in ethical leadership. 19 In our study, Cronbach’s alpha value of the scale was found to be 0.972. Sample items from the sub-dimensions of the scale are as follows: the ethics and fairness sub-dimension (My supervisor is sincere in his or her words); the clarification of duties/roles subscale (My supervisor explains the scope of authority of each group member; My supervisor explains priority duties clearly; My supervisor explains what he or she expects from each group member); and the power-sharing sub-dimension (My supervisor reviews his or her decisions according to the recommendations of his or her subordinates).
Study process
The data were collected through face-to-face interviews after the participants were given written information in their clinic. The participants were informed that participation in the study was voluntary, their names would not be taken, the data obtained would only be used within the limits of the study, and the information would be kept confidential. The participants were given both verbal and written instructions about how to fill out the Ethical Leadership Scale. They were informed that staff nurses were expected to respond to the scale considering the charge nurse in the clinic, and the charge nurse of the clinic was expected to respond considering the nurse manager of the hospital.
Data analysis
The data were analyzed using SPSS for windows 22.0 (Statistical Package for the Social Sciences) software package. In addition to descriptive statistical methods (frequency, mean, standard deviation, minimum and maximum values, numbers, and percentage values), Mann–Whitney U-test and Kruskal–Wallis test were used to compare the quantitative data. Spearman’s correlation analysis was used to determine the relationship between ethical leadership, ethical climate, and job satisfaction. 40 A multivariate logistic regression model was established using factors that were found significant in paired tests. 40 The mean Ethical Leadership Scale score was also used as independent risk factor as it was reported in the literature that it was likely to affect the missed nursing care and it was the variable of the study to be tested.18,24 Logistic regression analysis was used to evaluate the risk factors and the risk relationships between risk factors and paired results, and the estimates are presented with 95% confidence interval (CI). The Hosmer–Lemeshow test was used for the goodness of fit of the statistical model. A p value of less than 0.05 was considered statistically significant. 40
Ethical considerations
Institutional permission of the hospitals where the study would be conducted and permission from the non-interventional ethics committee of Dokuz Eylül University Ethics Committee for Noninvasive Clinical Studies were obtained (Issue: 2018/16-11). The study was carried out in accordance with the Helsinki Declaration Principles. The permission of the owners of the Ethical Leadership Scale and the Missed Nursing Care Survey was obtained. All participants’ written and verbal consents were obtained.
Results
According to the findings, the mean age of the nurses was 35.15 ± 7.76 years, 90.1% of them were female, 67.4% were married, and 37.8% were working in education and research hospitals. Also, 37.8% were working in intensive care units, 55.8% had more than 11 years of work experience, and 66.5% had an undergraduate degree. Of the nurses, 59.2% were found to choose the unit they were working willingly, and 92.7% were staff nurses.
Most of the nurses worked more than 30 h a week (96.1%) and in shifts (78.1%). The majority of them (85.4%) worked overtime—more than 12 h a week—and did not take any days off (81.5%) in the last 3 months. Besides, 76% of the nurses stated that they were not planning to leave the job, while 23.2% had the feelings of leaving the job with a frequency of 50%. Moreover, 38.6% of the nurses were in charge of more than 10 patients, and the mean number of patients they gave care in their last shift was 8.8 ± 7.38. The percentage of the nurses who were not satisfied with their current position was 55.8%, and 64.4% of them stated they were satisfied with teamwork. The rate of those who received training on caregiving was found to be 74.2%, while the rate of those who received training on ethical leadership was 43.3%.
According to the “missed nursing care” survey results of the participants, the most missed nursing care types were patient ambulation, attending interdisciplinary care conferences, participating in post-discharge planning, medication management after discharge, and responding to call signals. Table 1 shows the rates of other missed nursing care types.
Perceived types of missed nursing care (n = 233).
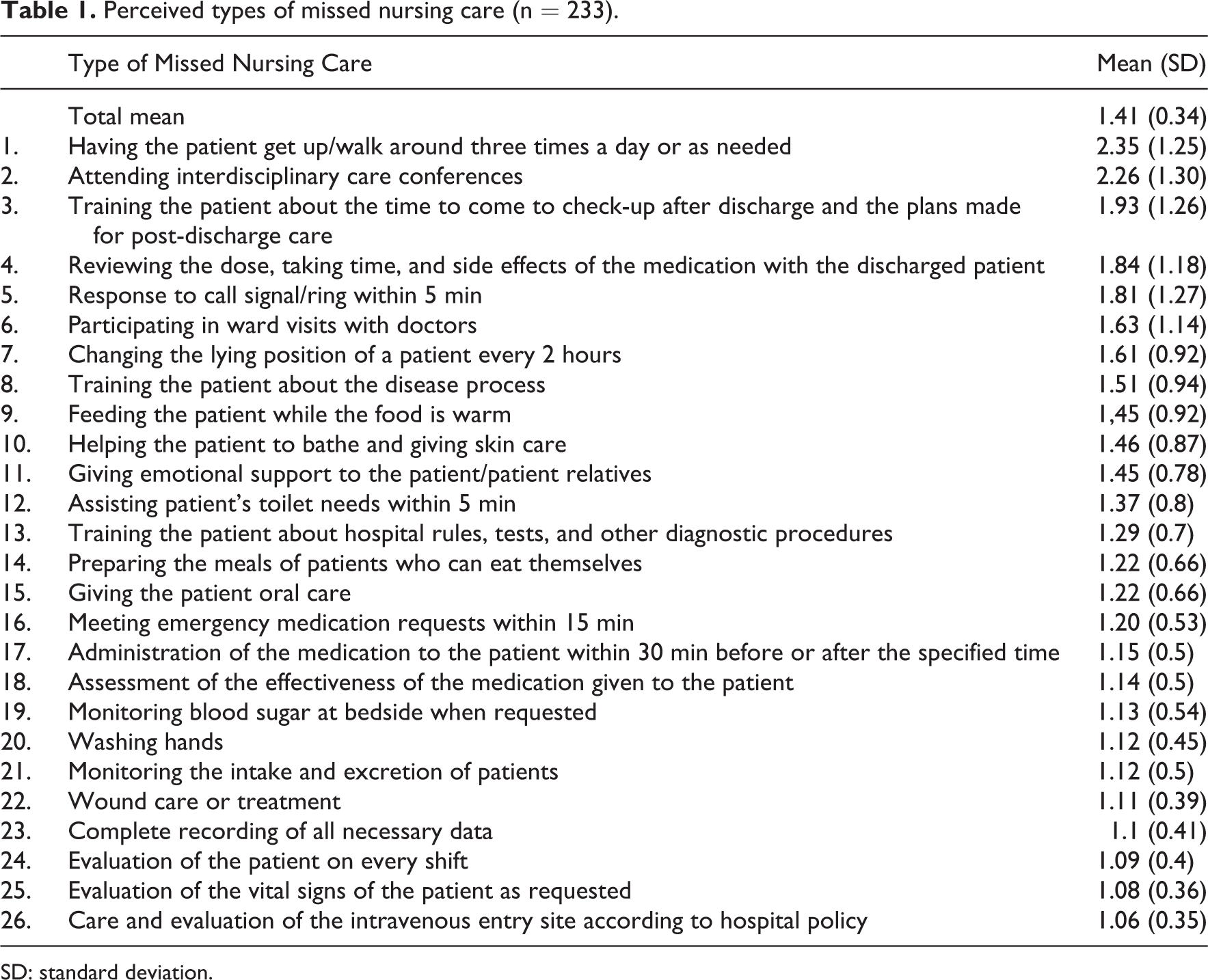
SD: standard deviation.
The mean ethical leadership score of the nurses was 60.18 ± 16.98. When the subscales of the ethical leadership scale were examined, the mean ethics and fairness subscale score was 20.91 ± 6.37, the mean clarification of duties/roles subscale score was 18.27 ± 5.28, and the mean power-sharing subscale score was 20.99 ± 6.20 (Table 2).
The mean scores of the nurses obtained from ethical leadership and its subscales (n = 233).

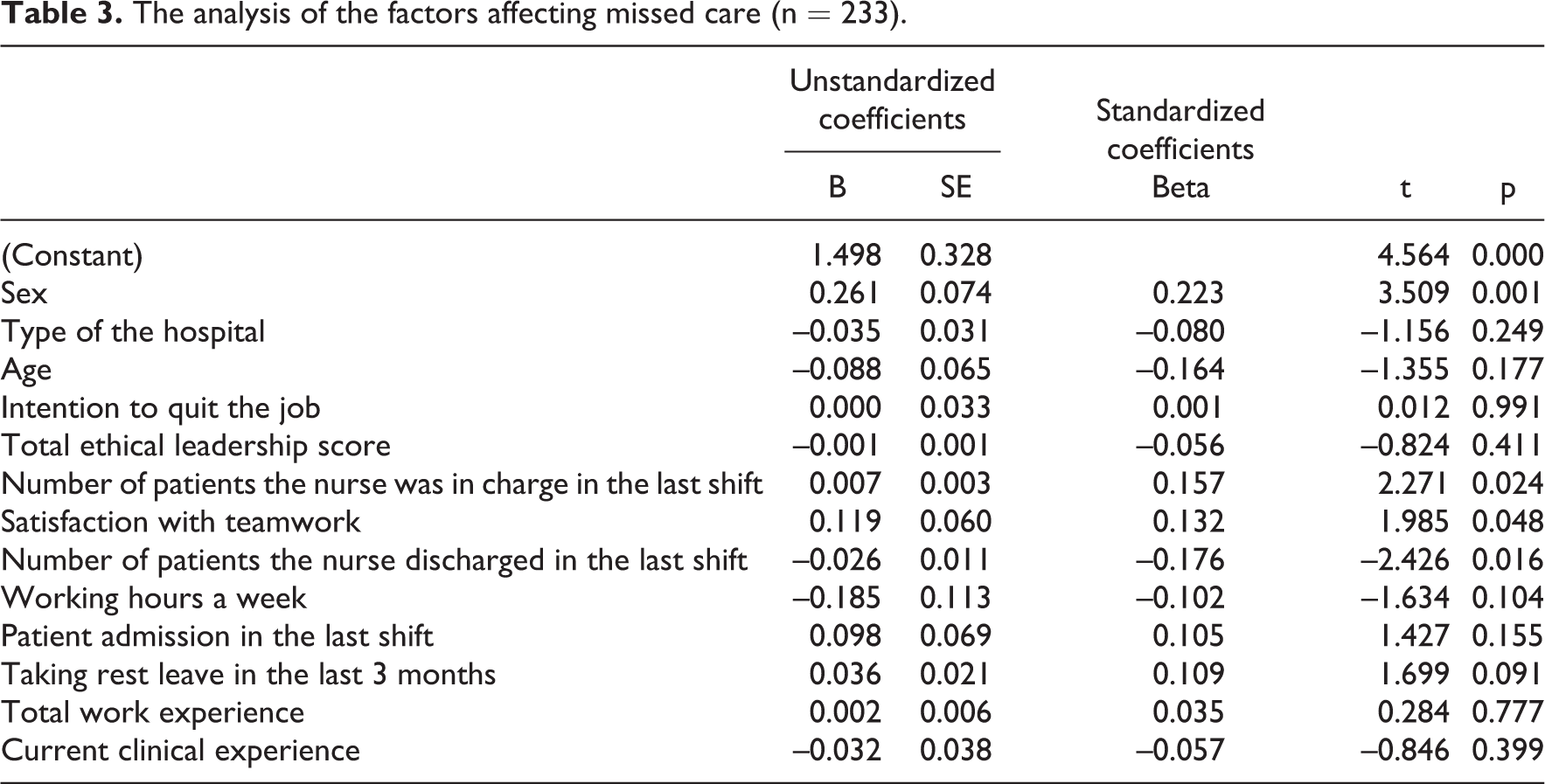
A multiple regression model was created to determine the nurses’ demographic characteristics, working characteristics, and the effect of ethical leadership on missed nursing care. According to this model, one or more variables had a significant relationship with “missed nursing care.” Variables that were significant in paired tests and thought to be theoretically significant were included in the model. According to the model, while the perceived missed nursing care was higher in nurses who were male and gave care to more patients in the last shift, it was less in nurses who had higher discharge numbers and were more satisfied with teamwork (Table 3). The model explained 16% of the variation in the “missed nursing care” level perceived through the common effect of all these variables. (F = 3.334, p < 0.001)
The analysis of the factors affecting missed care (n = 233).
According to the results in Table 4, no significant relationship was found between the means of the missed nursing care and ethical leadership total scores. A significant negative but weak relationship was determined between the clarification of duties/roles subscale of the Ethical Leadership Scale and the Missed Nursing Care Survey (p < 0.05).
The relationship between missed care and ethical leadership (n = 233).
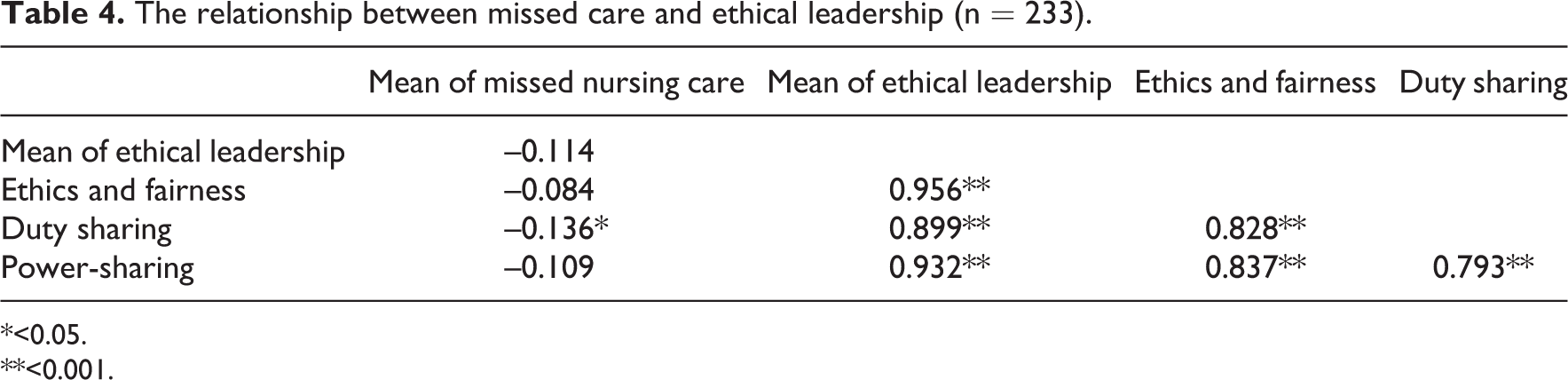
*<0.05.
**<0.001.
Discussion
According to the results of the study, the mean missed nursing care score was found to be at a medium level, similar to that of other studies in the literature. 10 Consistent with the literature, the three most frequently reported elements of missed nursing care were determined as ambulation, attending interdisciplinary care conferences, and making discharge planning.10,41–43 It was observed that nurses ignored the psychosocial aspects of nursing for routine jobs and prioritized the most urgent nursing duties. The reason why nurses cannot often meet these types of care may be due to not realizing their importance enough or lack of labor sources. In the study, increased number of patients provided care also increased the missed nursing care. Several studies in the literature clearly state that unplanned patient admissions, disruptions in daily work routines, unexpected increase in the number of patients, insufficient staff, and obligation to carry out support services are important factors in neglecting care.10,12,14,36,43–47 Bragadóttir et al. 8 stated that the excess number of patients given care in the last shift increased missed nursing care and that it decreased among nurses who thought that the number of staff was sufficient. Kalisch et al. 39 stated that the two most fundamental causes of missed nursing care in Turkey were lack of workforce and resources. Patient mobilization in Turkey is generally performed by patient companions. While one reason for the practice of patient accompaniment is that the relatives of the patient see accompaniment as a responsibility culturally, the other reason is the low number of nurses. 36 Nurse assistants are currently being educated to fulfill these missed care needs. 36 With this planning, less complex care practices can be assigned to nurse assistants and the burden of registered nurses can be reduced. However, these appointments are not enough to compensate for the inadequacy in the number of registered nurses in our country. Under these difficult conditions, ethical leaders who are responsible for both patients and their subordinates should clearly determine duties that nurses ignore doing and those which they cannot do due to lack of resources. If the reason for missed nursing care is inattentiveness, ethical leaders can raise awareness, for example, by monitoring negative consequences such as the increase in hospital stay and re-hospitalizations when ambulation is not provided. On the contrary, leaders can draw attention to the factors that contribute to missed nursing care both within the organization and at the policy level regarding the lack of resources, and accordingly, they can develop protocols and standards on the basis of units and at the country level. 24 Under the present conditions, nurses should be supported financially, and the number of nurses should be increased.4,20,48 The current guide of Health Quality Standards (2020) includes the titles such as the appointment of adequate personnel and provision of training for post-discharge care. 49 However, there may be a decrease in missed care if these inspections are carried out in a planned and steady manner in hospitals.10,50
Although discharge training is among the most frequently missed nursing care, missed nursing care was determined less in nurses who had a higher number of discharged patients. In the literature, the increase in discharge activities has been observed to increase missed nursing care. Winsett et al. 43 found hospitalization and discharge rates as 72%, which was considered as one of the important reasons for missed nursing care. Similarly, Blackman et al. 45 reported that high discharge activities were one of the important reasons behind missed care. In studies conducted in Turkey,46,47 unfulfilled and/or delayed practices among patient care practices carried out under current conditions have been found to be quite different from the list of missed nursing care practices reported in the literature. This situation has been observed especially in discharge procedures. The reason for the opposite result regarding discharge activities in our study may be due to the nurses’ view of the discharge as a decrease in the number of patients and therefore a decrease in the workload.51,52 Yıldırım et al. 47 found that the vast majority of nurses did not believe in the necessity of patient education and that more than half of the nurses did not provide patient education. 47 In studies conducted on reasons for ignoring discharge education, it was found that nurses did not take on educational roles in our country.53,54 In line with the contemporary educational role of nurses, providing discharge training with methods and techniques appropriate to the needs and characteristics of the individual/society is one of the responsibilities of ethical leaders in improving public health.3,55 For this reason, for the clarification of the duties of the team members related to the discharge process and for the nurse to take on an active role in this process, necessary institutional arrangements need to be made by ethical leaders. One of the tasks of ethical leaders is to increase and strengthen the level of employees’ knowledge, which can be accomplished by raising employees’ awareness of their roles through activities such as regular in-service training and following congresses.20,55
According to these results, the perceived missed nursing care was higher in nurses who were male. In the literature, no relationship was found between sex and missed nursing care in studies.44,56,57 Similar to our study, another study reported that missed nursing care was less common in female nurses.10,36 This result can be attributed to the adoption of caregiver roles by female nurses more in terms of gender roles.
Similar to our findings, several studies have shown that the stronger the collaboration within the team, the less missed nursing care is 58,59 Kalisch and Lee 58 and Bragadóttir et al. 8 also found that teamwork played an important role in missed nursing care. The appropriate communication skill of the ethical leader has been stated to be an important component in ensuring “satisfaction with teamwork,” which has been found as one of the reasons for missed nursing care in the literature. 32 More complex medical technology and healthcare systems require multidisciplinary teamwork in patient care. This increases medical errors and care expectancy in team-based care settings.60,61 Ethical leaders, who provide open and effective communication with the team, are stated to improve collaboration and empathy within the team.62,63 Gustafsson and Stenberg 22 expected leaders to provide a positive work environment where the entire team worked toward a common goal to ensure ethical care. A positive and valued work atmosphere provides a supportive work environment for nurses, and this warmth easily passes from the healthcare worker to the patient. Keselman 64 stated that ethical leaders needed to go beyond their own interests and focus on practices that benefit the whole group. Ethical leaders also increase employee commitment to the institution and job satisfaction by creating a harmonious and supportive work environment that shares common goals.6,17,21,55,65 Ethical leaders should attach importance to the health and motivation of nurses with their characteristics, such as empathy, motivation, and strengthening. 35 Çelik and Karaca 65 recommended that managers should use motivation tools, such as promotion and development in the profession, participation in team decisions, giving importance and value to the employee, and arrangement of appropriate working conditions, so that the motivation of nurses under the intense working conditions in our country could be ensured. Besides, training programs on teamwork and motivation can be organized to raise awareness of nurses on this issue.
In our study, the mean ethical leadership score was found at a medium level. This result is consistent with other studies in the literature.6,66 Also, some studies in the literature have found higher ethical leadership scores. 67 In our study, while there was no significant difference between the mean of the overall ethical leadership score and missed nursing care score, a weak and significant relationship was found with the clarification of duties and roles subscale. The finding of a significant relationship in this subscale can be explained by the expectations of nurses from their ethical leaders in clinical settings in Turkey. 5 Zhang et al. 68 also found a weak but significant relationship between ethical leadership and nurses’ patient-centered service behaviors. In this study, ethical leadership was found to have an effect on nursing services of specified roles, but it was determined to not have an effect on non-role nursing services. 68 These results show that further studies and analyses are needed on nurses’ expectations from ethical leadership in different cultures in future studies.
Clarification of nurses’ duties and roles in Gustafsson and Stenberg 22 was also one of the demands of nurses from their ethical leaders in their review on ethical leadership. Clarification of duties and roles includes the determination of clear communication by the ethical leader and promotion of ethical behaviors and clarification of the roles and responsibilities of healthcare workers. 19 In the Turkish healthcare system and hospitals, it is very common to witness role conflict and ambiguity among nurses because of a lack of understanding about what their specific role requires.5,25,69 Nurses who have to fulfill many tasks move away from patient care due to lack of time, are given every kind of responsibility, and have to interact with managers of various professions.2,20 To decrease the level of role conflict, ambiguity, and burnout level in nurses, serious efforts must be made to clarify role definitions, increase resources, and employ conflict management methods. 69 Therefore, even if the correlation of missed nursing care with ethical leadership total score is found to be weak, missed nursing care will not be prevented as long as employees work under difficult conditions with role uncertainties. At this point, ethical leaders can coordinate multidisciplinary teamwork with a proactive approach in providing high-quality care and patient safety, become more visible at the organizational level, and be stronger in identifying and defending roles.3,22,28,60,61,70
Limitations
Since this study is a survey study, the results are limited to the responses given by the nurses. Observational studies can be conducted to determine missed care. The study has limitations in terms of generalizability as it was carried out in hospitals located in the west of Turkey. However, the missed nursing care measurement tool also has some limitations. There is a need for a special measurement tool for Turkish culture that suits the nursing regulations and will assess the needs of different patient populations (such as intensive care, geriatrics, surgery, oncology) and care needs at the same time, including nursing roles at the national level. 36 Another limitation is the topics examined in the study. In one of them, the opinions of nurses about their leaders were asked, and their care responsibilities were questioned under the other topic. In the study, to make sure participants could supply responses with no hesitation, they were ensured that anonymity would be preserved, data such as names and clinics would not be shared with the management, and the data obtained would only be used for scientific purposes. To avoid the effect of other employees and managers on the participants, data were collected from each nurse at separate times.
Nurses may not have completed the open-ended responses because of the sensitivity of the leader topic, even though the anonymity was stressed by the researcher. In this regard, qualitative studies can be carried out in a cultural context regarding the expectations of nurses from their leaders in maintaining care.
Implications for practice and research
– Seminars should be organized for prospective nurses with leader nurses from different fields, such as intensive care, clinical services, pediatrics, and their caregiver roles in the new health system should be discussed.
– Nurse leaders should recognize the difficulties and ethical problems that nurses experience in meeting care at the clinical level and seek ways to support them.
– Levels of missed nursing care can be reduced by providing a good working environment, strengthening teamwork, and adopting appropriate policies regarding the healthcare staff role.
– Especially in the pandemic process such as Covid 19, it can be recommended to investigate the effects of ethical leadership, role uncertainties in institutions, and missed nursing care on nurses’ job satisfaction.
– Leaders can improve the standards of care in their clinics by raising awareness about the most missed nursing care, being a role model, identifying ethical standards, allocating resources and workforce, and monitoring the process constantly.
– It is important that training programs related to ethical leadership should be developed and leaders should receive training.
Conclusion
Good care consists of ethical elements with evidence-based, respectful, and dignified care. In the realization of good care, in addition to their responsibility to society, ethical leaders are responsible for maintaining the ethical and professional competence of care personnel and determining contextual, professional, and cultural preconditions that affect this. 21 This study investigated the most common missed nursing care and factors affecting it in three hospitals in the west of Turkey. Sex, the number of patients the nurse is in charge of, and satisfaction with teamwork were determined as factors affecting missed nursing care. While ethical leadership showed no significant relationship, the clarification of duties and roles subscale of the ethical leadership scale was found to be correlated with missed nursing care in the study. In this context, ethical leaders should have a say in the organizational dimension while defending the determination of the duties and roles of nurses in providing ethical care.19,20,63
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.